
Abstract
Purpose:
Fertility preservation (FP) is a critical component of adolescent and young adult (AYA) cancer care that remains inadequately delivered. Prohibitive cost due to a lack of insurance coverage remains a barrier. Since 2004 Sharing Hope/LIVESTRONG Fertility has assisted AYA cancer patients through discounted FP rates and access to free medications.
Methods:
Demographics, cancer diagnoses, and dollars saved by patients who used the Sharing Hope/LIVESTRONG Fertility program from 2004 to 2011 were retrospectively reviewed and reported using descriptive statistics. Utilization of financial services for the most common diagnoses was compared with the rate of diagnosis among AYAs.
Results:
One thousand one hundred fifty men and 1301 women received assistance between 2004 and 2011. Median age was 24 years (range, 12–67) for men and 30 years (range, 13–49) for women. Breast cancer, Hodgkin lymphoma (HL), and genitourinary cancers were the most common diagnoses among females; testicular cancer and HL were most common among males. Recipients represented 1245 cancer centers across the United States. Average cost savings was $6587 per female and $386 per male. Program utilization/diagnosis ranged from 0.8% to 2.7%.
Conclusion:
Utilization of financial assistance for FP was low despite literature pointing to the need for such assistance. Costs for FP for women far exceed those for men. State-specific insurance initiatives are beginning to mandate coverage for FP. As insurance coverage expands, further studies are needed to determine the true financial burden to patients, the degree to which lack of resources prevent FP in this population, and the impact that insurance coverage has on the provision of these services.
Introduction
In the United States, over 70,000 adolescent and young adult (AYA) males and females are diagnosed with cancer annually. 1 With the use of multimodal therapy, the vast majority of these individuals can expect to be cured of their cancer, but may face detrimental side effects, including loss of fertility, an outcome that is of great concern to young cancer survivors.2,3
Sperm banking has long been considered the standard fertility preservation (FP) option for post-pubertal males. 4 Live births have been reported from sperm thawed following cryopreservation for periods >20 years. 5 When patients cannot masturbate to ejaculation, procedures such as electro-ejaculation or testicular aspiration can be utilized to collect sperm that can then be frozen. 6 Due to intracytoplasmic sperm injection, even small numbers of cryopreserved sperm can lead to live births. Sperm cryopreservation typically costs about $700–900 for the initial collection and approximately $200–400 per year for subsequent storage. 7
The current standard-of-care options for the preservation of fertility in post-pubertal women include freezing oocytes and embryos, although oocyte freezing carried an experimental label until 2012.8,9 These procedures pose greater logistic problems than sperm banking. In both instances, women must have their ovaries hyper-stimulated with reproductive hormones so that multiple oocytes mature simultaneously. Once the oocytes have matured sufficiently, they are retrieved transvaginally under sedation. In the breast cancer population, it has been demonstrated that the use of random-start ovarian stimulation (i.e., not timed with the start of a menstrual cycle) did not delay the start of chemotherapy compared with individuals who did not undergo ovarian stimulation. 10 In terms of delaying the start of therapy, there is no difference between oocyte and embryo freezing as the fertilization of oocytes to embryos is done in vitro, and therapy may begin as soon as oocytes are retrieved.
