
Abstract
Impaired fertility is one potential late effect of cancer, with 15% of adolescents and young adults with cancer (AYAC) at a high risk. Guidelines state that fertility advice should be available at diagnosis; however, research shows that this is not routinely provided. This can negatively affect patients' emotional well-being, mental health, and satisfaction with care. This review aimed to synthesize and critically evaluate studies investigating professionals' experiences of discussing fertility issues with AYAC patients and to understand the barriers and facilitating factors to having these conversations with this specific age group. Peer-reviewed qualitative and quantitative studies were identified by systematically searching eight databases. Fifteen articles reporting from 14 studies were included in the review. Participants reported patient, parent, professional, and institutional factors that influenced fertility discussions. The most commonly reported barriers were the lack of patient educational materials and staff training. Participants were more likely to discuss fertility with patients who were male; had less severe disease; and raised the issue of fertility themselves. The findings suggest that professionals' own values and opinions influence the likelihood of fertility being discussed, with implications for guidance and training. Further, institutional barriers lead to a lack of consistent provision for patients both nationally and internationally. A paucity of research looking solely at AYA populations was noted. A need for research comparing the experiences of different professional groups and exploring the extent to which reported barriers impact on fertility discussions was highlighted. There is also a need for higher-quality qualitative research adopting stronger methodology.
Introduction
In the United Kingdom, the rates of adolescent and young adult (AYA) cancer diagnoses and survival are increasing concurrently; thus there is a growing population of adult survivors experiencing late effects of cancer and/or cancer treatment. 1 It is estimated that between 50% and 90% of adult survivors of childhood cancer have at least one moderate to severe adverse health outcome, such as impaired fertility.2,3 Around 6% of all female childhood cancer survivors experience acute ovarian failure. 4 The risk of infertility brings decisions to be made around fertility preservation (FP) options and adds further complexity to decisions about cancer treatment since some FP options require delaying treatment. 5
The National Institute for Health and Care Excellence guidelines state that risk of infertility should always be considered by the treating oncologist, and fertility advice should be available at diagnosis. 3 Despite this, there is evidence that adolescents and young adults with cancer (AYAC) do not receive sufficient information about fertility or opportunities to discuss options and feelings about fertility; fertility counselling is not routinely offered to AYA cancer patients; and most adult survivors of childhood cancer are unaware of their fertility status before trying to conceive.6–8 Studies suggest that infertility can lead to an increased risk of emotional distress, and young cancer patients who are not given information about FP before treatment later report feeling angry, disappointed, overwhelmed, and distressed. 9
Researchers have found that adolescents want to be well informed and responsible for their own medical decisions.10,11 However, a Teenage Cancer Trust survey found that 37% of respondents felt they were involved in their treatment decisions “some” or “not much” of the time, and there are often discrepancies between patients', parents', and professionals' views on the extent of AYAC involvement in treatment decision-making.3,12 Studies show significant variation in the proportion of participants who judge fertility-related information received to be sufficient (11%–90%); some do not receive any, and in one study 95% of young people viewed the information they received as inconsistent or incomplete, with some having to raise the issue themselves.13–15 This issue is not specific to AYAC, with studies showing inadequate knowledge of fertility-related issues in adult cancer patients. 16
Insufficient information can lead to anxiety and lack of knowledge about potential health threats. 7 For example, some women delay pregnancy because of concerns about triggering a cancer recurrence, despite lack of evidence for this. 17 Some AYA who face potential infertility blame themselves and attribute infertility to something they did or feel they deserve. Well-informed cancer patients experience less depression and are better able to utilize appropriate coping behaviors.13,18,19
AYAC have expressed a desire for information to be given sensitively by professionals who are friendly, honest, clear, do not use technical jargon, and are not embarrassed.6,8,20 AYAC also want their values to be understood; some report that their physicians assumed fertility matters would be of little importance. 8
Aims
The task of professionals having oncofertility conversations with AYAC is complex and involves having to raise a sensitive topic in a manner appropriate for age and developmental stage, providing information that may be complex and outside of their specialty and supporting AYAC to make treatment-related decisions consistent with good practice and in combination with other aspects of their cancer care. There is evidence that these discussions are critical in terms of patients' short- and longer-term emotional well-being, mental health, satisfaction with care, and informed choice, but are not routinely happening to a degree AYAC consider to be sufficient. As a result, both quantitative and qualitative studies have been conducted looking at the experiences of professionals discussing fertility issues with AYAC. This systematic review aims to provide a synthesis and critical evaluation of studies investigating professionals' experiences of discussing fertility issues with AYAC patients and to understand the barriers and facilitating factors to having these conversations with this age group.
