
Abstract

Introduction
Progression and achievement of education and vocational goals are considered developmentally imperative milestones and strong determinants of future health and quality of life for adolescent and young adults (AYAs) (aged 15–25 years within Australian oncology). 1 For AYAs with cancer, remaining engaged in education and vocational pursuits, known as productive occupations, can also greatly assist with adjustment to illness and recovery through optimizing a sense of normalcy and purpose, maintaining identity and promoting peer connectedness.2–5 Unfortunately their ability to remain engaged is often threatened by the array of challenges they encounter. These challenges can be referred to as “occupational performance issues” whereby ability to “choose, organize, and satisfactorily perform meaningful occupations” is impaired. 5
Despite increasing awareness of the role health care providers can play in facilitating engagement in education and vocational pursuits, this remains a significant unmet need for AYAs during and post-treatment.6,7 The impact is paramount with ∼50% of AYAs identifying ongoing difficulties with previous education or employment plans up to 24 months post diagnosis. 1 It is thus unsurprising that unemployment in U.S. populations is significantly higher for AYAs (34.1%) than for healthy controls (13.7%). 8 Given AYAs are at foundational stages of employment, this will likely have significant long-term impacts on career direction and financial stability. 9
The importance of supporting AYAs to remain engaged in productive occupations cannot be understated given disengagement is associated with pervasive short- and long-term adversities. This includes increased risk of longstanding unemployment, chronic medical conditions, mental health concerns, and social and economic disadvantage.2,4,8 It can also have considerable impacts on communities, such as increased health and welfare system expenditure, reduced social cohesion, and stunted economic productivity.2,4