Embryo/oocyte cryopreservation may cost up to $3000–5000 for the necessary ovarian stimulation drugs, and between $5000 and $10,000 for the procedures leading to cryopreservation, including but not limited to office visits, monitoring labs and ultrasounds, egg harvesting, in vitro fertilization when embryo cryopreservation is desired, and cryopreservation of oocytes and/or embryos. 7
Acknowledging the risks to fertility and the options that exist to preserve fertility, the American Society of Clinical Oncology, the American Society for Reproductive Medicine, and the National Comprehensive Care Network have all issued guidelines that recommend medical team address the possibility of infertility as a risk of cancer treatment as early as possible with newly diagnosed patients and make referrals to reproductive specialists or offer sperm banking as indicated before initiating appropriate treatment.11–13 Despite the consistency across these guidelines, identifying FP as a critical component of comprehensive AYA cancer care, it continues to be discussed and/or offered to only a fraction of eligible patients.14–17
Multiple barriers have been identified that prevent the full implementation of FP services to eligible patients. Barriers that exist for patients include being overwhelmed with information at diagnosis, difficulty obtaining information about fertility risks and FP options, and lack of coordination of services. Barriers at the provider level include lack of knowledge about fertility risks and FP options, assumptions related to patients' interest in FP based on age, parity status, and prognosis. A reluctance to delay the start of therapy has been identified as a barrier by both patients and practitioners. And, on the institutional level, a lack of adequate reproductive facilities, poor coordination among oncologists and reproductive specialists, and lack of guidelines for the provision of FP services have been identified as barriers as well.18,19
An additional significant barrier to the provision of FP services is cost, as most insurance companies do not cover FP procedures, and until recently there have been no mandates to do so. 20 In 2004, acknowledging the significant role that finances played in access to FP, the not-for-profit organization, Fertile Hope, created “Sharing Hope,” the first financial assistance program for FP to cancer patients. The program was created to provide financial assistance to cover oocyte, embryo, and sperm cryopreservation. Ovarian and testicular tissue cryopreservation were not included in the procedures available for assistance. Eligibility for the program required that patients had a cancer diagnosis, were U.S. citizens, and met financial need criteria, as well as a statement from the treating oncologist that proposed cancer treatments pose a threat to future fertility and that fertility treatments and associated medications are not contraindicated for a given patient. The program was structured so that no direct payments to the patient were needed. Instead, providers (reproductive endocrinologists and sperm banks) were contracted to substantially discount their rates for oocyte, embryo, and sperm cryopreservation. Medications required for ovarian stimulation were donated by a partnering pharmaceutical company. In mid-2009, Fertile Hope and the Sharing Hope program were acquired by the LIVESTRONG Foundation, and the Sharing Hope program became known as “LIVESTRONG Fertility.”
The aims of the current study were to quantify the utilization of the Sharing Hope/LIVESTRONG Fertility program by describing the demographic characteristics, geographic distribution, and the cost savings of the program on patient applicants from 2004 to 2011.
Methods
Deidentified records maintained by LIVESTRONG, which included the data collected during the time the program was administered by Fertile Hope, as well as when LIVESTRONG was administering the program, were retrospectively reviewed. The total number of patients receiving discounted FP rates and/or free medications from this program were available from 2004 to 2018. More detailed patient characteristics, including gender, age, cancer diagnosis, and the patient's home state, were available from 2004, when the program was initiated, through 2011. After 2011, these additional detailed data were not available for similar analyses. From 2004 to 2010, the utilization of oocyte versus embryo freezing as the method of FP was also available for female patients. Partner status was not available. Cost savings per patient were calculated by subtracting the discounted rate offered by the clinic or sperm bank to LIVESTRONG Fertility clients from the standard rate for FP procedures offered publicly. For men, cost savings included sperm banking and any additional relevant charges, such as the analysis of semen specimen. Some sperm banks included 1 year of storage at no cost to the patient, through a partnership with a long-term storage facility. For female patients, the market cost of FP medications was also added to cost savings as these medications were donated. Numbers regarding geographic location of patients were also reviewed and summarized. Summary statistics were utilized to describe these data.
To estimate the percentage of patients who utilized LIVESTRONG Fertility, we accessed incidence rates of the most common diagnoses in this cohort, at the website of the Centers for Disease Control and Prevention, U.S. Cancer Statistics for the year 2011, and compared this to the number of patients who used the financial assistance program in that year. 21 Percentages were calculated for the most common diagnoses in the study cohort among those 15–39 years old.
The study was reviewed and approved by the Columbia University Medical Center Institutional Review Board.
Results
From 2004 through 2018, LIVESTRONG Fertility has served over 11,481 individuals, 4272 males and 7209 females (Fig. 1), through over 670 network clinics, saving patients over $50,000,000 in FP services. 22 Between 2004 and 2011 when specific patient data were available, a total of 2451 individuals received financial assistance. Recipients resided in 49 states of the United States, as well as Washington DC and Puerto Rico. Although applications were received across almost all U.S. states, utilization rates were highest in California (23.1%) and New York (14.9%); utilization from these states was similar between men and women.

