
Abstract
Purpose:
Childhood brain tumors (CBTs) and their treatment increase the risk of secondary neoplasms (SNs). We studied the incidence of secondary craniospinal tumors with magnetic resonance imaging (MRI) screening in a national cohort of survivors of CBT treated with radiotherapy, and we analyzed the Finnish Cancer Registry (FCR) data on SNs in survivors of CBT with radiotherapy registered as a part of the primary tumor treatment.
Methods:
A total of 73 survivors of CBT participated in the MRI study (mean follow-up of 19 ± 6.2 years). The incidence of SNs in a cohort of CBT patients (N = 569) was retrieved from the FCR (mean follow-up of 11 ± 12.9 years). Brain tumors were diagnosed at age ≤16 years between the years 1970 and 2008 in the clinical study and the years 1963 and 2010 in the FCR population.
Results:
Secondary brain tumors, meningiomas in all and schwannoma in one, were found in 6 of the 73 (8.2%) survivors with a mean of 23 ± 4.3 years after the diagnosis of the primary tumor. The cumulative incidence was 10.2% (95% confidence interval [CI] 3.9–25.1) in 25 years of follow-up. In the FCR data, the 25-year cumulative incidence of SNs was 2.4% (95% CI 1.3–4.1); only two brain tumors, no meningiomas, were registered.
Conclusion:
Survivors of CBT treated with radiotherapy have a high incidence of meningiomas, which are rarely registered in the FCR.
Introduction
The risk of secondary neoplasms (SNs) after childhood cancer is increased, especially after radiotherapy.1–4 Exposure to ionizing radiation has been associated with the evolution of brain tumors, such as meningiomas and gliomas.5,6 A significantly elevated risk for a secondary brain tumor has been associated with the first neoplasm being either a central nervous system (CNS) tumor or leukemia, exposure to radiotherapy, and having a genetic risk factor for cancer.4–8
Ionizing radiation has carcinogenic potential. 9 Chromosomal injury after exposure to higher doses of radiation accelerates the loss of cellular control mechanisms, causing neoplasms to appear earlier. 10 Lower doses of radiation at the border of the radiation field are insufficient to induce cell death, which may explain the occurrence of SNs in these areas.10,11 How chemotherapy affects the risk of developing a secondary brain tumor is not well understood, but alkylating agents and epipodophyllotoxins are known to cause DNA changes that may result in tumors.8,12–14 Chemotherapy may also have an additive effect on the carcinogenic potential of radiotherapy. 15
Whether growth hormone (GH) treatment may actually increase the risk of the development of SNs is a concern.16–19 Meningiomas and gliomas express receptors for GH and insulin-like growth factor 1 (IGF1), both of which have been shown to be mitogenic and promote cell survival.19–21 Recent studies have not shown an increased risk of primary brain tumor recurrence or an increased risk of SNs after GH replacement therapy.19,20,22–24
Most of the previous studies of SNs among childhood cancer survivors are register-based or retrospective studies.1–5,7,15,25,26 Cranial magnetic resonance imaging (MRI) screening studies have been conducted in leukemia, lymphoma, and childhood cancer survivors, including a group of childhood brain tumor (CBT) survivors treated with cranial radiotherapy.12,27–29 We could not find any previous studies focusing on CBT survivors using craniospinal MRI screening.
Larjavaara et al. estimated the actual incidence of meningiomas to be one-third higher than that indicated in the Finnish Cancer Registry's (FCR) records. 30 The estimation was based on the identification of cases from different hospital databases, as well as comparison of these results to the FCR data of the hospital district. 30 In this study, we present the occurrence of secondary brain tumors in a cohort of Finnish CBT survivors, observed in MRI screening, and the incidence of SNs reported to the FCR.
Materials and Methods
Clinical study population
The patients were identified from the local registers of Oulu, Kuopio, Turku, Tampere, and Helsinki university hospitals, where all CBTs were treated in Finland between the years 1970 and 2008.
The inclusion criteria of the study were as follows: (i) the brain tumor diagnosed at the age of ≤16 years, (ii) radiotherapy as a part of the treatment, (iii) the patient's age at the time of the study ≥16 years, (iv) the follow-up time since the cessation of tumor therapy ≥5 years, and (v) no progressive disease at the time of the study. In addition to radiotherapy, the treatment of the primary tumor could have included operation(s), shunt operation(s), and chemotherapy.