This perspective article aims to highlight how the Canadian Model of Occupational Performance and Engagement (CMOP-E) may aid in comprehensively understanding the factors affecting the ability of AYAs to perform and engage in productive occupations. Relevant and current literature will be applied to the CMOP-E that will hopefully highlight its capability to guide intervention development for this population.
Canadian Model of Occupational Performance and Engagement
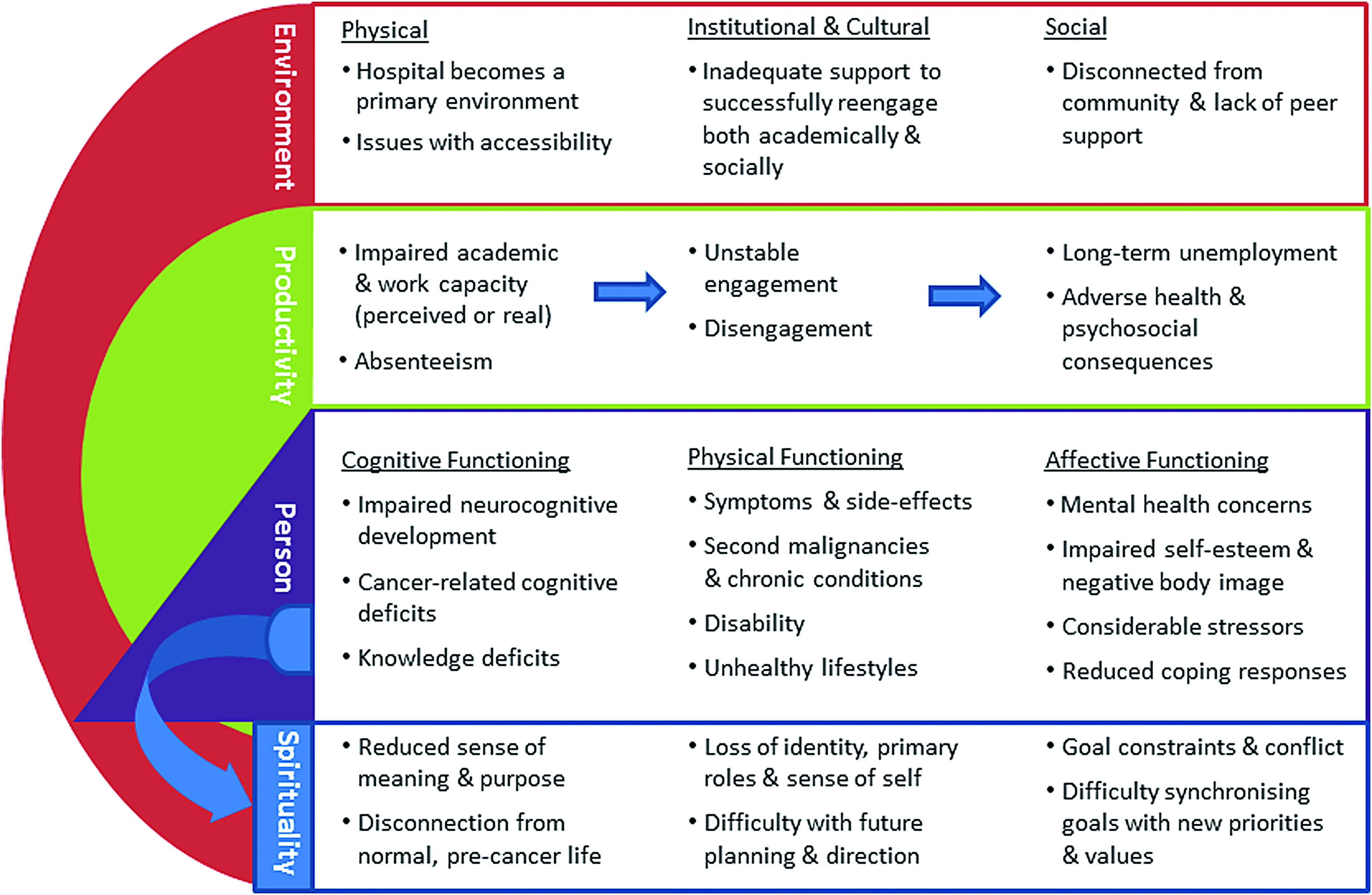
The CMOP-E determines an individual's ability to perform occupations and also their level of engagement by highlighting their strengths, resources, and limitations within three key components. 5 These components are occupations (including productive occupations), the person (encompassing physical, cognitive, and affective functioning), and environments within which occupations are performed (comprising physical, cultural, institutional, and social domains) (Fig. 1). 5 They are connected by a dynamic and interdependent relationship whereby variation in one component can affect the others and result in occupational performance issues. 5 The issues that AYAs commonly encounter with respect to productive occupations will now be examined through the CMOP-E lens (Fig. 2).
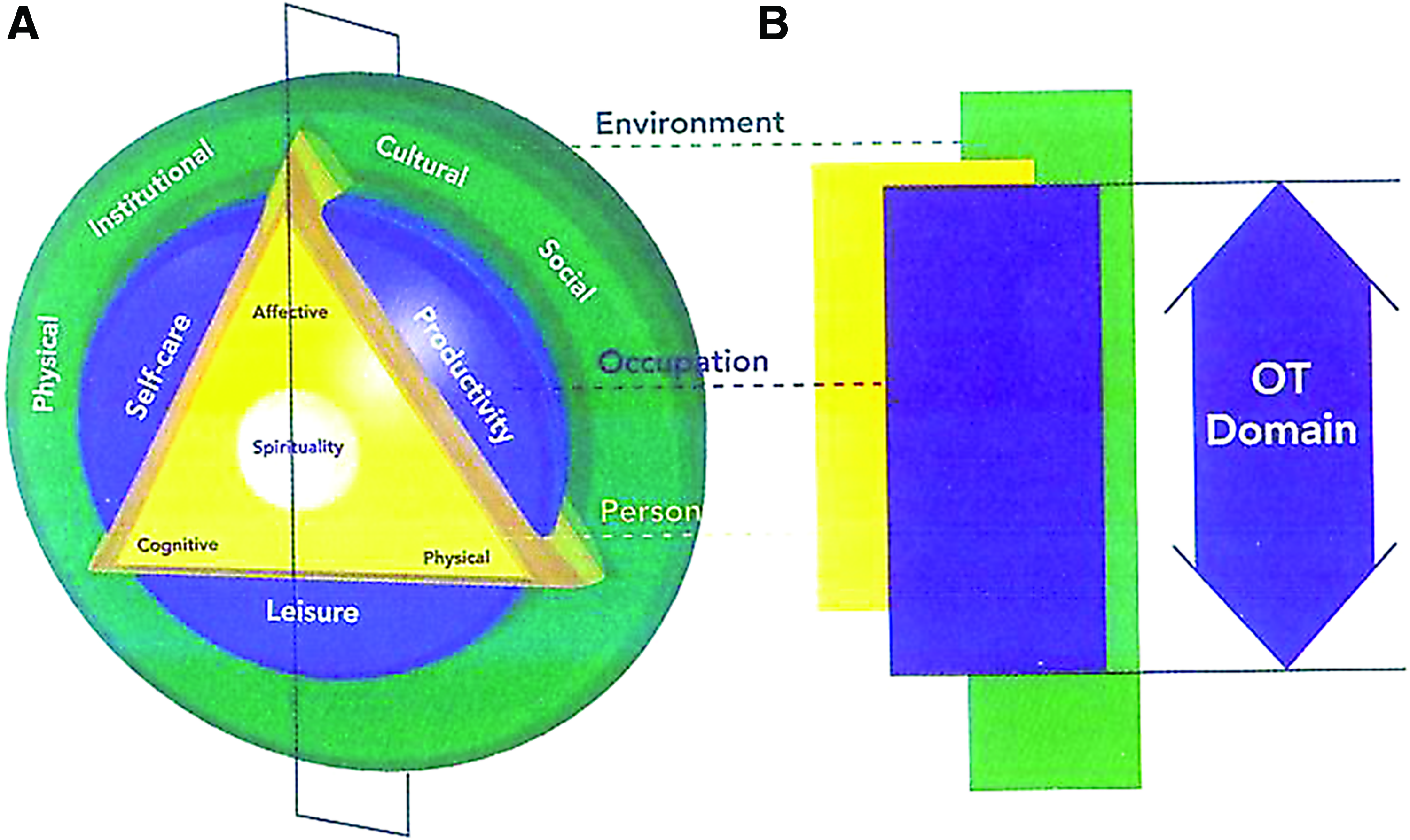
Application of the CMOP-E for the adolescent and young adult population. Color images are available online.
Disruptions to the person
Physical functioning
Cancer and its treatment are associated with a range of symptoms and side effects, which fluctuate in severity and can severely hinder academic and work capacity of AYAs. These include treatment-related toxicities such as pain, gastrointestinal issues, cachexia, neuropathy, and lymphedema.8,10 Cancer-related fatigue can also significantly affect function given it often causes a feeling of weakness, impairs cognitive functioning, and decreases motivation and mood. 11 It has been identified as a significant barrier for returning to school in a number of studies. 11
Beyond the acute phase of treatment, AYAs are at risk of second malignancies and chronic medical problems, including cardiovascular disease, hypertension, asthma, diabetes, and obesity.8,10,12 Furthermore, they report greater prevalence of disability (compared with AYAs with no cancer history), which may include impaired upper or lower limb function, further impairing occupational engagement.8,12 Functional status can also be impaired by increased likelihood of unhealthy lifestyle behaviors, including low physical activity, poor diet, and substance abuse (Fig. 2).8,12