Utilization rates of financial assistance program from 2004 to 2018 by gender.
Eleven hundred and fifty men received financial assistance between 2004 and 2011. Annual utilization of LIVESTRONG Fertility grew from 8 men to 285 men over this time period. Their median age was 24 years (range, 12–67). The two most common diagnoses were testicular cancer (34%) and Hodgkin lymphoma (HL, 18%). The full distribution of diagnoses is presented in Figure 2. A total of $444,361 was saved by having sperm banks provide discounted rates, averaging $386 per male patient.
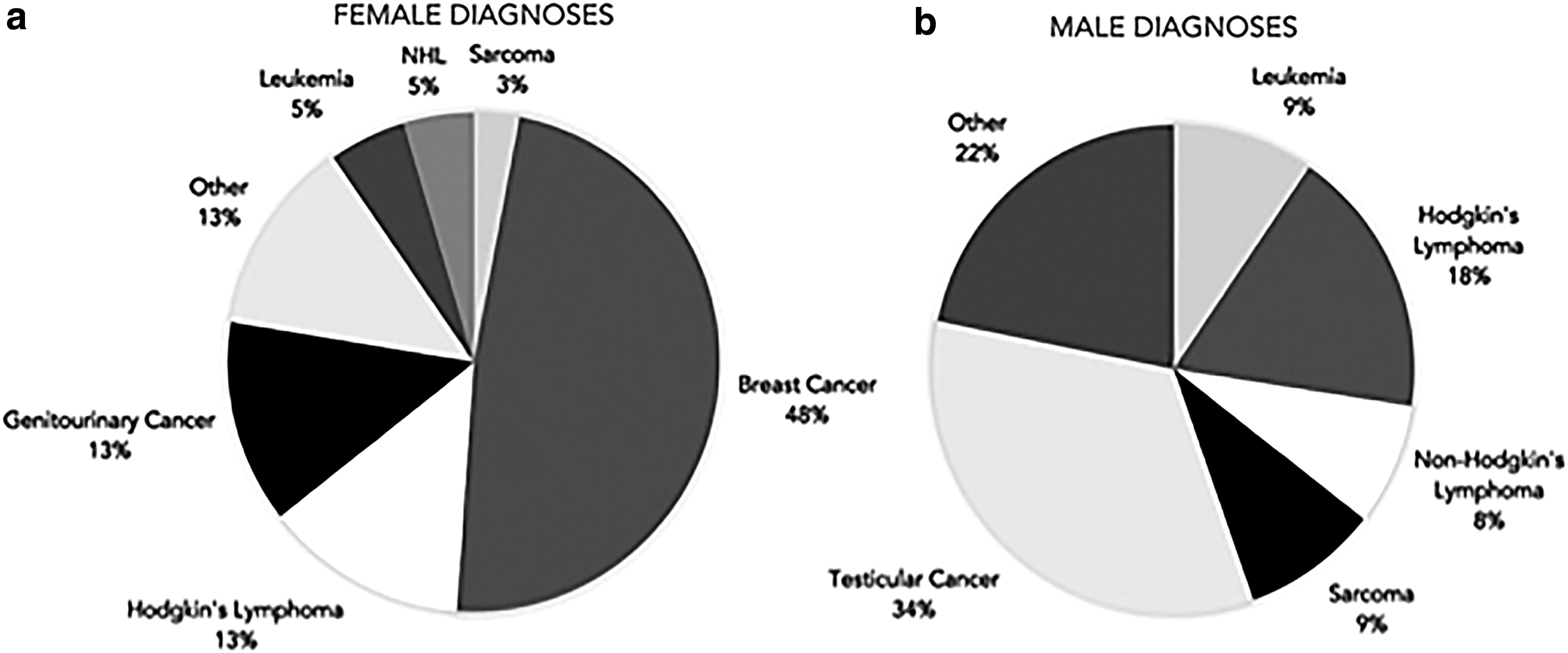
Breakdown of
Thirteen hundred and one women received financial assistance in the form of discounted rates by reproductive endocrinologists and provision of donated medications between 2004 and 2011. Their median age was 30 years (range, 13–49). The most common diagnoses included breast cancer (48%), HL (13%), and genitourinary cancers (13%) (Fig. 2). Similar geographic trends were noted for women as were seen in men. For women, a total of $3,904,303 was saved in discounted rates and $4,665,775 in medication costs, averaging $6587 per female patient. Fifty-one percent of women who received financial assistance between the years 2004 and 2010 opted for embryo cryopreservation, 40.6% pursued oocyte cryopreservation, and 8.3% utilized a combination of both methods. Women with breast cancer were more likely, than those with other cancer diagnoses, to opt for cryopreservation of embryos (Table 1). The mean age of patients who froze oocytes was 28 years, embryos only 32 years, and 31 years for patients who froze both.
