
Abstract
The human papillomavirus (HPV) causes several cancers and genital warts among sexually active adolescent and young adult (AYA) males. Quadrivalent HPV vaccines were approved for use in the AYA male population in 2010, but vaccination rates have plateaued at around 10%–15%. A better understanding of the barriers AYA male patients, their parents, and their health care providers (HCPs) experience with respect to vaccination uptake is necessary for tailoring interventions for this population. A literature search was conducted through the PubMed and PsycINFO databases in October 2017. Studies were included if they specified at least one barrier to vaccination uptake in AYA males. Studies were excluded if they did not focus on AYA males, their parents, or their HCP; were conducted outside the United States; or were published before 2010. A total of 23 studies were reviewed, and analysis found that these three groups (i.e., AYA males, parents, and HCPs) had significantly different concerns regarding vaccination. The identified themes included the lack of HPV vaccine awareness/information, misinformation about HPV, lack of communication, financial issues relating to uptake, demographic/perceived social norms, and sexual activity. Health care professionals working directly with AYA males and their parents should provide an open route of communication regarding these sensitive issues, and further educate families on the importance of HPV vaccines in reducing the incidence of certain cancers among men in later adulthood.
Introduction
The human papillomavirus (HPV) is the most common sexually transmitted infection (STI) in the United States (US), accounting for 49.5% of STIs in adolescent and young adult (AYA) males 15–28 years of age. 1 More than 16,500 HPV-associated cancers are diagnosed among males each year, 2 and HPV is responsible for more than 60% of penile cancer and 90% of anal cancer cases in males in the US. 2 Males are three times more likely to be infected with HPV than females, but future cancer incidence remains higher in females overall. 2 HPV tends to present with few visible symptoms in men,2–4 making transmission and acquisition of HPV more prevalent among this population.2,5
The most popular vaccination against HPV will aid in preventing the transmission and acquisition of HPV for AYA males and their future partners, protecting them from future HPV-related health complications, including specific cancers and genital warts.2,6
The most popular vaccine for HPV, Gardasil©, was recommended by the Advisory Committee on Immunization Practices (ACIP) for males 9–21 years of age in 2010. Following the ACIP recommendation, the Centers of Disease Control and Prevention (CDC) chose to implement the following recommendation for adolescent males and the HPV vaccine: male adolescents should receive the first HPV vaccine between 11 and 12 years of age and complete the two-dose regimen before the age of 132; for adolescent males, who do not receive the first of the HPV series by 15, the CDC recommends the three-dose series. 2 For specific male populations (e.g., men who have sex with men, gay or bisexual men), the HPV vaccine is recommended up to 26 years of age. 2 For males who are not within special populations, the vaccine is permissive between 22 and 26 years of age. 2
Despite the FDA's recommendation of the vaccine and the elevated level of risk for HPV infection among AYA males, vaccination rates remain low in this population. 3 Vaccination completion rates in AYA males in 2016 ranged from 10.7% to 20.8%. 3 HCPs recognize the importance of HPV vaccination among adolescent boys, 2 but face difficulty in recommending HPV vaccination to their male patients due to the general population's lack of knowledge about HPV vaccination among this population. 6 Other barriers to HPV vaccination in this population include insurance and cost issues, concerns about vaccine safety, misconceptions about personal relevancy of the vaccine and HPV risk, and other factors such as sexual activity, age, and number of sexual partners.7–12
The aim of this literature review was to identify barriers to HPV vaccination uptake within the US from the perspective of AYA males, their parents/caregivers, and their HCPs.
Materials and Methods
Data sources and study selection
The PubMed and PsycINFO databases were searched and cross-referenced with the following search terms on October 9, 2017: HPV, human papillomavirus, adolescent, teenager, teen, young adult, males, boys, men, cancer, Gardasil, prevention, vaccine, and vaccination. With the help of a research librarian, search terms were inputted into each database and results were saved for review of study inclusion/exclusion.
Studies were eligible for inclusion if they met the following criteria: (1) examined male adolescents/young adults (AYA males were identified as being between 15 and 29 years of age), (2) reported male adolescents/young adults', their parents', and/or their providers' perceptions of barriers to the HPV vaccine and/or HPV risk, (3) were published between February 2010, when the U.S. Federal Drug Administration (FDA) approved Gardasil for AYA males, and October 2017, and (4) were conducted within the US. Studies that did not allow for examination of male-specific results, separate from female results, and studies not written in or translated into English were excluded from the review.
