
Abstract
Childhood cancer survivors are at risk for ongoing health risks related to their initial treatment. One potential long-term complication following radiation is the development of secondary tumors, including peripheral nerve tumors, such as schwannomas. We present three adolescent and young adult (AYA)-aged survivors of pediatric cancer (22–40 years), followed in our AYA survivorship clinic. Each was found to have a schwannoma many years following total body irradiation for a childhood primary malignancy. We highlight a late effect of low-dose total body irradiation as well as the importance of long-term monitoring in this population.
Introduction
In the United States, there are more than 400,000 childhood cancer survivors. 1 This growing population of childhood cancer survivors are at risk for, and experiencing, late effects of their primary treatment as they age into adulthood. In 2014, the Childhood Cancer Survivor Study reported the cumulative incidence of severe, disabling, life-threatening, or fatal health conditions among survivors by the age of 50 as 53.6%. 2
Radiation therapy, one of the more commonly used treatment modalities in childhood cancer patients, is associated with significant late-term effects. Complications from irradiation include growth and development failure, gastrointestinal dysfunction, pulmonary and cardiac abnormalities, and secondary tumors. 3 The types of secondary neoplasms vary by radiation dose and field. One type of neoplasm seen in patients following radiation therapy is the schwannoma, a benign tumor arising from the peripheral nerve sheath. 4 Although they are typically benign, tumors of the peripheral nerve sheath have the potential of rapid growth and cause significant impingement on the nerve as well as surrounding structures. The standard of treatment when patients become symptomatic is surgical resection with negative resection margins as a prognostic indicator. 4
Most cases of radiation-induced schwannomas described in the literature are the result of localized low-dose radiation for tinea capitis or tonsillitis or, more rarely, high-dose radiation for a childhood malignancy. 4 In this report, we discuss the history, presentation, and management of three adolescent and young adult (AYA)-aged survivors of pediatric cancer who were found to have schwannomas between 2015 and 2017, following total body irradiation (TBI) for a childhood primary malignancy. These patients were followed in our AYA Survivorship Clinic at Tufts Medical Center (MC), which cares for patients, ages 18–39, having a previous diagnosis of cancer in childhood, adolescence, or young adulthood.
Case 1
A 34-year-old female presented to a routine follow-up appointment with new-onset dizziness and vertigo. Her medical history was significant for a diagnosis of standard risk acute lymphoblastic leukemia (ALL) at age 5 years that was initially treated with multiagent chemotherapy and central nervous system (CNS) prophylaxis with intrathecal therapy. While on treatment she relapsed and underwent reinduction therapy. Ultimately, she underwent an ex vivo purged autologous bone marrow transplant for which she received 14 Gy of fractionated TBI and high-dose chemotherapy. Post-transplant, she had stable trilineage engraftment and no evidence of disease. She was followed over the ensuing 25 years in survivorship care.
At the time of her AYA clinic visit, she described few months of history of dizziness, balance problems, and progressively muffled hearing on the left side. She was referred to otolaryngology where an audiogram demonstrated left-sided hearing loss. She subsequently underwent magnetic resonance imaging (MRI) and was found to have a 3.2 cm mass in the cerebellopontine angle with extension into the jugular foramen (Fig. 1A, B). She was referred to neurosurgery where it was determined her mass was most consistent with a glossopharyngeal schwannoma. Given her symptoms and the imaging results, she underwent a left suboccipital craniotomy for excision of her tumor.