Methods
Search strategy
Relevant articles published up until July 2016 were identified by systematically searching NHS evidence (AMED, EMBASE, HMIC, MEDLINE, PsycINFO, BNI, and CINAHL databases) and Scopus using terms related to fertility, FP, cancer, professionals, and AYA. In addition, reference lists of all identified articles were screened and authors of published abstracts were contacted to obtain any available full articles not yet published. One thousand five hundred and seventy citations were identified by electronic searches, and 65 abstracts were selected for review.
Twenty-six articles were retrieved for a full-text review, of which 12 met the inclusion criteria. A manual search of reference lists and relevant journals identified a further three studies that met the criteria. In total, 15 articles reporting 14 studies were included in this review (see Fig. 1 for a flow diagram of search outcome).
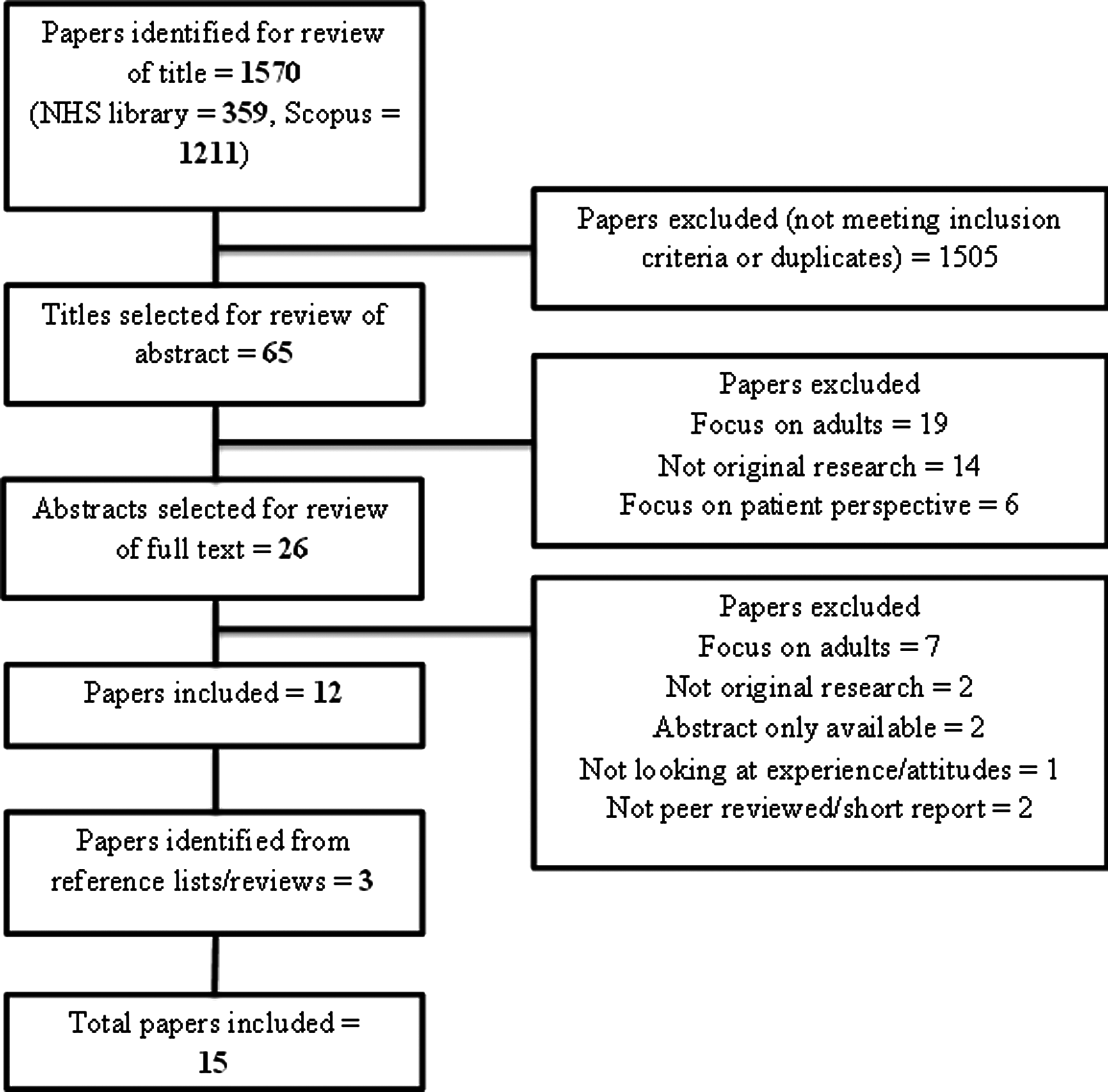
Flow diagram of search strategy. Of the 1570 articles identified by the search through NHS evidence and Scopus, 65 were selected for a review of the abstract. Thirty-nine were excluded based on the abstract, and a further 14 were excluded after reviewing the full text. In addition to the 12 articles that met criteria for inclusion, three further articles were identified from a review of reference lists and review articles, resulting in a total of 15 included articles.
Inclusion and exclusion criteria
The review included quantitative and qualitative studies published in peer-reviewed journals in the English language, in which the participants were professionals whose work included dealing with AYA cancer patients, and if there was a focus on discussions about fertility. AYA was broadly defined as 11–25 years of age to capture the variability in the literature and to reflect AYAC service provisions in the United Kingdom that