Data extraction and analysis
Our search yielded a total of 2672 unique articles. One reviewer (K.D.) reviewed article titles, and 1916 articles were eliminated because they did not examine males and 41 articles were published before 2010. Two reviewers (K.D. and J.M.) analyzed the remaining 715 abstracts. A total of 603 articles were eliminated because they did not describe AYA male, parent, or provider vaccination barriers, and 42 were eliminated because the studies were conducted outside the US (Fig. 1).
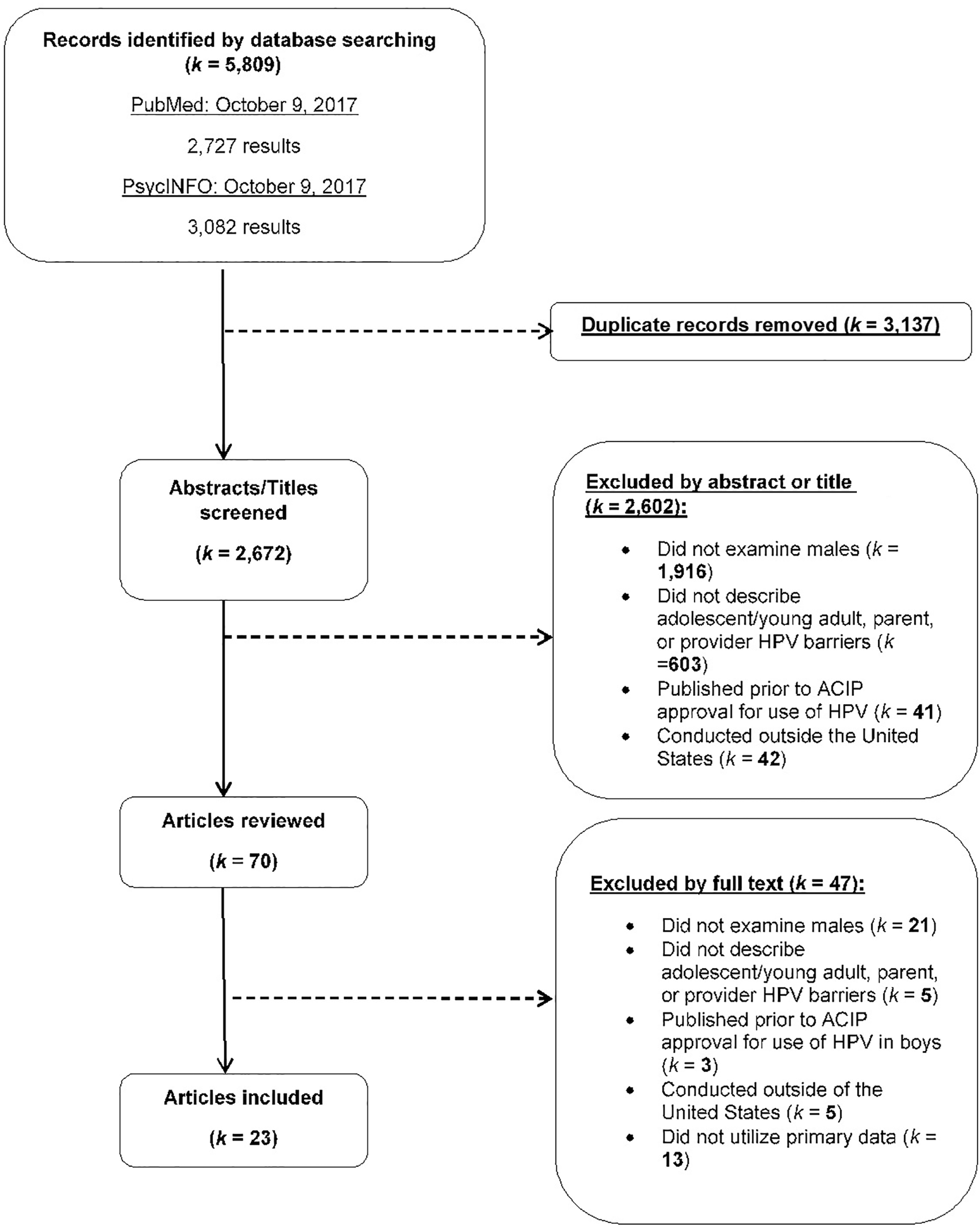
Elimination process for this review. The PRISMA diagram details our search and selection process applied during this systematic literature review.