Cognitive functioning
AYAs commonly experience neurocognitive challenges given development of the prefrontal cortex, and formal operational thought is not completed until late 20s.13,14 These challenges can include difficulties with deductive and analytical reasoning, logical and abstract thought processes, and problem-solving and moral behavior.3,13 Furthermore, behaviors tend to be reactive and emotional rather than reflective and rationale given the amygdala, emotional center of the brain, matures before the frontal lobe. 13 This development may compromise cancer and its treatment due to brain vulnerability, and given stressful circumstances can result in regression to well-established concrete thought processes.1,3,15
In addition to developmental neurocognitive difficulties, AYAs may also experience cancer-related cognitive dysfunction (CRCD), which can arise regardless of age, diagnosis, and treatment. It encompasses difficulties with working memory, concentration, attention, language, multi-tasking, and organizational skills. 16 CRCD can be longstanding with a significant percentage of AYAs continuing to experience difficulties with attention, memory, and “keeping up” with work or studies post treatment. 9
Many AYAs lack knowledge and skills that are essential for gaining employment or undertaking further education.1,17 This includes their rights as an employee or student with a chronic illness and entitlements (such as accommodations and modifications) that can alleviate impacts.1,17 They also frequently express uncertainty with regard to disclosing diagnosis and explaining gaps in employment history to potential employers. 17 For those wanting to undertake further education, in particular those who want to commence or resume after a period of disruption, knowledge is often lacking regarding tertiary education options, application processes, and special consideration entitlements (Fig. 2).