Parameters measured
Participants were examined with craniospinal MRI and clinical examination. Clinical files were reviewed for previous secondary tumors, treatment of primary brain tumor, and hormonal therapy.
Craniospinal MRI
Scans were performed by using a Magnetom Espree 1.5T scanner in Oulu, a Siemens Avanto 1.5T scanner in Helsinki, Kuopio, and Tampere (Siemens, Erlangen, Germany), and a Phillips Ingenia 1.5T scanner in Turku (Phillips Healthcare, Amsterdam, the Netherlands). Cranial MRI protocol included the following pulse sequences: T1-weighted spin-echo (SE) sagittal, T2-weighted SE axial, T2-weighted fluid-attenuated inversion recovery axial, T1-weighted 3D inversion recovery SE coronal, diffusion-weighted imaging axial, and 3D time-of-flight magnetic resonance angiography. Gadolinium contrast agent (Dotarem, 0.2 mL/kg, Guerbet, France) was used in T1-weighted SE axial and T1-weighted SE coronal sequences. A spinal MRI was imaged after contrast-enhanced brain MRI and included T1-weighted turbo spin echo (TSE) sagittal and T2-weighted TSE sagittal sequences.
MRI scans were evaluated on a research PACS/DICOM viewing application for diagnostic radiology: neaView (Neagen, Helsinki, Finland) in Oulu, Sectra Workstation IDS7 version 19.1.10.3584 (Sectra AB, Linköping, Sweden) in Kuopio, and Agfa Impax version 6.6.1.5551 2017 (Agfa Health care N.V., Mortsel, Belgium) in Helsinki. MRIs were analyzed by four radiologists (M.S-P., A.S., P.K., and S-M.T-S.) and re-evaluated by M.S-P.
Contrast enhancement was not used in 12 participants because of their creatinine levels (n = 5), chronic renal insufficiency (n = 1), previous nausea during infusion (n = 2), previous allergic reaction (n = 1), problems in cannulation (n = 1), and unknown reasons (n = 2).
Radiation analyses
Medical physicists analyzed the radiation doses by using patient charts and field images. Exact 3D doses were not available for all patients. The field images and treatment plans of two patients with secondary brain tumors were unavailable.
Hormonal analyses
The blood samples were collected after overnight fasting between 7:30 AM and 10:00 AM, and they were analyzed in Nordlab, Oulu University Hospital. IGF1 and insulin-like growth factor binding protein 3 (IGFBP3) were analyzed with the immunoassay method (Immulite 1000 Immunoassay, Siemens Health care, Munich, Germany). Blood samples could not be collected for one subject.
The FCR study
The FCR is a population-based nationwide registry that has collected data on all cancers diagnosed in Finland since 1953. The coverage of the FCR data has been proven to be adequate and almost complete, but the benign neoplasms of the CNS are under-registered. 31 Data are based on tumors with International Classification of Diseases (version 10) codes C70–72, D32–33, and D42–43, as well as any secondary malignancies of these cases. The FCR population in this study met the following criteria: (i) the brain tumor diagnosed at age 0–16 years between 1963 and 2010 and (ii) radiotherapy registered as a part of the primary tumor treatment. The date of the diagnosis of primary brain tumors, the presence of chemotherapy as a treatment for primary cancer, the date of the diagnosis of the secondary cancer, the histology of the secondary cancer, and the date of death were retrieved from the registry.
Statistics
Analyses were carried out with the following statistical programs: IBM SPSS Statistics for Windows version 24.0 (IBM Corp, Armonk, NY), StatsDirect Statistical software version 3 (StatsDirect Ltd 2013, England), and Stata Statistical Software: Release 13 (StataCorp LP, StataCorp. 2013 College Station, TX) An exact chi-square test was used to evaluate the relationship between categorical variables and study groups. Differences between two proportions were compared by using the standardized normal deviate test. For continuous variables, Student's t test was used to determine whether the means between those with and without SNs differ.