extends to the age of 25.21,22 Studies were included if the professionals worked with both AYA and child populations, and results pertinent to AYA populations were extracted. Review articles and studies where the participants were professionals working solely with adult or preadolescent populations were excluded.
Quality appraisal and data extraction
PRISMA guidelines were used as a methodological structure for this review. 23 Qualitative studies were critically evaluated using the framework of Walsh and Downe. 24 Quantitative studies were critically evaluated using the criteria of Boynton and Greenhalgh. 25
Results
See Table 1 for a summary of the included studies. Two articles reported data from the same study.36,40
Summary of Included Studies
AYA, adolescent and young adult; FP, fertility preservation.
Rates and timing of fertility discussions
Six studies asked how often participants discussed FP with their patients; four reported that 63%–97% of participants routinely discussed fertility.26,31,32,35 Two studies highlighted differences in opinion versus practice; for example, in Köhler et al.'s study, 92% and 46% of participants agreed that male and female patients, respectively, should be offered FP before cancer treatment, but only 85% and 13%, respectively, reported offering FP options to these patients more than half the time.33,39
Two studies asked more specifically about the importance of initiating discussions about fertility soon after diagnosis, and factors that would influence males being offered sperm banking before undergoing chemotherapy.37,38 Another asked participants about the best time to raise fertility-related side effects, with 58.6% of participants agreeing that this was during consent to treatment. 32 Other studies did not specify when, in the patient's journey, participants currently undertook these discussions or felt they should occur.