Two reviewers (Kate Dibble and Morica Hutchison) examined the remaining 70 full-text articles, eliminating 21 articles because they did not examine males; five because they did not describe AYA male, parent/caregiver, or provider vaccination uptake barriers; three because they were published before FDA recommendation for use of the HPV vaccine in boys; five because the studies were conducted outside the US; and 13 because they examined nonoriginal research (e.g., editorials and commentaries). A total of 23 articles were included in the literature review. We calculated Cohen's kappa statistic to assess interrater reliability (e.g., agreement) between reviewers on the inclusion and exclusion of articles, finding strong agreement (Cohen's kappa = 0.87).
To further code the data, an Excel spreadsheet was used to extract and categorize information about the study's authors, title, study design (qualitative, quantitative, or mixed methods), data collection methodology, study setting, and geographic location. Participant viewpoint (AYA male, provider, and/or parent), participant characteristics (adolescent male/young adult age, race/ethnicity of sample), proportion of previous HPV vaccination uptake, and reported barriers to uptake were also extracted. Information for each article can be found in Table 1.
Summary of Male Adolescent HPV Vaccination Uptake Included in Current Literature Review
HIS, HPV Immunization in Sons; HPV, human papillomavirus; N/A, not applicable; NIS, national teen immunization survey; PCP, primary care physician; STI, sexually transmitted infection; US, United States.
Using thematic analysis based on the procedures described by Tong et al., 13 descriptive themes were suggested by authors in isolation (K.D., J.M., and E.S.) and then later discussed as a group. Tong et al. 13 posited that there are five main domains of qualitative synthesis: introduction, methodology, literature search/selection, appraisal, and synthesis of findings. This study followed the outline composited by past research 13 coding aims, methodology, inclusion criteria, database sources, electronic search strategy, screening (e.g., title, abstract and full-text review) and data extraction, derivation of themes, and rational for appraisal (e.g., supported by past literature) in chronological order.
To further assess study quality, the modified Downs and Black Quality Checklist 14 for nonrandomized and randomized studies was used to identify individual included study quality on 27 items regarding reporting, external validity, internal validity, and power with potential scores ranging from 0 to 28, with higher scores indicating better study quality. In accordance with past literature, 14 each article was given a quality grade of “excellent” (24–28 points), “good” (19–23 points), or “fair” (14–18 points). This scale has high internal consistency (KR-20 = 0.89) and test-retest reliability (r = 0.88). Study quality ranged from 17 to 25, with an average study quality of 21.4. There were five studies considered “excellent” (21.7%), 16 considered “good” (69.5%), and two considered “fair” (8.6%). There was no study under “fair” range (<14 points) included in this systematic review.
Results
We identified common themes by reviewing the barriers described across studies. The six most common themes were: (1) lack of HPV vaccine awareness/information, (2) misinformation about HPV as a disease, (3) lack of communication, (4) financial concerns relating to uptake, (5) demographic/perceived social norms, and (6) sexual activity.
Lack of HPV vaccine awareness/information
Most articles included in the literature review (n = 19; 82.6%) noted lack of knowledge regarding the HPV vaccine and HPV in general, including among sons (6; 31.5%), parents (13; 68.4%), and providers (5; 26.3%) as a barrier to vaccination. In a study conducted by Khurana et al., 15 50% of adolescent males were unsure or did not want to be vaccinated with the HPV vaccine. Adolescent males also reported additional barriers to enrollment, including slight embarrassment,16,17 fear of side effects and needles, perceived vaccine effectiveness, dosage schedule, low HPV awareness, and perceived low susceptibility to HPV, as reasons not to vaccinate,18,19 in addition to lack of information about the vaccine overall.20–24
Across a number of studies, young adult males believed HPV vaccination was important, but only among those who viewed themselves to be at a higher risk for HPV.18,25 Some parents believed that the vaccine was more relevant when their sons reached 9–17 years of age, but a subset of this group did not wish for their children to be vaccinated because of vaccine side effects and/or because vaccination is not treated as routine for school admittance. 26 Beliefs concerning the HPV vaccine were also reported by parents, such as believing the HPV vaccine is experimental (15.1%), the vaccine causes HPV infection (7.1%), and even that it is better to get the disease and recover naturally (4.4%). 27 In some studies, however, up to 89% of parents had never heard of an HPV vaccine for males.20–23 Many parents also noted young age20,22,28,29 as a reason not to vaccinate.