The association between secondary tumors and a set of explanatory variables: age at the diagnosis, follow-up time since the diagnosis of the primary tumor, radiation dose in Gray (Gy), measured levels of IGF1 in nM, body mass index in kg/m2, sex, and mode of radiation therapy (local or whole brain with/without spinal radiation) was examined by a multivariate logistic regression model with enter methods. The Kaplan-Meier estimator was used to calculate the cumulative incidences for clinical data. For FCR data in which death was present as a competing risk, the cumulative incidence function was estimated by using the Fine-Gray method.
Ethics
Written informed consent was obtained from all the enrolled subjects and/or their legal guardians for the clinical study. The study was approved by the Institutional Review Boards of all the university hospitals, Finland. The research was conducted according to the principles of the Declaration of Helsinki. Permission to obtain data from the FCR was granted by the National Institute for Health and Welfare.
Results
Patient characteristics in the clinical study
Of the 127 subjects initially identified as eligible, 74 (58%) participated. Two participants were not examined with craniospinal MRI because of vagus nerve stimulator (n = 1) and claustrophobia (n = 1). A subject with vagus nerve stimulator was followed up previously on a clinical basis with MRI for secondary brain tumors. The information from his previous images and the treatment details were added to the final analysis, increasing the total number of subjects to 73.
The mean age of diagnosis of the primary tumor was 8.4 ± 4.3 years and at the follow-up visit, it was 28.4 ± 6.8 years. The mean follow-up duration was 19.9 ± 6.2 years. A total of 40 eligible subjects declined to participate, and 13 were lost to follow-up. The group of participants did not differ statistically from non-participants with respect to patient, disease, or treatment characteristics. 32