Factors influencing fertility discussions
Patient factors
Severity of disease and prognosis
Some professionals felt it was inappropriate to invite AYAC to use FP options if they had a poor prognosis, with one study reporting concerns about the effect on young males if they were unable to produce a “good enough” sperm sample.27,29 Further, 37%–40.7% of nurses in three studies reported that the need to start treatment immediately would make discussions less likely.28,37,39 Conversely, pediatric oncologists in one American study reported that the priority of FP for them was dependent on the disease stage, but the inability to delay FP treatment would not deter them from discussing the options. 40
Another study found that not seeing the patient as having significant fertility risk was the most common reason for not discussing fertility risk or FP options. 26 Participants in three studies (38%–77.8%) reported that they would be less likely to mention FP if their patient was HIV-positive.28,37,39
Treatment
One study reported that all surveyed institutions felt sperm banking should be offered to males who would be receiving pelvic radiotherapy or bone marrow transplants; and for those receiving an alkylating agent, 80% of institutions said they would offer sperm banking regardless of dose. 27
Ethnicity
Some professionals felt that fertility concerns varied according to ethnic group.29,32 Differences between the patients' and professionals' cultural and religious backgrounds were raised as a potential barrier. 36
Age and pubertal status
Some professionals saw FP as a priority for older AYAC, and some thought that adolescents were too young to undergo FP.27,32,40 However, when asked about the youngest age that professionals would consider offering sperm banking, participants in one study reported a mean of 12.6. 33 In one study, pubertal status was predictive of fertility discussions for females (p < 0.001), with patients' age not being reported as a barrier to fertility discussions for post-pubertal patients, and another study found no large effect of age on the likelihood of FP conversations.26,39
Expressed interest
In three studies, 74%–85.2% of nurses stated that they would be more likely to discuss fertility if the patient raised the issue themselves or stated that they wanted to have children, though another found that patients instigated fertility conversations in just 2% of cases.26,28,37,39 AYAC ranked issues of fertility and sexual well-being higher than professionals. 38
Gender
Participants were more likely to discuss fertility with, and offer FP to, males.26,33,40 Patients' perceived interest was also related to gender; in one study professionals reported that females were more likely to be distraught by the possibility of infertility, and most were interested in discussing the issue of fertility. Conversely, around half their male patients were open to conversations around fertility, but half never thought about having children or were embarrassed by the topic. 40 Participants in this study were also unanimous in the opinion that females could not delay their cancer treatment by 6–8 weeks to undergo FP, whereas half felt that males could delay by 1–2 days to bank sperm. Perceived differences in families' views were also reported; 22.4% of participants in Goodwin et al.'s study agreed that the families of female patients were more concerned about fertility. 32
Socioeconomic status
Professionals perceived that the costs associated with FP was a barrier to conversations with families in one study. 36 However, in two other studies the majority of participants reported that patients not having health insurance did not affect the likelihood of discussions about FP.37,39
Relationship status and sexuality
Of the nurses interviewed in three studies, 37%–60% would be more likely to mention FP if the patient was engaged or recently married, and 22%–39% stated they would be more likely to discuss FP with a patient if that patient already had at least one child; 17%–33% also said they would be less likely to discuss FP if a participant was openly homosexual.28,37,39
Parent factors
Parents not wanting FP to be discussed with their child and/or not providing consent was described as a barrier to conversations in two studies.37,33 However, three studies reported that the majority of participants disagreed that parental consent was necessary to discuss with under-18s about FP (68%–85.2%),28,37,39 and 14/15 participants in one study said they would discuss FP with adolescents even if parents refused to give permission. 30
Two studies reported parental shock to cancer diagnosis as a barrier, which prevented the parents from focusing on anything other than survival and from seeking information about FP.36,40 In another study 58% of nurses agreed that family members might be upset with the discussion of FP. 39
Four studies noted challenges unique to serving a AYA population, notably the issue of the extent to which both patient and parent should participate.30,40 Communicating with AYA was felt as a challenge by some, with varying levels of confidence and some professionals finding the conversations “awkward”; some also reported that it was harder to communicate with parents present.36,38
Professional factors
Discomfort