Affective functioning
Visible symptoms, treatment effects, and functional deficits can be particularly damaging for AYAs given their developmental stage.2,3 Feeling similar to, and accepted by peers, is of significant importance with formal operational thought and egocentrism, enabling thoughts of others to be conceptualized.2,3 Subsequently, concerns regarding body image and functional deficits may result in social avoidance, disconnection, and isolation.2,3 Social difficulties may also arise due to different perspectives and priorities compared with peers as a result of exceptional experiences.2,18 Furthermore, AYAs are at increased risk of mental health concerns, including post-traumatic stress, anxiety, and depression, given exposure to considerable stressors and evolving coping responses. 2 This can impair education and vocational capacity with post-traumatic stress and emotional symptoms associated with poorer school and work functioning (Fig. 2). 1
Disruptions to spirituality
Spirituality lies within a person's core and refers to sense of identity, connection, meaning, and purpose that can be acquired through positive occupational engagement. 5 These aspects may subsequently be disrupted for AYAs who are unable to remain engaged in productive occupations. Spirituality also encompasses goal setting with AYAs often experiencing goal constraints and conflict due to uncertainty regarding their capabilities, impaired physical or cognitive functioning, regression of independence, or fears regarding their prognosis and future.2,3 Conversely, modification of vocational goals may occur for positive reasons. For instance, AYAs may consciously decide to adjust goals to synchronize with new life values and priorities, such as health, enjoyment, altruism, and work–life balance (Fig. 2). 2
Disruptions to the environment
Education facilities or workplaces are usually key physical environments for AYAs. However, for those with cancer, they are often replaced by the hospital given treatment regimens tend to comprise frequent and lengthy inpatient admissions and outpatient appointments. In addition, accessing these environments may be challenging for AYAs with functional deficits. Institutional (policies and procedures of organizations), cultural (beliefs and values within communities), and social environments (including peer relationships) are intertwined and can have a significant impact on engagement. For instance, key barriers to resuming school include inadequate support from schools and hospitals (which may be due to institutional or cultural factors) to assist AYAs with re-engaging both academically and socially (Fig. 2).18,19
Application of CMOP-E
ONTrac at Peter Mac Victorian Adolescent and Young Adult Cancer Service provides comprehensive multidisciplinary care for patients aged 15–25 years. A service priority is supporting AYAs to remain engaged in productive occupations from time of diagnosis. Reassurance often needs to be provided to AYAs, parents, health care professionals, and education facilities or workplaces that most patients are able to remain engaged, at least to some extent, regardless of diagnosis, prognosis, or treatment regimen. Realistic goals and plans are developed with AYAs in collaboration with family, treating team and education facility or workplace. Plans need to be flexible to accommodate fluctuations in medical and functional status and encompass supports and modifications to optimize strengths, compensate for deficits, and ensure equitable access. This can include adjustments to treatment schedule, physical environment, study, or work demands and delivery mode. Multidisciplinary expertise are utilized to address occupational performance issues—for instance fatigue is often multidimensional with physical and psychosocial components that requires intervention from a range of health care professionals. Education is frequently provided regarding symptom management and strategies to optimize learning capacity and work productivity. Patients requiring prerequisite employment skill training and long-term support with maintaining and obtaining employment are referred to suitable employment services, such as disability employment services and recruitment agencies. Interventions align with research that highlights the importance of developing education and vocational programs that address physical and psychosocial needs and utilize skills of employment professionals.1,2,7,18–21
Conclusion
AYAs with cancer are at risk of productive occupational performance issues for a host of reasons. This can have serious implications and is, therefore, an area in need of considerable attention. The CMOP-E provides a comprehensive lens to identify, and thereby address, occupational performance issues. It is a valuable framework for assisting AYAs with cancer to remain engaged or re-engage in education and vocational pursuits and support them with the imperative task of becoming “… self-reliant, independent and productive members of society.” 22
Footnotes
Acknowledgments
We acknowledge the Victorian Department of Health & Human Service who funds the Victorian Adolescent and Young Adult Cancer Service and the Australian Government who funds Youth Cancer Services via CanTeen Australia.
Author Disclosure Statement
No competing financial interests exist.