
Abstract
The role of mediastinal radiotherapy (RT) in primary mediastinal large B cell lymphoma is controversial. We used the Surveillance, Epidemiology and End Results program 18 database to identify the role after rituximab approval. Among 474 patients included, 65.8% were 18–39 years old and 34.2% were 40–59 years old; 45.8% received RT. Univariate analysis showed that disease stage and race could affect survival. After adjusting for stage and race, RT was correlated with prognosis in patients aged 40–59 years (none/unknown vs. RT, hazard ratio = 2.898, p = 0.034). However, in patients aged 18–39 years, this impact was not significant. Omission of RT in selected young patients may be considered.
Introduction
Primary mediastinal large B cell lymphoma (PMBCL) is a distinct entity of diffuse large B cell lymphoma (DLBCL), accounting for 2%–3% of all non-Hodgkin lymphoma cases,1,2 which is believed to arise from a putative thymic medulla B cell. 3 Based on the U.S. population data from the National Cancer Institute's Surveillance, Epidemiology and End Results program (SEER) database, <500 patients were diagnosed with PMBCL and the annual incidence rate was 0.4 per million from 2000 to 2012. 4 PMBCL is more common in young adults, especially in women. In the post-rituximab era, first-line immunochemotherapy along with consolidative mediastinal radiation is widely applied and has demonstrated high curability,5–8 thus bringing the issue of long-term side effects such as second primary cancer and increased coronary artery disease to health care practitioners, especially for those exposed to radiotherapy (RT).
The International Prognostic Index (IPI), which includes five parameters (stage III/IV, age >60 years, elevated serum concentrations of lactate dehydrogenase, Eastern Cooperative Oncology Group [ECOG] performance status ≥2, and involvement of more than one extranodal site), has been shown to be useful in predicting the outcome of de novo DLBCL patients. 9 Besides, other prognostic tools such as R-IPI (revised IPI), aaIPI (age-adjusted IPI), and NCCN-IPI were subsequently developed for better prediction in newly diagnosed DLBCL.10,11 In spite of optimization of prognostic tools, their predictive potential in PMBCL is not as convincing as in general DLBCL, partially due to the age distribution and limited-stage predominance. Several indicators, including poor performance status, pericardial effusion at presentation, and response to first-line treatment, have been reported to be correlated with poor survival. 12
Hence, in this population-based study, we aim to identify prognostic parameters and evaluate the role of radiation therapy in the rituximab era among PMBCL patients in different age groups.
Methods
Clinical variable measures
Based on the U.S. population-based SEER 18 Regs Custom Data (with additional treatment fields), November 2016 Sub (1973–2014 varying), PMBCL cases younger than 60 years old, diagnosed during the period January 2001 to December 2014, were included. PMBCL was identified according to the Lymphoma Subtype Recode/WHO 2008, which is updated for hematopoietic codes on the basis of World Health Organization International Classification of Diseases for Oncology, Third Edition (ICD-O-3), 13 and WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (2008). 14 Age at diagnosis, year of diagnosis, sex, race, Ann Arbor stage, receipt of radiation therapy (none/unknown or Beam radiation or other), receipt of chemotherapy, survival months, and vital status were collected in the current study. Patients without chemotherapy treatment and patients with missing information for sex, race, age at diagnosis, Ann Arbor stage, survival months, and vital status were excluded from the analysis.
Statistical analysis
Pearson's chi-square test was used to compare differences in patient characteristics according to different age groups (18–39 vs. 40–59 years). Age at diagnosis was presented as median with interquartile range (IQR). The Kaplan–Meier method was used to calculate survival curves, which were compared using log-rank tests in univariate analysis. Multivariate survival analysis was performed by Cox proportional hazards regression. The hazard ratio (HR) and 95% confidence interval (CI) were calculated. Statistical analysis was conducted using SPSS 22.0 (SPSS, Inc., Chicago, IL). All tests were two-tailed, and a p-value <0.05 was considered statistically significant.