Six studies reported some degree of embarrassment and/or discomfort when discussing infertility and FP, due to the emotional and intimate nature of the subject matter.29,31,34,37,38,40 In one study, some could remember a time earlier in their career when they were embarrassed. 29 Only one study reported that discomfort was not a barrier. 33
Knowledge
Lack of knowledge and false beliefs about the risks of infertility and the FP options available can be barriers to discussing fertility and FP.31–33,35,37 For example, in one study 18.9% believed that chemotherapy would increase the risk of birth defects in offspring, which is not backed by evidence, and few reported moderate or high confidence in their knowledge of FP options. 35 Further, only 53.3% of participants in one study were aware that children of childhood cancer survivors do not show a higher rate of cancer or birth defects, and 52% of nurses in another study falsely believed that children conceived from semen collected during the first week of chemotherapy or radiation therapy had an increased risk of birth defects.32,37
Professional role
Two studies looked at differences between professional groups; one found that oncologists, occupational therapists, and physiotherapists reported lower confidence in communicating with AYA than psychosocial clinicians, nurses, and AYA cancer service professionals. 38 However, another study found that significantly more physicians than nurses reported discussing with their patients the impact of cancer treatment on fertility (93.6% vs. 48.2%; p < 0.05), feeling comfortable discussing FP with adolescent males (78.7% vs. 51.9%; p < 0.05), and using educational materials with their patients (51% vs. 38.9%; p < 0.05). Further, significantly fewer nurses (18.6%) were familiar with the process of intra-cytoplasmic sperm injection, compared with physicians (51.3%) and advanced practice nurses (47.4%; p < 0.05). More physicians and advanced practice nurses were also familiar with current fertility research and recommendations for fertility practice than nurses, although statistical significance was not reported. 31
Responsibility
Five studies discussed participants' understanding of their role and responsibility in having discussions about fertility. Some nurses reported confusion about their role in FP discussions, including thinking that the doctor was doing it. 34 Pediatric oncologists in one study did not believe it was part of their role. 40 However, in both Dutch studies, participants reported that they felt it was their duty and responsibility to discuss infertility and offer FP options.30,35
Institutional factors
Time pressures
The reported impact of time pressure as a barrier varied between 37.1% and 89.2%.35,37 Having little prior knowledge of the patient and little time to form a relationship made it difficult to know how to approach individual situations. 29
Training/guidelines
The lack of training and guidelines specific to fertility issues and the AYA age group was a commonly reported barrier, with participants in five studies reporting that they would welcome training and feel that more education was needed.27,29,32,34,36 Clayton et al. found that 96% of nurses were unaware of recently published guidelines. 28 Some reported that more information would enable them to provide better explanations of fertility risks and options to their patients. 40 Another study also highlighted participants' uncertainty with the consent process, particularly for those who infrequently worked in this area. 29
Evidence base
Lack of evidence on the effectiveness of FP techniques was a reported barrier, significantly more so for females.26,32,35
Financial cost
Only 18.5%, 12%, and 9% of participants in three survey studies agreed that FP options were affordable for most patients.28,37,39 However, 96.6% of participants in one of the studies believed the cost of FP to be greater than in reality. 37
Availability of facilities
Some participants reported that it was difficult to find appropriate and/or convenient facilities and services for FP, and those who reported discomfort about FP discussions in one study felt establishing FP facilities in their area would help.26,27,32,37,39,40
Educational materials
The most commonly reported barrier was a lack of sufficient educational material about fertility and FP to offer to patients and families, as well as resources to aid discussions that are developmentally appropriate for AYA. 27,28,31,34,36,40 A number of nurses across three studies (32%–66.7%) said they would be more likely to discuss FP if they have educational materials available.27,37,39 In one study, 66% of pediatric oncologists said there is a lack of educational material in their service, or that the current material is not appropriate for their patients, and those who reported not being comfortable discussing FP said having better educational materials would help. 40
Quality appraisal of the literature
Measures
No validated measures were used in any of the studies. Eight developed measures based on the domains identified in previous literature or existing questionnaires.27–29,31,35,37,39 Six studies reported having their measures reviewed by professionals from the target population and/or “experts” in the field.27,31,32,34,37,39 This may have led to measures including only components that were deemed pertinent by the researchers and not capturing other aspects of the participants' experiences.