Female Fertility Preservation Method by Cancer Diagnosis, 2004–2010
Within the 15- to 39-year age group, the rate of financial assistance utilization in 2011 (the year with the highest utilization of the program) was 2.7% among women with HL, 1.5% for those with breast cancer, 2.0% for testicular cancer, and 0.8% for female genitourinary cancers (Table 2).
Use of Financial Services Compared with Total Annual Diagnoses by Disease
Discussion
Preserving the capacity to have biologic children after the completion of cancer-directed therapy is a critical component of comprehensive cancer care in reproductive-age cancer patients. Yet, multiple barriers continue to exist that prevent the full inclusion of FP in this population, including the high cost of the procedures.20,23,24 Our review of LIVESTRONG Fertility demonstrates that the utilization of financial assistance to cover the high costs of FP has grown over time and that the need for this coverage exists across the entire country. The higher rate of usage of the program in California and New York may represent the large number of reproductive specialists and sperm banks that exist in these two states. The etiology of the median age difference between men and women is not clear and deserves further exploration. Our data suggest that embryo cryopreservation was a slightly more common method of preserving fertility compared with oocyte cryopreservation, particularly among women with breast cancer. This may, in part, be explained by the fact that oocyte cryopreservation was still considered experimental in the years 2004–2010, having achieved non-experimental status in 2012. 8 It could also be hypothesized that breast cancer patients represent a slightly older patient population compared with diagnoses of leukemia and lymphoma and may have been more likely to be in a committed relationship and, therefore, opt for embryo cryopreservation. Not surprisingly, the cost savings for women were almost 20-fold higher for newly diagnosed patients compared with males.
Despite being one of the oldest and most established financial assistance programs operating in the United States, LIVESTRONG Fertility is only utilized by a small subset of reproductive-age patients at risk of fertility impairment. This may be, in part, related to FP procedures being cost-prohibitive despite financial assistance. As indicated above, initial costs for sperm cryopreservation range from approximately $500 to $700. With average cost savings of $386, men would still pay $314–514, excluding the costs for long-term storage. Costs for the drugs needed for ovarian hyperstimulation range from $3000 to $5000 for a stimulation cycle. Within this range, patients in this cohort saved an average of $3587 by having drugs donated to them. Costs for the procedures associated with oocyte/embryo cryopreservation range from $5000 to $10,000. Discounts from practitioners for these procedures averaged $3000 per patient. Therefore, female patients would still be responsible for $2000–7000 to undergo these procedures.