Results
A total of 586 patients with PMBCL have been identified. After excluding patients without chemotherapy treatment (n = 39); missing stage information (n = 4) or race information (n = 4); and ≥60 years old or missing age information (n = 65), 474 patients were included for analysis. Among the entire cohort (n = 474), 180 (38.0%) were male and 294 (62.0%) were female; the median age was 38 (IQR: 28–43) years; 312 (65.8%) were 18–39 years old and 162 (34.2%) were 40–59 years old at PMBCL diagnosis; 89 (18.8%) were diagnosed during the period 2001–2005 and 385 (81.2%) were diagnosed during the period 2005–2014; the majority (n = 367, 77.4%) were of white race, followed by black race (n = 54, 11.4%), and American Indians/AK Natives or Asians/Pacific Islanders (53, 11.2%); 217 (45.8%) received RT and 257 (54.2%) were marked as not or unknown; and 378 (79.8%) were categorized as stage I/II disease and 96 (20.3%) as stage III/IV.
Demographic and clinical stages and use of RT in the study population were summarized according to different age groups (Table 1). There was no significant difference in patient characteristics between the two age groups.
Demographics and Clinical Characteristics of the Study Population (n = 474)
In the entire group (n = 474), the 5- and 10-year overall survival (OS) rates were 87.2% and 81.9%, respectively. Univariate analysis showed that the two factors affecting patient survival were Ann Arbor stage (I/II vs. III/IV; 5-year OS 89.4 vs. 78.5%, p = 0.006) and race, with the 5-year OS rate significantly higher in white patients than in other (American Indian/AK Native or Asian/Pacific Islander) patients (84.8 vs. 75.6%, p = 0.046). Other indicators, including age group (p = 0.517), sex (p = 0.994), year of diagnosis (p = 0.614), RT (p = 0.437), and marital status (p = 0.731), did not significantly influence OS. Multivariate analysis was performed, which established that only the Ann Arbor stage remained as an independent indicator of OS in patients with PMBCL (Table 2).
Univariate Analysis and Multivariate Analysis of the Prognostic Factors of Overall Survival in Patients with Primary Mediastinal Large B Cell Lymphoma
American Indian/AK Native or Asian/Pacific Islander.
CI, confidence interval; HR, hazard ratio; OS, overall survival.
Furthermore, survival analysis was conducted in the patients subgrouped by age. After adjusting for disease stage and patient race, mediastinal RT in patients with PMBCL was correlated with prognosis in patients aged 40–59 years (none/unknown vs. radiation, HR = 2.898, 95% CI: 1.082–7.760, p = 0.034). However, in patients aged 18–39 years, this impact was not significant (none/unknown vs. radiation, HR = 0.676, 95% CI: 0.338–1.350, p = 0.267) (Fig. 1).
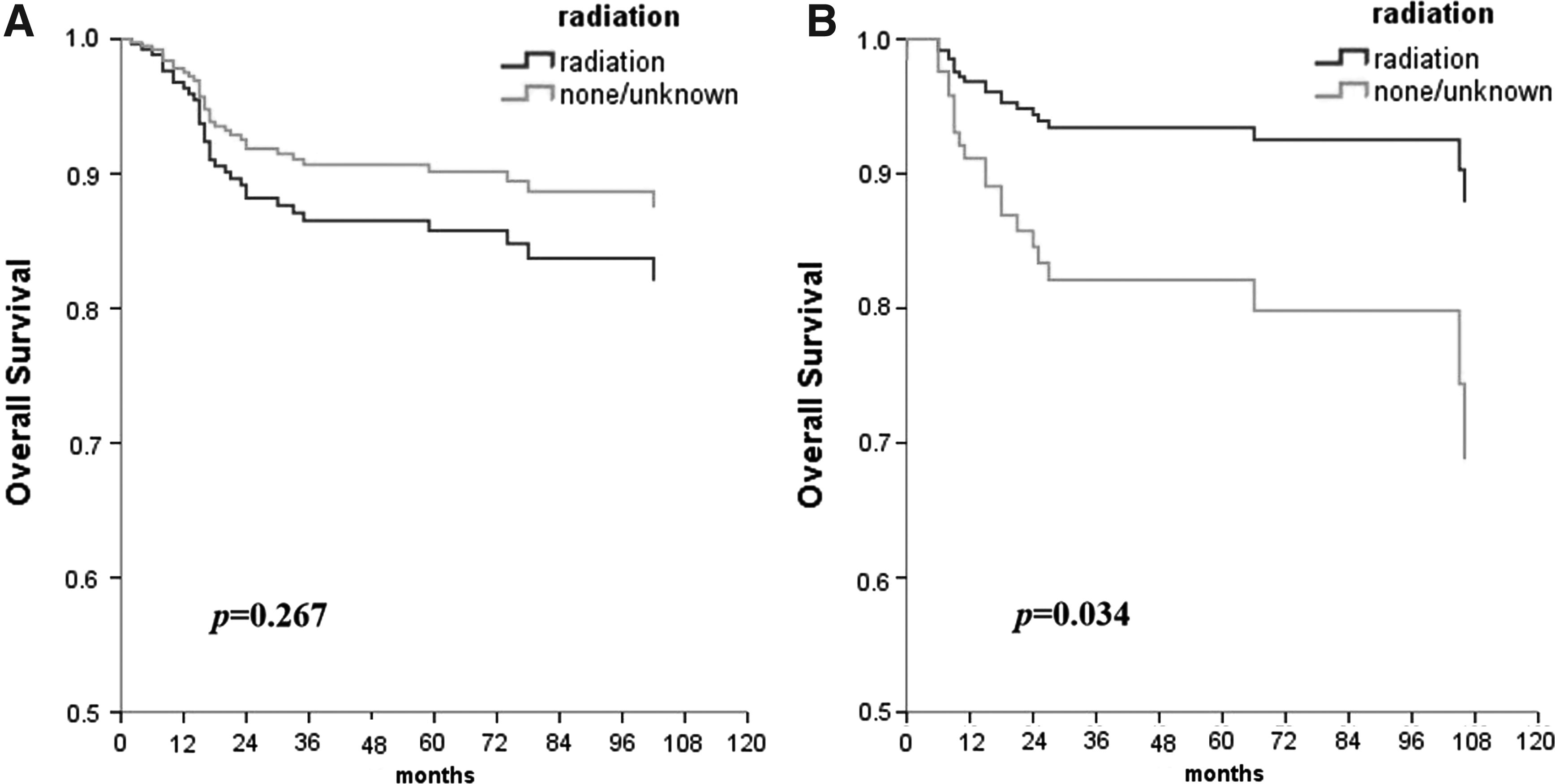