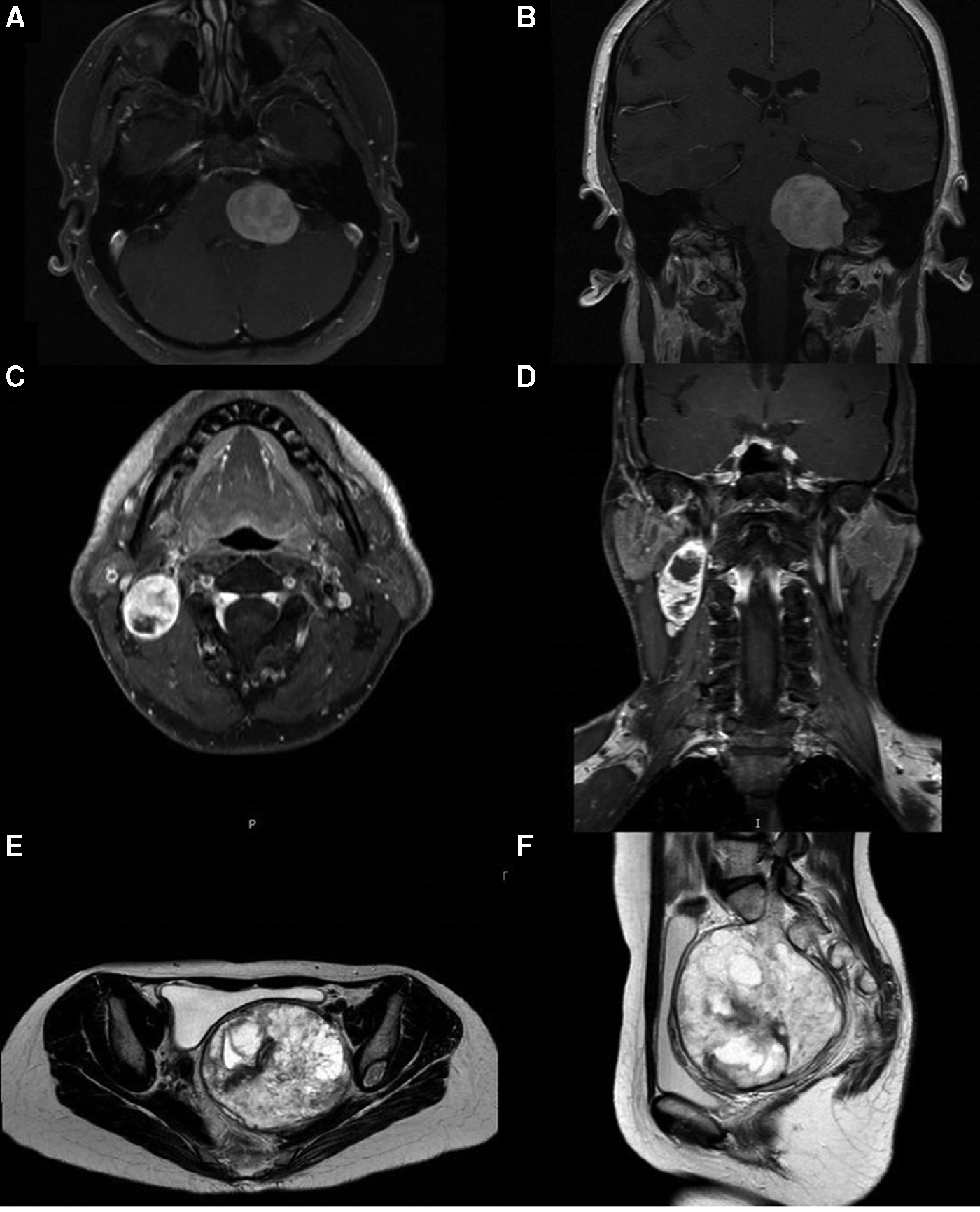
Magnetic resonance imaging of patients in case series.
Intraoperatively, a complete resection of the tumor was achieved. Pathological evaluation of the specimen with reticulin special stain showed a reticulin fiber distribution, consistent with a WHO grade I schwannoma (Fig. 2A). Immunohistochemical staining for S-100 was high and for Ki-67 was low, confirming these findings. Postoperatively, the patient's symptoms resolved and her hearing returned to normal baseline.