Studies have identified that the perceptions of oncologists about patients' ability to pay for FP deters them from providing information.25,26 Qualitative investigations have found that physicians believe finances pose a barrier for most patients based on their experience with trying to identify insurance coverage for sperm banking or oocyte preservation. 27 A study of FP counseling in the state of Georgia identified that women who did not have insurance or were publicly insured were less likely to receive counseling from medical professionals. The authors speculated that concern about the financial burden of cancer treatment and the perception that FP options are cost-prohibitive may be contributing to the lack of counseling. 16 A recent systematic review noted cost and financial concerns were among the top five factors hindering the decision to pursue FP by women with cancer; financial concerns were related to self-funding treatment and not feeling financially secure. 28 Perceiving cost as strongly influential in the decision to pursue or not pursue FP has also been found to be associated with higher decisional conflict among patients. 29
Having insurance coverage does seem to impact the utilization of FP. A retrospective review compared patients presenting for medically indicated FP, who had some form of fertility benefits, with those who did not. Insurance information was available on 269/332 individuals (81%). Within this group, 99.3% had insurance, 34.9% had insurance benefits for FP, 25.9% of which included oocyte vitrification. A higher percentage of patients who proceeded to stimulation had both fertility benefits (42.1% compared with 27.1%, p = 0.01) and oocyte vitrification compared with patients who did not undergo stimulation (31.4% compared with 19.8%, p = 0.04). 30 When the experiences of women pursuing medical egg freezing in the United States were compared with those of women in Israel, where it is covered by national health insurance, the women in the United States had greater difficulty funding their FP, and this added significant emotional and financial pressure to already stressful circumstances. 31
Currently, only 15 states in the Unites States provide insurance coverage for any female infertility factor, and only eight provide such coverage for male infertility factor, and often this coverage does not extend to medically induced needs for FP, such as potential gonadotoxicity, from cancer treatment.20,32 In part, this insurance does not extend to this population because they are not considered infertile at the time they are seeking coverage. One argument for coverage is that the current definition of infertility can neither account for, nor accommodate the needs of, cancer patients who may be rendered infertile by their cancer treatment. Thus, one method of ensuring that children or people in their reproductive years who are diagnosed with cancer have access to, and insurance coverage for, FP is to legally treat them as a distinct group from individuals in the general population who have been diagnosed with infertility. 33 Such an argument has been applied successfully to other iatrogenic conditions such as the need for reconstructive surgery following mastectomy for breast cancer, or wigs for alopecia.23,34,35
In 2017 Connecticut and Rhode Island were the first states to pass legislation mandating the coverage of FP services for medical treatments that could affect fertility. 20 In 2018 Delaware, Maryland, and Illinois followed and have passed legislation specifically requiring insurers to cover FP services for patients undergoing cancer-related treatment that may cause infertility. 36 However, this coverage is available only to those who participate in state-regulated insurance policies and not to those who receive Medicaid, Medicare, or employment-based insurance coverage where insurance claims are paid for by the company itself. Other states, including California, Hawaii, Kentucky, Missouri, and New York, have introduced bills that have not yet been adopted. 37 Until universal state legislature and insurance reform are undertaken, financial assistance programs will continue to be a critical component of providing comprehensive care to individuals diagnosed with cancer during their reproductive years. In fact, since the establishment of Sharing Hope in 2004, a number of financial assistance programs to FP for cancer patients have been created, including but not limited to the Heart Beat Program, Team Maggie, Bonai Olam, Verna's Purse, Fertile Action, and The SAMFund.
To our knowledge, this is the first study detailing the demographics of patients who have used a not-for-profit financial assistance program to access FP at the time of a cancer diagnosis. Due to the programmatic goal of rapid access to financial assistance, limited amounts of data were collected between 2004 and 2011, and inconsistent methodologies were used to collect data in more contemporary years. While this limitation restricts the investigations we were able to undertake and the conclusions we were able to draw, it does allow us to highlight the role that patient-centric non-for-profit organizations can play in the delivery of comprehensive cancer care when traditional medical infrastructure – for example, medical centers and insurance companies – inadequately address aspects of this care. The study also draws attention to future opportunities for academic centers to partner with patient-centric not-for-profits to collect more consistent, comprehensive data that can then be reported in the medical literature with additional rigor. Further studies of this nature are needed to determine the true financial burden of FP and the degree to which lack of financial resources and insurance coverage prevent FP in this population. As insurance coverage for FP expands, studies should document the financial, medical, and psychosocial impact of this coverage in the AYA cancer patient/survivor population.
Footnotes
Acknowledgment
There is no research support affiliated with this article.
Author Disclosure Statement
No competing financial interests exist.