Radiotherapy was carried out by using photons. The treatment techniques and doses varied. Some treatments only consisted of fields for part of the brain, whereas others had a combination of spinal field, whole brain, and booster to a part of the brain.
Chemotherapy was used in 46 subjects. Protocols varied because of the histology of the tumor and the period of treatment. The
The survivors had not been systematically followed up for their GH status in the adult clinics, and they have been rarely treated.
Clinical study
In the clinical study, 6 of 73 (8.2%) participants were diagnosed with radiation-induced meningiomas. The cumulative incidence was 2.0% (95% confidence interval [CI] 0.3–13.6) in 20 years and 10.2% (95% CI 3.9–25.1) in 25 years of follow-up (Fig. 1A). Subjects with meningiomas had ependymoma (n = 3), medulloblastoma (n = 1), meningioma (n = 1), and astrocytoma (n = 1) as their primary brain tumor.
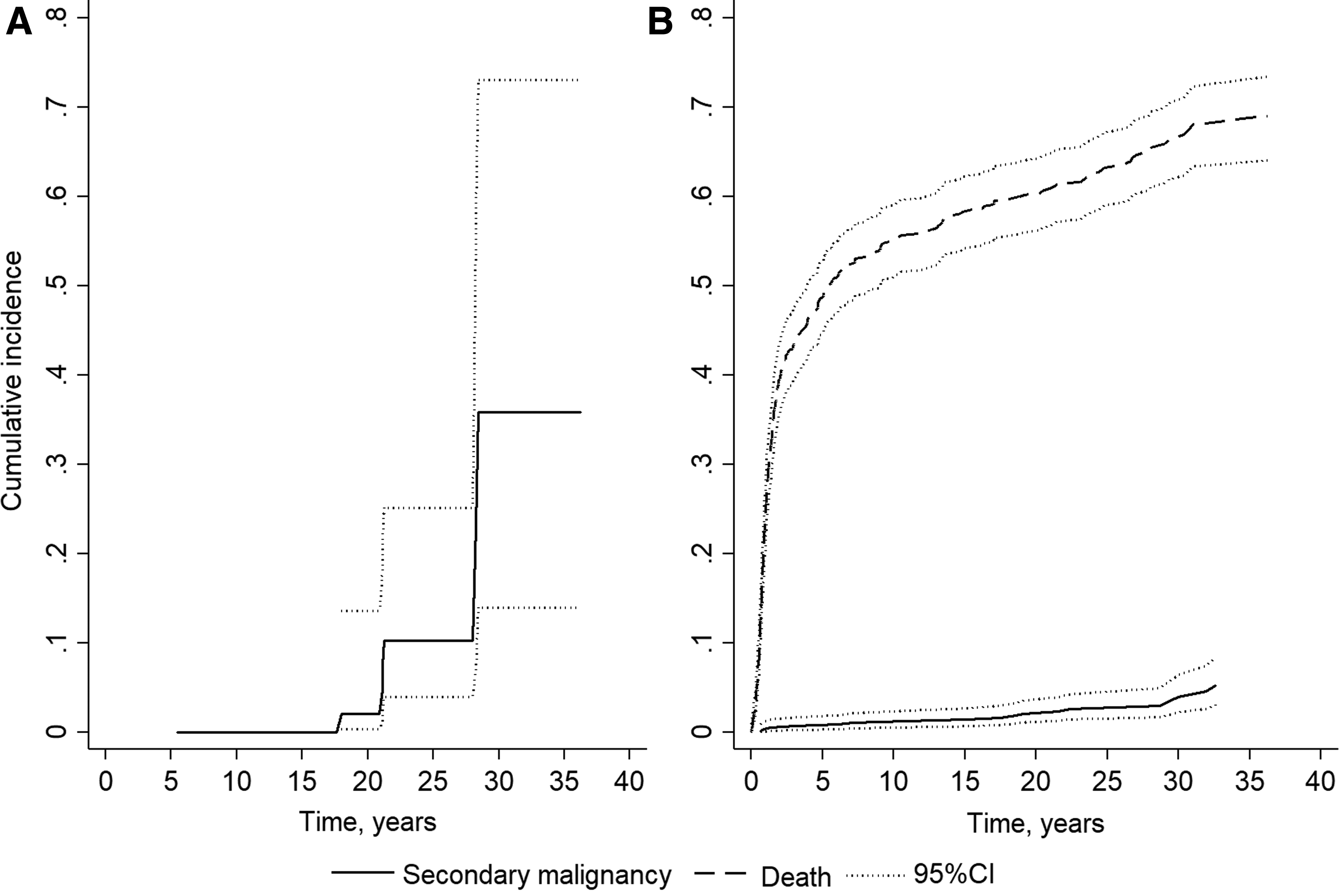
Cumulative Incidence for Radiation-Induced Meningiomas in the Clinical Data
In six subjects, brain MRI showed brain tumors with the typical radiological characteristics of meningioma. In three of them, meningiomas were not previously diagnosed (Fig. 2, Panel 1). Patients had no symptoms from the tumors.
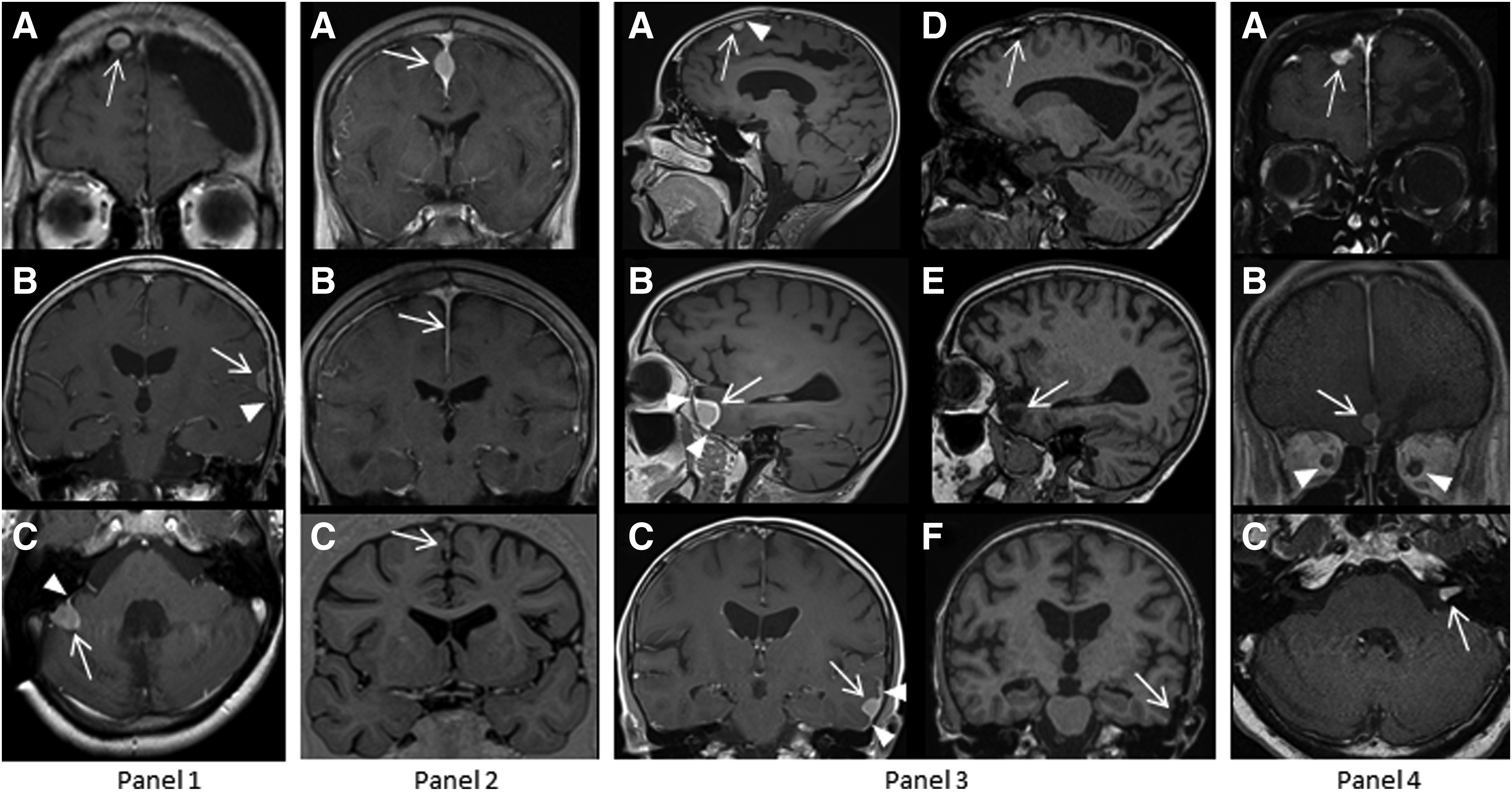
Secondary Benign Brain Tumors in the Clinical Data. Panel 1: Meningiomas of different subjects on contrast-enhanced T1-weighted (T1W) MRI
SNs were previously diagnosed in 3 of the 73 (4.1%) participants (Fig. 2, Panels 2–4). Two subjects were operated on because of meningiomas; one of them was found to have a relapse in the study MRI (Fig. 2, Panel 2). Another subject underwent two operations for three meningiomas before the study (Fig. 2, Panel 3). One subject was followed up for a vestibular schwannoma, three meningiomas, and thickening of the optic nerves (Fig. 2, Panel 4). No secondary spinal tumors were observed in the studied subjects.