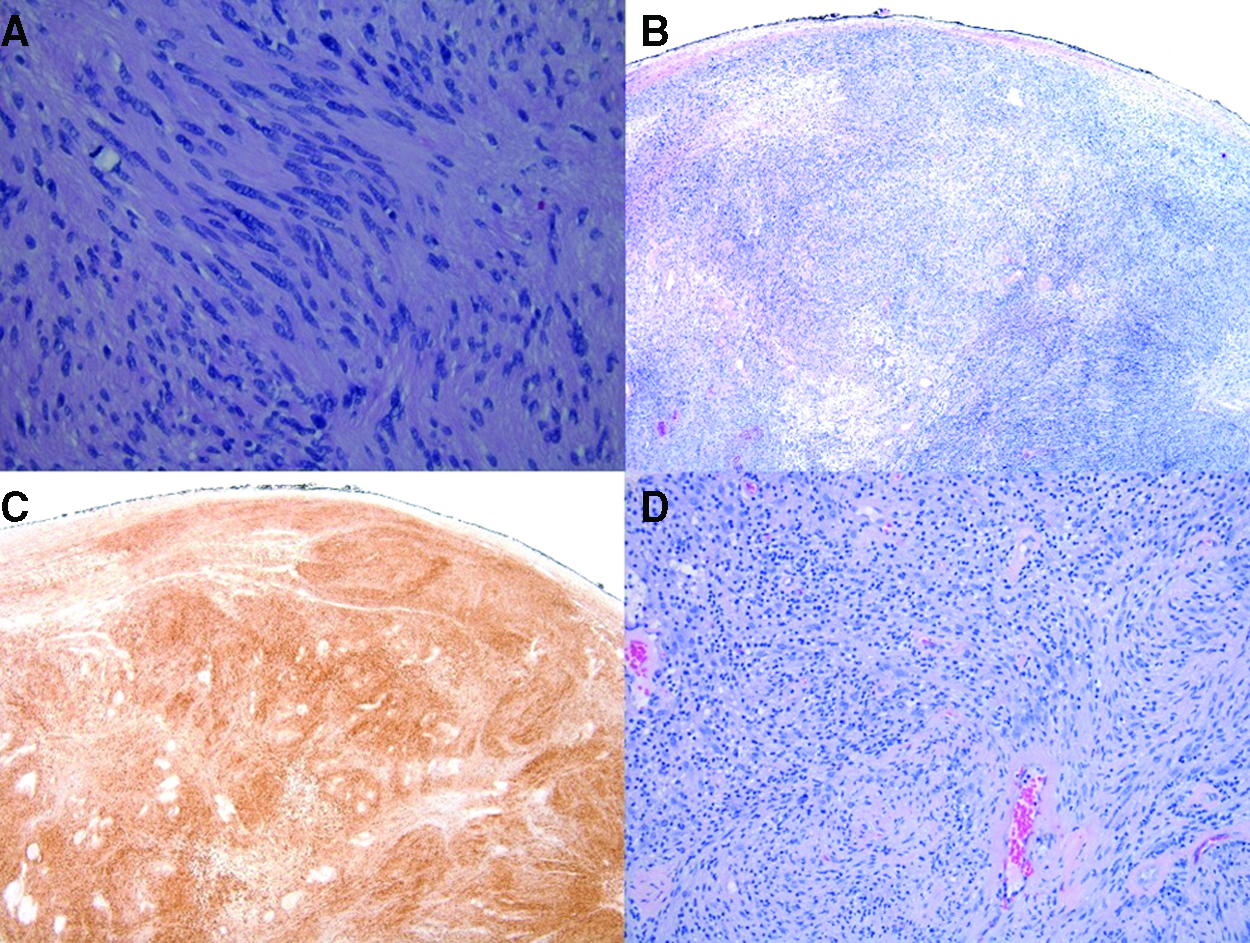
Pathology slides from patients in case series.