Other studies, stemming from parental and adolescent son viewpoints, noted concerns for vaccine safety.16,22,27,28 Providers reported struggling to make vaccine recommendations because the HPV vaccine was not required for school admittance, they had doubts about vaccine safety,16,30–32 and it was difficult to add more vaccines to age-oriented vaccine schedules. 30
Misinformation about HPV
Misinformation regarding HPV itself was reported by parents (n = 6, 30%), AYA males (n = 3, 15.7%), and providers (n = 1, 5%). Parents reported inaccurate information or lack of knowledge regarding HPV, including what it is, how it is spread, and the consequences.20,22,24,29
As many as 54% of AYA males believed that HPV only occurred in females.16,33 Bhatta and Phillips 34 found that HPV knowledge and awareness increased 28 significantly as adolescent boys aged. Providers also reported a lack of knowledge regarding HPV risk among their AYA male patients. 34 Providers also had their own knowledge limitations with one study reporting 12% of providers lacking knowledge on when to administer HPV to AYA males and how to have conversations with their patients and their parents regarding HPV. 32
Lack of communication
Eleven articles (47.8%) reported communication barriers to vaccine uptake. Many providers noted difficulty communicating the importance of completing the HPV vaccine regimen among this population.30–32 A number of studies noted that providers did not recommend the HPV vaccine or raise awareness due to language differences 33 or personal embarrassment.30,31 Within some studies, providers reported personal discomfort talking about STIs with parents and adolescent males.16,30 Parents, however, either did not ask about the HPV vaccine or HPV 24 and/or had providers who never recommended the vaccine at all,20,23,35 especially if their own HPV knowledge was low. 24
A small group of parents expressed a desire to communicate with providers in their native language, especially if from Hispanic or Ethiopian backgrounds, explaining that they did not trust providers about these topics when speaking in English. 33
Financial concerns relating to uptake
A total of seven articles outlined financial barriers to HPV vaccination (30.4%). Both AYA males and their parents reported financial concerns as a main deterrent to the HPV vaccine, including the cost of the vaccine both out of pocket and using insurance.16,29,35 Having no or poor insurance17,23 or a household income lower than $75,00015 were notable factors in low vaccination rates. Some insurance companies did not cover the HPV vaccine for adolescent males because it was not viewed as routine36,37 or thought that this population was less susceptible to HPV infections. 31 The out-of-pocket cost of all doses of the HPV vaccine was prohibitive for some parents,16,29,30 as was the cost of doctor appointments to receive the vaccine regimen17,21,23; this burden was compounded for families with multiple children.20,36
Providers argued that the out-of-pockets cost of the HPV vaccine was unaffordable for some populations due to low insurance coverage and impacted uptake rates.31,32 In addition, physicians also face low reimbursement rates from health care insurance companies and subsequent age restrictions on HPV vaccines, 38 limiting the reach of such vaccines to older AYAs.
Demographic/perceived social norms
Seven articles (30.4%) mentioned race/ethnicity, native language, and cultural norms of parent respondents as perceived barriers relating directly to lax HPV vaccination uptake. Caucasian parents, although less likely to initiate the vaccine regimen, as opposed to African American or Hispanic participants,22,29,36,37,39 were more knowledgeable regarding HPV and the vaccine, but only after discussing this with a provider.26,41 Another study noted that Asian males were less likely to be open to vaccination compared to their Caucasian or African American counterparts. 15 English-speaking parents were less likely to believe the vaccine is necessary compared with non-English speaking parents. 23 Adolescents who were older had significantly higher rates of uptake than younger adolescents. 34
Related to parental demographics, cultural or community norms impacted vaccine uptake. 42 Schuler and Coyne-Beasley 43 found that parents whose friends or community vaccinated their sons were over four times more likely to vaccinate their own sons within the next year. In addition, Oldach and Katz 42 noted that 4.4% of providers stated that they did not recommend the HPV vaccine to families who they knew held specific religious beliefs. Community location was also found to be an important barrier to HPV education 42 and related to access to health care.16,22,24,30,37 In rural communities in the US with lower socioeconomic status, 15 providers report that discussion of a sexually oriented disease and possible prevention strategies, like a vaccine, was viewed negatively by community members. 42
Sexual activity
The sexual contraction of HPV infections remains a relevant barrier to vaccine uptake within some adolescent males. Oldach and Katz 42 found that 15.6% of providers, in more conservative areas 15 of the US, were worried that the HPV vaccine initiation and completion would encourage sexual activity, and therefore refused to recommend the vaccine. 23 A minority of adolescent males (8.1%) claimed that embarrassment of receiving a vaccine related to sexually involved diseases was enough to stop them from initiating the regimen. 23 A small portion of studies found that parents were concerned with their sons becoming sexually active,23,27 and were less likely to begin or complete the three-dose regimen. Furthermore, some parents refused the vaccine because their son was not currently sexually active, but expressed intention to vaccinate them once they became sexually active23,35 in the future.