Overall survival of PMBCL patients treated and stratified by receipt of radiotherapy in
Discussion
This literature suggests that RT may offer survival benefit in middle-aged patients (40–59 years), but not in young adults (18–39 years). Additionally, disease stage is the only significant predictor of patient survival in the entire cohort.
We identified patients with PMBCL from 2001 to 2014 in our study. Patients who were 60 years or older were rare (n = 38) and were excluded from analysis because age has been recognized as a predictor in DLBCL. In fact, patients aged 60 years or older had significantly worse survival than their younger counterparts in this cohort, with 5-year OS of 41.0% (p < 0.001), mostly because of immune response deterioration, comorbidities, and unfavorable organ reserves. 15 Thus, we included those younger than 60 years in our study. Similar to previous evidence, 12 disease stage remained as an independent predictor of patient survival.
Although addition of anti-CD20 monoclonal rituximab to front-line chemotherapy has significantly yielded survival benefit in PMBCL,5–8 relapse and refraction still exist with 3-year event-free survival (EFS) of 78% in the post-rituximab era. 6 Mediastinal consolidative RT has been introduced in the hope of improving prognosis. However, different from general DLBCL, PMBCL is often seen in young adults with female predominance. Thus, long-term toxicities of mediastinal radiation such as second malignancies and increased coronary artery disease are of concern, which make the role of consolidative RT controversial in this population.
Previously, it has been indicated that RT could bring benefit to PMBCL patients regarding both EFS and OS.16,17 Nevertheless, some studies have failed to identify statistically significant benefit of RT in PMBCL patients responding to first-line immunochemotherapy.5,7 Taking long-term toxicity into consideration, it is important to balance the increasing cure rate, minimizing side effects in the young population with PMBCL.
Dunleavy et al. had conducted a prospective phase 2 study with 51 PMBCL patients enrolled. They found that the use of DA-EPOCH-R (dose-adjusted etoposide, doxorubicin, cyclophosphamide, vincristine, prednisone plus rituximab) not only could obviate the need for RT in all but 2 (4%) patients but also had a favorable 3-year OS rate of 97% and EFS of 93%. In this study, post-treatment fluorodeoxyglucose (FDG)-positron emission tomography (PET)-computer tomography (CT) was used to identify patients with persistent disease and need for RT. Although FDG-PET-CT showed a positive predictive value of 17%, the negative predictive value was 100%. 18 Thus, consolidative RT could possibly be omitted in PET-negative PMBCL patients to avoid long-term side effects of mediastinal RT.