Case 2
A 40-year-old male presented to the otolaryngology department for an enlarging right-sided neck mass. His history was significant for a diagnosis of myelodysplasia with unfavorable cytogenetics at the age of 11 years, for which he received an allogeneic bone marrow transplant from his human leukocyte antigen-identical sibling. Given the results of cytogenetics that differentiated his aplasia as myelodysplasia from acquired aplastic anemia, he was treated with fractionated TBI of 14 Gy and high-dose cyclophosphamide.
One month before his appointment at Tufts MC, the patient noted a right-sided neck mass. On the advice of his primary care physician he underwent computed tomography (CT) scan at a regional hospital. Results from the CT scan were consistent with a parapharyngeal space mass. A biopsy was performed and appeared to be consistent with a benign schwannoma.
At the time of his presentation to Tufts MC, the mass was enlarging and was now inducing the sensation of pressure on his throat. After discussion of these findings, he underwent an MRI, which showed that the mass had increased in size ∼7 mm compared with the previous scan (Fig. 1C, D). Given his history and the rapid growth of the tumor, the patient opted to undergo resection of the tumor.
Intraoperatively, the nerve of origin of the tumor appeared to be the cervical sympathetic chain. It was inseparable from the mass and could not be dissected away, therefore it was clipped and divided. Immunohistochemical stains of the specimen were positive for S-100 protein and negative for HMB-45 and MART-1. This was consistent with a diagnosis of a WHO grade I schwannoma (Fig. 2B, C).
In the postoperative period, the patient was noted to have ipsilateral miosis without lid ptosis. He also developed first bite syndrome and underwent parotid Botox injections for relief.
Case 3
A 22-year-old female presented to the AYA clinic to re-establish survivorship care, following a 2-year hiatus. Her medical history was significant for ALL, diagnosed at age 2. She successfully completed initial treatment, consisting of multiagent chemotherapy and CNS prophylaxis with triple intrathecal therapy. Less than 2 years off therapy, she had a disease recurrence in both the bone marrow and CNS. Remission was successfully reinduced before proceeding to an allogeneic bone marrow transplant from her matched sibling. Her conditioning regimen included high-dose chemotherapy, 12 Gy of TBI, and a 6 Gy craniospinal boost.
She received intermittent follow-up care at her local institution and at the transplant center before transitioning to the AYA clinic. As part of her AYA-based survivorship care, she was referred to gynecology. At her appointment, she described stabbing left leg, calf, and foot pain that started 4 years earlier, but was progressively worsening and was reproduced with intercourse. On gynecological examination, she was found to have a large left-sided pelvic mass. She underwent an MRI that demonstrated a 9 cm pelvic mass appearing to arise off the S1 nerve root (Fig. 1E, F). She was evaluated by the neurosurgery department, which recommended a needle-guided biopsy. The final pathological diagnosis of the tumor was a spindle cell neoplasm of neural derivation, most likely representing a schwannoma.
Given these findings, resection of the tumor was recommended. Both neurosurgery and surgical oncology were involved in the case because of the extensive nature of the mass and its location. Intraoperatively, the tumor was found to be extremely vascular and fibrous, making the resection challenging. The tumor was debulked piece by piece with the bipolar down to the S1 nerve root and the remainder of the tumor was dissected from the root. During the procedure, she received four units of blood and two units of platelets. Estimated blood loss was 2.7 L. Immunohistochemistry staining of the specimen demonstrated strong immunopositivity with S-100 and low staining with Ki-67. Reticulin special stain was present in-between tumor cells supporting the diagnosis of a WHO grade 1 schwannoma (Fig. 2D).
In the postoperative period, the patient had mild residual numbness in her left foot but her leg pain improved.
Discussion
Radiation therapy is the cause of significant long-term side effects in childhood cancer survivors. 3 One such side effect, although rare, is the development of schwannomas. The three patients in our report were diagnosed as children with primary blood malignancies, two with ALL and one with myelodysplasia. All three patients received TBI as part of conditioning for a bone marrow transplant during treatment of their primary malignancy. Two of the patients received treatment with 14 Gy of irradiation, while one received 12 Gy of irradiation with a 6 Gy boost to the cranium and the spine. All three patients presented with deficits secondary to schwannomas many years into their survivorship (20–30 years). Interestingly, the schwannomas in each patient arose in different locations; one from the glossopharyngeal nerve sheath, one from a sympathetic cervical nerve sheath, and one from the S1 nerve sheath, highlighting the variability of presentation.