The mean age at the diagnosis of the first meningiomas was 30.0 ± 8.1 years and the mean follow-up time since the diagnosis of the primary tumor was 23.0 ± 4.3 years. Primary tumor and treatment characteristics were not associated with the occurrence of meningiomas (Table 1).
Tumor Characteristics, Tumor Treatment, and Growth Hormone-Related Measures in the Clinical Study
Student's t test.
Chi-square exact test.
Follow-up time since the diagnosis of the primary tumor to the diagnosis of the secondary tumor or to the follow-up visit.
n = 66.
Definition of GH deficiency is low IGF1 and/or IGFBP3 and/or GH replacement therapy.
CI, confidence interval; GH, growth hormone; IGF1, insulin-like growth factor 1; IGFBP3, insulin-like growth factor binding protein 3.
The cyclophosphamide equivalent dose was calculated according to the study of Green et al. 45
Two subjects with meningiomas received local radiotherapy for their primary brain tumor, and four of six were treated with whole-brain radiation (Table 1). The total dose of radiation to the primary brain tumor was higher in those subjects with meningiomas than those without, although the finding was not statistically significant (p = 0.075) (Table 1).
In four subjects with radiation field charts available, all six meningiomas were situated outside the primary target volume area of the prescribed treatment dose: four were in the whole-brain volume (dose of radiation 34.5 Gy [n = 1], 36 Gy [n = 2], and 48 Gy [n = 1]) and two in the field border area (dose of radiation <51.2 Gy and <54 Gy). The subject with multiple meningiomas had one meningioma in the field border (dose of radiation <54 Gy) and two meningiomas in the low-dose area (dose of radiation 36 Gy). Chemotherapy was part of the treatment for the primary tumor in four of six subjects with meningioma (Table 1).
