
Abstract
Introduction:
As the survival rate of childhood acute lymphoblastic leukemia (ALL) continues to improve, the physical deconditioning is becoming an increasingly common problem in survivors. The aim of this study was to compare the cardiorespiratory fitness and physical activity levels of survivors and control participants.
Methods:
A total of 221 childhood ALL survivors (114 males and 107 females), diagnosed between 1987 and 2010 and treated according to Dana Farber Cancer Institute-ALL 87-01 to 05-01 protocols at Sainte-Justine University Health Center (SJUHC), Montreal (Canada), and 825 control participants (364 males and 461 females), recruited in the Canadian Health Measures Survey (cycle 2) during 2009 to 2011 by Statistics Canada, were included in our analyses. In both survivors and controls, cardiorespiratory fitness and moderate to vigorous physical activity (MVPA) were assessed.
Results:
Survivors' V̇O2 peak was found to be 22% lower than that of controls. Cardiorespiratory fitness was different between the survivors (32.4 ± 8.3 mL/(kg·min); β = 0.11; 95% confidence interval [CI] 0.07–0.14) and the controls (41.6 ± 9.4 mL/(kg·min); β = 0.16; 95% CI 0.13–0.18), despite a clinically equivalent level of MVPA [survivors (27.5 ± 27.4 min/day) and controls (33.4 ± 24.2 min/day)]. Status (being survivor) and the age of the participants were negatively associated with cardiorespiratory fitness, whereas MVPA and male gender were positively associated with cardiorespiratory fitness.
Conclusion:
We observed that for a clinically equivalent level of MVPA, cardiorespiratory fitness was significantly lower in survivors compared with controls. Our findings showed that female survivors were most affected, compared with male survivors. These findings allow further understanding of the physiological differences between childhood ALL survivors and control participants and have important implications for this high-risk population of survivors.
Introduction
Childhood acute lymphoblastic leukemia (ALL) is the most common pediatric cancer. Over the past decades, the progress in treatments has considerably improved the survival rate of children with ALL. 1 However, patients' exposure to chemotherapeutic agents leads to multiple late adverse effects that occur several years after the end of the treatment. 2 Among these late adverse effects, cardiovascular diseases and physical deconditioning in survivors are common problems that seem to increase with age.3,4 Ensuring a good cardiorespiratory fitness is an essential component in the care of childhood ALL survivors, especially since above-normal exercise behavior has been shown to reduce the risk of mortality due to cancer. 5
It has been suggested that the decrease in cardiorespiratory fitness of childhood ALL survivors may be due to their cardiovascular response to chemotherapeutic agents.6,7 Indeed, the cardiotoxic effects of treatments (i.e., anthracycline) seem to induce structural and functional disorders to the myocardium. 8 Numerous studies have reported improvements in survivors' functional capacity, musculoskeletal system, immune system, inflammatory profile, and cardiovascular system following the regular practice of physical activity.9,10 However, nearly 53% of survivors do not meet the physical activity guidelines, with a greater proportion of females; even though physical activity is safe for their health. 11
The cardiorespiratory fitness of this population is directly impacted, as illustrated by a shorter exercise duration than the one predicted during a maximal cardiopulmonary exercise test. 12 A decrease of about 13% (≃6 mL/(kg·min)) of maximal oxygen uptake is observed among childhood ALL survivors in comparison to a healthy population. 13 This suggests that survivors should practice regular physical activity to maintain a normal functional capacity as recommended by the American Cancer Society.
In this study, we assessed the cardiorespiratory fitness and moderate to vigorous physical activity (MVPA) of ALL survivors in comparison to control participants. This was done to provide a better understanding of how these two parameters differ in both populations and to find out whether gender has an impact on their cardiorespiratory fitness.
Materials and Methods
Participants
Our study included 250 childhood ALL survivors, among whom 29 were excluded: 24 survivors did not complete the cardiopulmonary exercise test because there were issues with the equipment or data collection, and 5 participants received a different treatment than the Dana Farber Cancer Institute (DFCI)-ALL protocols. All 221 childhood ALL survivors (114 males and 107 females) were diagnosed between 1987 and 2010 and treated according to DFCI-ALL 87-01 to 05-01 protocols 14 at Sainte-Justine University Health Center (SJUHC), Montreal (Quebec), Canada. The survivors' age at cancer diagnosis was 6.4 ± 4.6 years. They were recruited in the context of the PETALE study, a multidisciplinary research project with the goal to identify and to comprehensively characterize associated predictive biomarkers of long-term treatment-related complications in childhood ALL survivors. 15 These survivors had no history of refractory or recurrent diseases and did not receive a hematopoietic stem cell transplant. They were almost exclusively of French Canadian descent (>95%). 15 In this study, we restricted survivors to those who were less than 19 years old at diagnosis. Subjects who had suffered from congenital bone disease or who received osteotoxic drugs for non-ALL diseases were excluded. Written informed consent was obtained from every patient or parent/legal guardian. The PETALE study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Review Committee of SJUHC.