While low-dose radiation-induced schwannomas have previously been described in the literature, the majority of them were found in patients with local radiation for treatment of tinea capitis or tonisillitus.5–8 In a study by Ron et al., the authors reported on 10,000 children who received low-dose radiation for tinea capitis. The relative risk for developing a nerve sheath tumor was 18.8 when compared with general population controls and nonirradiated siblings, and the absolute risk of developing any neural tumor was 0.55%. 5 Although there have been cases described of radiation-induced schwannomas in the AYA population, the majority of patients had received high-dose local radiation. In a large systematic review by Yamanaka and Hayano, nine cases of radiation-induced schwannomas following radiation for a primary malignancy were described. 4 Of these patients, the lowest dose of radiation used was 24 Gy and the average dose was 43.7 Gy. The patient who received 24 Gy of radiation was a 23-year-old male, with an acoustic schwannoma, treated with combined radio- and multiagent chemotherapy, including intrathecal methotrexate and prophylactic radiotherapy to the neuroaxis, for treatment of his ALL when he was 15. In comparison with previously described cases, our series demonstrates that radiation, even at lower dose, can cause schwannoma formation throughout the peripheral nervous system in AYA-aged childhood cancer survivors.4,6
Of note, genetic diseases such as neurofibromatosis or, more rarely, schwannomatosis can predispose patients to schwannoma formation. Although none of our patients had formal genetic testing, neither their health history not family history suggested they may have a predisposing genetic disorder. 9
Although considered benign, schwannomas can lead to serious long-term complications, based on location. The deficits noted in our patients included hearing loss, airway impingement, and severe leg pain. Given the symptoms the schwannomas were causing, all three patients in the series opted for surgical resection. While complete surgical resection provides the best long-term outcomes in terms of recurrence, given the location of the tumors and the potential for invasion into crucial nearby structures, surgery poses a serious risk and complete resection often comes at a cost. While the tumors are considered benign, they can cause serious complications and treatment with surgery can result in long-term neurologic deficits.
Given the indolent growth of these tumors, it is difficult to ascertain when they began. In all three cases, the lesions were only diagnosed when they led to demonstrable symptoms. The patient in case 1 of our series was actively followed in our AYA clinic. During a routine follow-up appointment, she described her new symptoms and she was promptly referred to otolaryngology and neurosurgery. She was diagnosed and treated within three months of the onset of her initial symptoms. Had her history of TBI not been known or not been prioritized, her diagnosis could have been delayed and her outcome may not have been as successful. The patient presented in case 2 was followed locally by his primary care physician. The patient himself reached out to his original oncologist with whom he had maintained close contact for 30 years to inquire if there could be a possible link to his previous TBI and asking for assistance with a further evaluation. The patient discussed in case 3 had experienced symptoms for several years before her diagnosis was made. Fortunately, she followed the recommendation to see gynecology and the mass was identified. Had she followed up with the AYA clinic when pain persisted, it is possible that her symptoms would have been worked up to a greater extent given her known history of radiation exposure. Early identification of her tumor may have prevented the extensive tumor invasion and may have significantly reduced the risks encountered during her surgery.
Conclusion
This report highlights the detection of TBI-associated tumors after more than 20 years from initial exposure and argues for regular monitoring for long-term effects. Formal survivorship care enables us to actively engage these patients through education regarding their previous oncologic treatment and specific recommendations for ongoing surveillance.
Footnotes
Acknowledgments
The authors gratefully acknowledge the generosity of the Reid R. Sacco AYA Cancer Alliance for programmatic support.
Author Disclosure Statement
No competing financial interests exist.