All subjects with meningiomas had GH deficiency (low IGF1 or IGFBP3 or GH replacement therapy), and the difference was statistically significant compared with those without meningiomas (p = 0.009) (Table 1). Current or previous GH replacement therapy was not associated with radiation-induced meningiomas (Table 1).
In the multivariate regression analysis, the total dose of radiation (adjusted OR 1.43; [95% CI 1.04–1.96]; p = 0.027) and whole-brain radiation (adjusted OR 43.3; [95% CI 1.75–1067.01]; p = 0.021) was associated with meningiomas (results not shown).
Patient characteristics of the FCR data
A total of 569 cases were identified from the FCR to meet the inclusion criteria. Of these, 194 (34.1%) were alive at the time of data collection. The mean age at diagnosis of the primary tumor was 7.6 ± 4.2 years and at the end of the follow-up, it was 33.5 ± 10.1 years. The mean follow-up time since the diagnosis of the primary tumor was 11.8 ± 12.9 years. Chemotherapy was registered as a part of the treatment of the primary tumor in 194 of the 569 (34.1%) cases.
FCR data
Only two secondary brain tumors were reported in the 569 FCR registered cases (0.35%): ganglioneuroma or ganglioneuroblastoma of posterior fossa and grade 3 primitive neuroectodermal tumor. No secondary meningiomas were registered in the FCR. SNs were reported in 18 of the 569 (3.2%) registered cases and 8 of the 194 (4.1%) cases who were alive at the time of data collection (Table 2). The cumulative incidence of SNs was 1.5% (95% CI 0.7–2.8) in 20 years and 2.4% (95% CI 1.3–4.1) in 25 years of follow-up (Fig. 1B). Those SNs reported in the FCR were associated with a high mortality rate because 10 of the 18 (55.6%) cases with SN
Associations Between Tumor Characteristics and Tumor Treatment Modalities in Patients With or Without Secondary Neoplasm in Finnish Cancer Registry Data
Student's t test.
Age at the diagnosis of secondary neoplasm, at the death, or at the retrieval of the registry.
Follow-up time since diagnosis to the diagnosis of secondary neoplasm or to the retrieval of the registry.
n = 10.
n = 361.
Significant level 0.05.
Standardized normal deviate test.
Chi-square exact test.
The most common SNs were basal cell tumor (n = 5) and hematological malignancies (n = 4). The other SNs registered were ovarian tumors (n = 2), endocrinological epithelial tumor of the Fallopian tube (n = 1), papillary adenocarcinoma of the thyroid (n = 1), breast cancer (n = 1), melanoma (n = 1), and neurilemmoma of the autonomic nervous system (n = 1).
Discussion
In our cohort of irradiated CBT survivors studied with MRI screening, we observed a crude incidence of 8.2% after 19 years of follow-up and a cumulative incidence of secondary meningiomas of 10.2% at 25 years of follow-up. The incidence of radiation-induced meningiomas in CBT survivors was lower in this cohort than in those in earlier screening studies with cranial MRI.12,27–29
In a cohort of childhood cancer survivors treated with cranial radiotherapy, the crude incidence was 17% after a median follow-up of 24 years. 28 In two studies of childhood leukemia survivors treated with radiotherapy, the reported cumulative incidence was 15% and 47% at 20 years of follow-up.12,27 In the leukemia treatment protocols, the doses of cranial radiotherapy are lower, but the treatment includes repeated injections of intrathecal methotrexate, which is rarely used in the treatment of brain tumors.12,27–29 Taylor et al. showed that intrathecal methotrexate and higher radiation doses increase the risk of secondary meningiomas. 37
The cumulative incidence is slightly higher than that reported on patients treated with radiotherapy of 50 Gy or more (7.1%). 7 As in earlier studies, the incidence increased sharply in the follow-up.7,12 The crude incidence reported earlier in register-based and retrospective studies (0.4%–4.2%) was lower than that in our study (8.2%).7,38,39 This difference can be explained by the detection of asymptomatic meningiomas during the screening. Meningiomas rarely appear in the spine, which may explain why no spinal meningiomas were detected. 40
No meningiomas were registered in the FCR. The differences in the SNs between the clinical and FCR data can be explained by the high SN mortality of the FCR population. Malignant secondary brain tumors seem to appear earlier in the follow-up and have a high mortality.8,24 Meningiomas in the clinical study appeared to be asymptomatic, and according to earlier studies, seemed to manifest later in the follow-up.8,24
Similar to previous reports, we found that increasing the total dose of radiation increases the risk of intracranial SNs.4,37 This may represent the intensity of the overall treatment, as the analyzed secondary meningiomas were situated outside the primary target volume. This finding is in line with that of Galloway et al. that the most common location of the second tumor was in the whole-brain field.