All 825 Canadian control participants (364 males and 461 females) were recruited in the Canadian Health Measures Survey (cycle 2) during 2009 to 2011 by Statistics Canada. 16 Statistics Canada excluded all controls and their families who lived in reserves or in other Aboriginal settlements in the provinces, institutional residents, and full-time members of the Canadian Forces. Pregnant women were excluded as they were not eligible for the modified Canadian aerobic fitness test or for the physical activity assessment. Participants who scored negatively on the Physical Activity Readiness Questionnaire were also excluded. 17 In addition, we excluded participants who were not from the Caucasian Canadian population aged 10 to 43 living at home and residing in one of two provinces (i.e., Quebec or Ontario). Participants who have or had cancer were excluded. The protocol was approved by Health Canada's Research Ethics Board, and all control participants provided written informed consent.
Cardiopulmonary exercise test
Cardiopulmonary fitness was measured in both cohorts with an incremental cardiopulmonary exercise test. In survivors, maximum oxygen uptake (V̇O2 peak) [mL/(kg·min)] was measured by a McMaster incremental cycle protocol 18 on an electromagnetic cycle ergometer (ER900; Ergoline, Bitz, Germany) with a breath-by-breath system (Oxycon Pro; Viasys Healthcare, Germany) calibrated before each test. The test consisted of a standard incremental procedure at a pedaling cadence of 50–70 rpm starting at 25 W, increasing the load by 25 or 50 W (depending on the height and the gender of the survivor) every 2 minutes. At the end of the test, an active rest period at 25 W for 3 minutes was followed by a passive rest period of 3 minutes. All survivors were monitored continuously during the test with 12-lead electrocardiograms (CASE Exercise Testing; GE Marquette, Milwaukee, WI). Blood pressure was measured every 2 minutes (Tango M2; SunTech Medical, Morrisville, NC). The exercise physiologist ensured that the cardiopulmonary exercise test was not limited by symptoms. He determined whether the survivors reached two out of three of the following criteria to validate their V̇O2 peak: respiratory exchange ratio value >1.15, OMNI >7, and HRmax ≥85% of the predicted value. 19 In controls, aerobic capacity with a corresponding equation to predict the V̇O2 peak [mL/(kg·min)] was measured by the modified Canadian aerobic fitness test (mCAFT). 20 The mCAFT has been known to have a high degree of reliability and validity for predicting exercise capacity. 21 During the mCAFT, controls were required to complete one or more 3-minute “stepping” stages at predetermined speeds based on their gender and age. 22 Their heart rate was recorded at each stage. The test was completed when the heart rate of control participants had reached 85% of their age-predicted maximal heart rate. The predicted V̇O2 peak was calculated based on the last completed stage.21–23 Predicted values from the mCAFT were highly correlated to the objectively measured V̇O2 peak. 21 The pediatric-specific equation was used to calculate V̇O2 peak in children aged 10 to 15, 24 whereas the regular equation was used in control participants aged 16 to 43.21,23 Thus, cardiopulmonary fitness was measured in both cohorts with a maximal cardiopulmonary exercise test in survivors and with a sub-maximal cardiopulmonary exercise test in controls. These methods have been shown to be correlated in the general population as well as in pathological populations.25,26 Also, it has been reported that in a sub-maximal cardiopulmonary exercise test, the correlation coefficient between the V̇O2 peak measured and predicted is strong (r = 0.83).27,28 In this sense, there is strong evidence supporting the fact that the incremental cardiopulmonary exercise tests can be compared between the cohorts.
Physical activity assessment
Physical activity was assessed in both cohorts with a daily measure of moderate to vigorous leisure physical activities. In survivors, the Minnesota Leisure Time Physical Activity Questionnaire29,30 and the Tecumseh Self-Administered Occupational Physical Activity Questionnaire 31 were used to estimate their daily physical activities. An experienced exercise physiologist conducted the interviews. In accordance with the Canadian physical activity guidelines, 32 all survivors ≥18 years old had to cumulate a minimum of 150 min/week of moderate to vigorous leisure physical activities, whereas the survivors <18 years old had to achieve at least 60 min/day of moderate to vigorous leisure physical activities. In controls, MVPA was calculated in min/day when the activity was at an intensity higher than 3.0 metabolic equivalents, over a period of 10 minutes or more.32,33 Physical activity data were collected by using a waist-worn Actical accelerometer (Philips Respironics, OR) over their right hip on an elasticized belt during waking hours during 7 consecutive days. A valid day was defined as 10 or more hours of monitor wear time, and a valid respondent was defined as 4 or more valid days. 34 Wear time was determined by subtracting non-wear time from 24 hours and non-wear time was determined as at least 60 consecutive minutes of 0 counts, with allowance for 1 to 2 minutes of counts between 0 and 100. 34 Thus, physical activity was measured with a physical activity questionnaire in survivors and with an accelerometer in controls. The correlation between both methods is strong to compare the data and does not differ despite the age or sex of the participants. 35 Moreover, it has been shown that self-reported MVPAs measured from the Minnesota Leisure Time Physical Activity Questionnaire and the Tecumseh Self-Administered Occupational Physical Activity Questionnaire are strongly associated with accelerometer data.35–37 In this sense, there is strong evidence that shows that physical activity questionnaire and accelerometer data can be compared between both cohorts.