Results of the IELSG-26 Study 19 confirmed the utility of FDG-PET-CT. With liver uptake as the cutoff for PET positivity, patients were discriminated most effectively between high and low risk of failure, with 5-year PFS of 99% versus 68% (p < 0.001). Results also suggested that few patients with post-immunochemotherapy PET negativity could benefit from consolidation RT. Furthermore, the ongoing International Extranodal Lymphoma Study Group-37 Study aims to address the need for consolidation mediastinal RT in patients obtaining a PET-confirmed complete metabolic response after standard immunochemotherapy and the results are awaited. 20 However, due to the unavailability of PET-CT and lack of data regarding prospective PET-guided studies, incorporating consolidation RT into routine practice is still common in clinical practice.
In our study, we focused on the variant effect of mediastinal RT in different age groups and demonstrated significant survival benefit from RT in PMBCL patients aged 40–59 years. Nevertheless, this benefit was not observed in young adults (18–39 years), possibly due to increased risks of cardiovascular risk and second primary malignancies, which is the metachronous malignancy developing 6 months or more after DLBCL based on Warren and Gates criteria. 21
Increased cardiovascular risk is considered to be correlated with higher doses of heart radiation. 22 Actually, the risk of coronary heart disease was increased 2.5-fold for patients with Hodgkin lymphoma receiving a mean heart dose of 20 Gy from mediastinal RT compared with patients not exposed to mediastinal radiation. The relationship of excess relative risk (ERR) and age period has been studied and there seemed to be a decreased trend in ERR with increasing treatment age. For patients aged <27.5, 27.5–36.4, and 36.5–50.9 years, ERR/Gy is 20.0%, 8.8%, and 4.2%, respectively. 23 For patients aged 40–59 years, hypertension and cardiac diseases such as atherosclerosis and valvular degeneration are more common than their younger counterparts, which could partially limit the use of anthracyclines and increase the significance of mediastinal RT. In contrast, young adult patients most often have a better performance status, better organ reserves, and usually more resilience to bear the full-intensity chemotherapy.
Additionally, unlike patients aged 40–59 years, young adults themselves may not pay attention to their symptoms, especially for those not fully aware of the late effects of prior treatment. Meanwhile, young adults are less likely to be considered to have heart disease in clinical daily routine. Thus, for those who survived decades after cancer treatment, diagnostic delays of cardiac dysfunction could be more common than their older counterparts, which could result in a less favorable outcome.
It is true that incidence rates of cardiac toxicity have decreased with advances and changes in modern radiation therapy techniques such as three-dimensional treatment planning and intensity-modulated radiotherapy. 24 However, these advanced techniques are only available with advanced equipment and experienced radio-oncologists, which limit the use of these modern radiation therapy techniques, and there is virtually no direct evidence regarding the decrease in cardiac toxicity with the use of these techniques in PMBCL.
Limitations of our study are specific to the population-based registry. First, some information regarding RT may be missed by SEER registries, especially for patients receiving RT outside of hospital settings. Second, the biases associated with unmeasured reasons for RT have been considered as limitations of SEER RT data. Finally, with the shifting treatment paradigm, thanks to PET-CT, mediastinal radiation is selectively used and the decision of radiation therapy may be related to perceived risk of relapse. Without available information on response to front-line systematic treatment and patient characteristics, data analysis could not be done under adequate control within such a study.
In regard to advances in RT techniques and technologies, the accuracy of delivery is improved and irradiation of healthy tissues is minimized. Thus, in this modern radiation era, prospective case–control cohort and randomized controlled clinical trials are expected to determine the role of RT in PMBCL.
Conclusions
Radiation therapy may offer survival benefit to PMBCL patients aged 40–59 years. However, in patients aged 18–39 years, this impact was not significant. Omission of radiation therapy in young adult patients may be considered, especially for those who attain complete metabolic remission on whole-body PET/CT after initial systemic treatment.
Footnotes
Acknowledgment
The authors acknowledge the efforts of the SEER program tumor registries in creation of the SEER database.
Author Disclosure Statement
No competing financial interests exist.