Generalizability
Most studies did not provide information about the demographics of their population (such as age and gender), limiting conclusions about the representativeness of the sample.26,29,32,34,36,38,40 Although Fuchs et al. reported that their survey included 13 items about participant demographics, only their profession was reported. 31 Most studies also had small participant numbers due to low response rates or the small number of available participants where sampling took place. Further, all studies required volunteer participation, and the results may not be generalizable to all staff working with AYAC, for example, those with low levels of confidence or interest in fertility.
Design
Seven survey studies provided statements for participants to agree/disagree with, or asked participants whether certain factors would make discussions around fertility and FP more/less likely.28,31,33,35,37,39 These studies did not allow opportunities for participants to report other barriers or expand on their responses. Providing suggestions may also have led to participants endorsing factors they would not have otherwise considered. However, surveys can be useful to look at trends over time, as in Clayton et al., which may be of particular value as it followed new guidelines or legislation. 28
Analysis
Five quantitative studies reported descriptive statistics only.32,33,35,37,39 Five qualitative studies reported using a range of analytic methods: grounded theory, constant comparison, intuitive analysis, and content analysis.30,34,36,38,40 Four of these studies did not provide any justification for why these methods were used, and one study that did noted that their method of intuitive analysis was used successfully by the same research team in other research. 40 Two qualitative studies did not make their analytic approach explicit.27,29
Confounding factors
Some studies reported the participants' age, gender, and time in their profession, but did not control for these variables in the analyses.30,33,35,37
No study looked separately at those who (regularly) discussed FP with patients and those who did not in order to see whether their reported barriers differed. It was not always clear whether studies reported factors as being a barrier to either having a conversation or to the FP process itself, or to what extent these barriers were real or perceived. Most studies also did not report on the consequences of these barriers or experiences, such as whether they prevented conversations from happening or impacted the length of discussions.
Discussion
The results of this systematic review highlighted that fertility is an issue that is considered important by professionals but is discussed to varying degrees with AYAC. Some patient-factor barriers reported by the professionals in these studies concur with research into patients' experiences of receiving fertility-related information, for example, age and gender affecting the likelihood of fertility discussions.26,27,32,33,38,40 Further, the level of importance attached to fertility issues is not always in line with the patient's priorities, and professionals sometimes find it challenging to communicate effectively with this patient group.36,38,41–43
Some barriers were commonly reported across studies, notably the lack of appropriate patient educational materials and staff training.27–29,31,32,34,36–40 All studies that addressed finding convenient facilities and services for FP reported difficulties doing so, and all studies looking at gender differences found that professionals are more likely to discuss and offer FP to males.26,27,32,33,37,39,40 However, several factors were reported as barrier for some but not others, such as socioeconomic status and age.27,32,33,36,37,39,40 There was some suggestion of culture and profession playing a role, although only two studies looked at differences between professional groups explicitly, and these findings were conflicting in terms of which professionals feel more comfortable communicating about fertility with AYA.30,38 This finding indicates a need for further investigation.
It was not clear to what extent these barriers may be due to professionals' own value judgments or lack of knowledge; for example, some professionals reported false beliefs about the financial cost of FP and the risk of birth defects in children resulting from gametes collected during treatment, which will likely interact with patient-factors such as socioeconomic status and disease severity.32,35,37 Lack of knowledge, lack of facilities/options, as well as the patient's actual or perceived inability to cover the costs of FP may also compound the feelings of discomfort. Further, the results show that some professionals view females as being more concerned about fertility issues, but are less likely to discuss FP options with female patients or refer them to FP services.26,32,33,40 This may be due to a lack of availability of, and evidence for, FP options for female patients, and professionals therefore feel being less able to provide a solution and less comfortable with raising the issue in the first place. However, these findings largely come from studies reporting only descriptive statistics with no exploration of impact or participants' interpretations, and thus these suggestions remain speculative.