Embarrassment was noted for parents in a small group of studies, finding that introducing the sexually oriented conversation about their son was awkward.16,17 The results of one study suggest, however, that sexual activity may act as a facilitator to HPV vaccination. Khurana et al. 15 found that a subset of AYA males who were sexually active were four times more likely to be open to receiving the vaccine regimen than those who were not sexually active. While some parents and AYA males do not vaccinate due to the beliefs surrounding sexual activity, the results of this review suggest that this is not a primary barrier to vaccine uptake, and in some cases may act as a facilitator.
Study quality score and publication date
A vast majority (69.5%) of studies included in this review were considered of “good” study quality, while 21.7% were considered “excellent,” and only 8.6% considered “fair.” The studies that scored in the “excellent” range were more recent, mainly from 2015 to 2017, with only two from 2012. Similarly, the study with the lowest study quality score of 17 was also the oldest included study, published in 2010. Most of these studies were recently published, ranging from 2014 to 2017, with a few in 2012 to 2013, and only one from 2011.
Discussion
This literature review provides a perspective on how the barriers of the HPV vaccine vary between AYA males, their parents, and providers. Moreover, there are areas that remain unexplored that deserve attention. Most articles outlined how vaccination uptake for HPV prevention, especially among AYA males, remains uncommon due to barriers from adolescents', parents', and providers' point of views. Generally, it can be suggested that the HPV vaccine uptake to prevent HPV infection among AYA males is lacking within the US. Instead of focusing solely on specific groups (i.e., adolescents, parents, or providers), it is imperative to outline common barriers and differences among these groups to further target interventions and policy changes regarding vaccination uptake among this population.
Parents, providers, and AYA males have different perspectives on potential facilitators or barriers to HPV vaccination. Among young adult males, the HPV vaccine was important to those who perceived themselves to be at increased risk for HPV,18,25 but they report several barriers to vaccination, including fear of side effects, fear of needles, perceived vaccine effectiveness, need for multiple shots, perceived susceptibility to HPV, difficulty scheduling an appointment, and HPV awareness/knowledge.18,19 Adolescents reported slight embarrassment23,32 and overwhelming misinformation20–24 as being the top reasons not to vaccinate against HPV.
The perspectives of all parties involved in these discussions are important because although vaccination intent was present in many parents, vaccination rates continue to remain low. 41 For instance, in a study conducted by Dempsey et al., parents believed that having their sons receive the HPV vaccine was important (62%), but only when their sons were between 9 and 17 years of age. 26 A subsection of parents believed that receiving the HPV vaccine would increase sons' sexual activity at a younger age. 23 Misconceptions regarding HPV and available vaccines also stemmed from parental demographics, belief systems, 42 and community pressures causing the vaccine's safety to come into question.27,29,32,40,42 Generally, Caucasian parents were more knowledgeable than African American parents regarding the HPV vaccine, but only after discussing the vaccine with a provider.26,41
It is possible that regions of the US, 23 socioeconomic status, 15 access to health care,16,22,24,30,37 and community norms20,29,42 have some impact on HPV knowledge and vaccine recommendations to parents and their sons. Future research should target various regions of the country and families of different socioeconomic statuses and backgrounds to fully encompass how these misconceptions can cause failure of HPV vaccine uptake or completion of the three-dose regimen among this population.