11
Armstrong et al. suggested that chemotherapy potentiates the effect of radiation on the development of SNs.
No association has been demonstrated between SNs or meningiomas nor relapse of the primary tumor and GH replacement therapy.16,19,20,22,24 Our results suggest that GH deficiency, but not replacement therapy, may be associated with secondary meningiomas. Both secondary meningiomas and GH deficiency have been shown to be associated with an increasing dose of radiation and a longer follow-up time; therefore, whether GH deficiency is a marker of higher radiation doses or a longer follow-up time or whether a true association exists remains unknown.4,24,41
Children's Oncology Group guidelines stipulate that the brain MRI is indicated in symptomatic patients and every other year in patients with neurofibromatosis. 42 In previous screening studies, large meningiomas with mild or no symptoms have been detected.28,29 These findings have led to a discussion on whether early detection of lesions would lead to successful complete resection.12,27–29 Current evidence on the benefits of screening is lacking.
The strength of our study is that we have systematically examined a national cohort of CBT survivors treated with radiotherapy with MRI screening. The participation rate (58%) in our study is similar to that of previous cohort studies in CBT survivors treated with radiotherapy.41,43,44 Participants and non-participants did not differ in the tumor or treatment characteristics, but information on their current psychosocial status was lacking; therefore, selection bias cannot be ruled out. The heterogeneity of the study population, as well as the small number of SNs in clinical and register-based data, however, limits the statistical methods used in this study. In the multivariate analysis, a potential confounding factor could be the higher incidence of GH deficiency in those subjects with a higher radiation dose and a longer follow-up time.
In conclusion, we report a high incidence of radiation-induced meningiomas found by MRI screening in long-term CBT survivors treated with radiotherapy. Secondary meningiomas were not reported to the FCR, which partially explains the higher incidence of SNs in the clinical study.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to the following foundations for their support to this study: Special State Grants for Health Research in the Department of Pediatrics and Adolescence, Oulu University Hospital, Finland; Väre Foundation for Pediatric Cancer Research, Finland; Foundation of Päivikki and Sakari Sohlberg, Finland; Foundation of Arvo and Lea Ylppö, Finland; Foundation for Pediatric Research, Finland; Foundation of Emil Aaltonen, Finland; Cancer Society of Finland; Foundation of Thelma Mäkikyrö, Finland; Cancer Foundation of Northern Finland; Foundation of Alma and K.A. Snellman, Finland; and Foundation of Märta Donner, Finland. They likewise thank child oncologist Marika Grönroos for her kind help in investigating some patients. Finally, they thank the survivors, their families, and the group homes for their contribution to this study.
Author Disclosure Statement
T.M.R. has received financial support for attending symposia of the Cancer Foundation of Northern Finland, Foundation of Arvo and Lea Ylppö, Finland, Foundation for Pediatric Research, Finland, PtcBio, Orion Pharma, and Biogenes. P.M.A. has received financial support for attending symposia of Abbvie and Alexion. P.M.L. has received financial support for attending symposia of Shire, Sobi, Bayer, and Cancer Foundation of Finland. M.O.A. has received financial support for attending symposia of Sobi and Pfizer. V.P.R. is an advisory board member in Bayer, Novo, Pfizer, Shire, and Sobi. T.R.I.L. has received a speaker honorarium from Actelion Pharmaceuticals and Biomarin. M.K.O. has received financial support for attending symposia of Novo Nordisk and Merck. She has received a speaker honorarium from Algol, Pfizer, Merck, and Sandoz. She has also received a grant from the Emil Aaltonen Foundation Finland and the Cancer Society of Finland.
All other authors have no conflicts of interest.