Clinical implications
These results highlight the importance of developing relevant training for staff, building and maintaining a knowledge base and confidence around fertility issues, having clear national and service-specific policies that are effectively implemented, establishing links with specialist FP services, as well as suggest a need for longer consultations or the use of an effective screening tool to facilitate the prioritization of issues that are most salient to the patient.
The results also highlight the role of professionals' own views on a range of sociocultural issues. This has implications for general training and supervision that professionals receive around recognizing and managing their personal opinions and discomfort, particularly early in their careers. 29
Some studies reporting on barriers also reported relatively high rates of fertility discussions, suggesting that physicians try to find ways to overcome these barriers.32,35 However, no study reported that all professionals discussed fertility with all patients, indicating inequality in service provision.
Future directions and further research
Most studies focused on oncologists and nurses who have prevalent and frequent involvement with AYAC treatment. However, given that AYAC come into contact with multiple professionals, a broader awareness of fertility issues in this population and professionals' ability to support or signpost may warrant further investigation.
Further research could also develop and evaluate the effectiveness of interventions aimed at changing professionals' behavior and attitudes toward fertility discussions with AYAC, and explore whether such interventions would benefit from being tailored to different professional groups or settings. Larger-scale quantitative surveys could provide the opportunity for more sophisticated analysis, considering the effect of demographics such as gender, age, and years of experience in a professional role (the consideration of which was notably lacking from a majority of studies in this review, even in terms of reporting demographics), to inform how training and support needs may differ.
While the current research base shows factors that act as barriers to fertility conversations, why these factors prevent the conversations from happening, the extent to which they do so, and the complex interaction between factors are unclear and require further qualitative exploration. Further, since there is some suggestion that professionals try to find ways to overcome barriers to fertility discussions, investigations into what these might be will be useful to inform training and support. There is a particular lack of in-depth qualitative analysis of participants' accounts of their experiences.
Although the evidence base is still in its infancy for many FP techniques, the number and availability of these techniques is growing. Conducting further studies as more such techniques become widely available, as the evidence base grows, and following the introduction of new guidelines or legislation would help to better understand how these wider contextual events shape professionals' experiences of discussing fertility with patients and highlight when existing study results might no longer be applicable to certain settings.
Limitations of this review
The review only included articles published in English and do not represent a global experience. Further, the definitions of inclusion terms such as adolescent, teenage, young adult, and pediatric in these studies were diverse, or even not provided; due to a dearth of research in this area, it was decided to also include studies that did not provide an explanation of their included age range, but it is acknowledged that this may have resulted in the inclusion of participants who fell outside of the 11–25-year range decided upon for this review. The critical appraisal highlighted the limitations of available research, and results should therefore be interpreted with caution.
Conclusions
A variety of factors influence the likelihood of fertility conversations, and providing staff with appropriate training and educational materials may help to address the role played by professionals' value judgments and lack of knowledge.
More high-quality research is needed in this area; there is also a need to explore how, and to what extent, reported barriers impact clinical practice in order to gain a greater understanding of facilitating factors. This, as well as examining the differences across professional groups and services, is vital to better inform the development of education and training that so many professionals would welcome. Further, there may be a need to address the practicalities related to how services are set up both locally and nationally to ensure the application of policies and guidelines and to offer professionals the tools required to provide an equitable service to their patients.
Footnotes
Acknowledgment
Thanks to Dr. Myra Cooper, Dr. Susie Hales, and Dr. Aiysha Malik for their support in developing this review and for providing feedback on the process.
Author Disclosure Statement
No competing financial interests exist.