Providers, additionally, were also found to hold many misconceptions among this population, but the reasons for these misconceptions remain unclear. Many providers failed to recommend the vaccine or introduce HPV information,20,23,35 possibly due to language differences 33 that may make it more difficult to begin or sustain this conversation, or due to personal embarrassment regarding the subject.30,31 While this may have been noted in this review as a barrier, the World Health Organization (WHO) has introduced avenues to reduce embarrassment of all parties by suggesting the recommendation of the HPV vaccine as a cancer-preventative vaccine, removing the sexual nature of its origins, especially to younger patients. 44
Providers' recommendations remain imperative for the HPV vaccine uptake among this population, 38 but providers perceive numerous barriers to this discussion, including health care reimbursement and age-related barriers such as fears around increasing sexual activity. 38 While fears of increased sexual activity were noted among few studies further included in this review, this lapse is equivalent to what was found in previous literature and should be identified within future research. Despite widespread recommendations by providers 45 and clinical guidelines,46,47 many AYA males remain unvaccinated against HPV. If providers begin talking to adolescents at the age of nine, the youngest age recommended for beginning the HPV vaccine three-dose regimen, they may be too young to understand what it is for and its importance.20,22,23
It may be more beneficial to introduce the vaccine to the parents, and in addition, educate both parent and child about HPV and the HPV vaccine before scheduling or administering the vaccination. Increasing communication about HPV and its vaccination between these groups may increase uptake rates within this population over time. To discover the most beneficial avenues of communication between parents, providers, and AYA males, future research should examine what communication methods are associated with male willingness to be vaccinated and completion of the HPV vaccine three-dose regimen.
It is apparent that lack of communication between all parties may rely on preconceived notions about who should initiate the conversation about HPV and its prevention. Overwhelmingly, parents would not ask about HPV or the HPV vaccine regarding their AYA sons, 24 possibly not knowing enough about the subject to do so. Embarrassment, especially in the presence of adults, may stem from the sexually oriented conversation at doctors' appointments, possibly with parental overview.16,17 HCPs have the ability to influence vaccination uptake among adolescent males and their families. Brewer 47 discussed that vaccinating urgently, listing the HPV in the middle of recommended vaccines, noting child's risk, and easing parent concern all increased vaccination uptake drastically, more so than the unstructured current process.
HCP training, as related to HPV vaccination uptake among adolescent males, has been few and far between. Yarwood and Bonanni 48 have discussed training avenues to improve HPV vaccination uptake, including 30% improvement by verbal recommendation. Continuing education for HCPs in vaccinology, allowing questions during office visits, comprehendible materials, and the use of layterms when speaking with patients and their parents are imperative for vaccination uptake. 48 More information is required to pinpoint exact causes of misinformation among parents and providers to better understand these phenomena.
This review must be interpreted considering its limitations. The search results may have been updated through the editing process, making it possible that additional articles may be published now, which could have been included in this review. Some relevant articles may have been missed, which were published in press, dissertations, conference proceedings, and/or results not yet published. In addition, it is possible that policy and legislation concerning vaccination and HPV among this population have changed since this review. Since this review only included US studies, generalizability to other countries and areas outside of the US remain limited.
Implications and Future Directions
HPV-related cancers are increasing, and therefore, increasing vaccination is imperative.2,49 For instance, HPV-associated oropharynx cancer incidence has increased 225% over the past three decades. 2 Barriers associated with HPV vaccination include AYA embarrassment as well as lack of provider knowledge regarding this specific population. This is particularly concerning, as provider recommendation is one of the most important factors for vaccination uptake. Increasing provider knowledge may be imperative for reducing incidence of HPV-related cancers as well as improving lines of communication between all groups.
Future health policy should focus on involving the HPV vaccine as one of the vaccines adolescents require before enrollment in school within the US. Future research should also identify which groups and regions of the US have lowest HPV vaccination uptake rates overall and make the vaccine more accessible and affordable in those locations.48–53 In addition, HCP communication methods should be studied to identify ideal comfort for the HCP and patient. 53 Policy should influence how HCPs recommend specific vaccines, such as the HPV vaccine, and should be trained to do so, to further increase vaccination uptake among this population.
Conclusions
Evidence suggests the HPV vaccine is an effective vaccination against cancer and genital warts in AYA males, but AYA males, their parents, and providers report many barriers to vaccination. While parents, providers, and adolescent males may differ in relation to their barriers, they did show many similar traits, including fear of side effects, 15 HPV awareness/knowledge,18,19,50 financial costs,15,36,51,52 and changes in sexual activity. 38 It remains imperative to increase communication between these groups to facilitate more discussion regarding HPV and the HPV vaccine among this population in hopes of increasing the number of males fully vaccinated to protect themselves and future partners.
Footnotes
Acknowledgments
We want to thank our second outside reviewer (Abdul Khaleque) for his role in reviewing our completed project.
Author Disclosure Statement
No competing financial interests exist.