Statistical analysis
Descriptive statistics were used to report survivors' and control participants' characteristics. To compare survivors with their control counterparts, we performed a Chi-square test for binary variables and a Wilcoxon Rank-Sum test for continuous variables. Crude linear models were used to construct the regression lines reflecting crude associations between V̇O2 peak and MVPA, V̇O2 peak and age. To assess whether survivors were associated with a smaller V̇O2 peak value independently of the MVPA level, we performed multiple linear regression analyses with status (being survivor), MVPA, gender, and age as predictors. Analyses were performed by using SAS (version 9.4; SAS Institute, Inc., Cary, NC). A p-value <0.05 was considered significant. We used R (R Core Team, Vienna, Austria) for the graphical output.
Results
The characteristics of the 221 survivors and 825 control participants are presented in Table 1 (survivors' treatments are detailed in Supplementary Table S1). Descriptive statistics reported no significant differences between survivors and controls for the main anthropometric characteristics. There was no significant difference for the white blood cell count. Also, hemoglobin and platelet count were statistically, but not clinically, different between survivors and controls; values of blood parameters were within their normal range. 38 Analyses showed a significant difference of 9.2 mL/(kg·min) for V̇O2 peak between survivors [32.4 ± 8.3 mL/(kg·min)] and controls [41.6 ± 9.4 mL/(kg·min)]. According to the Wasserman 39 and Hansen 40 equations, V̇O2 peaks predicted in survivors and controls were 41.9 ± 9.1 and 41.4 ± 9.5 mL/(kg·min), respectively. A statistically significant difference was shown for the MVPA [survivors (27.5 ± 27.4 min/day) and controls (33.4 ± 24.2 min/day)]. However, this difference cannot be considered significant in a clinical context. Gender analyses (Table 2) showed similar results for V̇O2 peak and MVPA between survivors and controls. In males, a significant difference of 10.7 mL/(kg·min) between survivors and controls was observed for the V̇O2 peak; whereas in females, this difference was of 9.3 mL/(kg·min) between both cohorts.
Clinical Characteristics of Childhood Acute Lymphoblastic Leukemia Survivors and Controls
MVPA variable represents minutes per day of MVPAs. Continuous data are expressed as mean ± standard deviation.
We used the chi-square test for binary variables and Wilcoxon Rank-Sum test for continuous variables.
Twenty-seven missing data in control participants.
ALL, acute lymphoblastic leukemia; MVPA, moderate to vigorous physical activity; N, number of survivors; V̇O2 peak, maximal oxygen uptake.
Clinical Characteristics of Childhood Acute Lymphoblastic Leukemia Survivors and Controls According to Gender
MVPA variable represents minutes per day of MVPAs. Continuous data are expressed as mean ± standard deviation.
We used the chi-square test for binary variables and Wilcoxon Rank-Sum test for continuous variables.
Twenty-seven missing data (8 male controls and 19 female controls).
Crude associations between V̇O2 peak and the MVPA are presented by regression lines, estimated separately, in Figure 1. A significant positive crude association between MVPA and V̇O2 peak was observed in both cohorts (Fig. 1A). However, the V̇O2 peak was not the same between the survivors and controls, as can be seen in Figure 1A. We also observed that the MVPA values and V̇O2 peaks were higher in controls than in survivors. This difference in V̇O2 peak between controls and survivors was higher with MVPA. In male survivors, V̇O2 peak augmented more slowly (β = 0.06; 95% confidence interval [CI] 0.02–0.11), compared with controls (β = 0.11; 95% CI 0.08–0.14) (Fig. 1B). In females, the V̇O2 peak trend was similar between the survivors (β = 0.13; 95% CI 0.08–0.18) and controls (β = 0.12; 95% CI 0.09–0.15) (Fig. 1C). Crude associations between V̇O2 peak and age are presented by regression lines, estimated separately, in Figure 2. The V̇O2 peak was lower with the age of the participants in both cohorts, especially in survivors (β = −0.43; 95% CI −0.6 to −0.27) in comparison to controls (β = −0.28; 95% CI −0.34 to −0.23) (Fig. 2A). In males, the V̇O2 peak was lower in survivors compared with controls of the same age, but the decline in V̇O2 peak as a function of age was similar between the cohorts (survivors β = −0.38; 95% CI −0.58 to −0.17) and controls (β = −0.37; 95% CI −0.44 to −0.30) (Fig. 2B). In females, the V̇O2 peak was lower in survivors and the V̇O2 peak was lower with age among survivors (β = −0.51; 95% CI −0.68 to −0.34) than for controls (β = −0.17; 95% CI −0.23 to −0.11) (Fig. 2C).
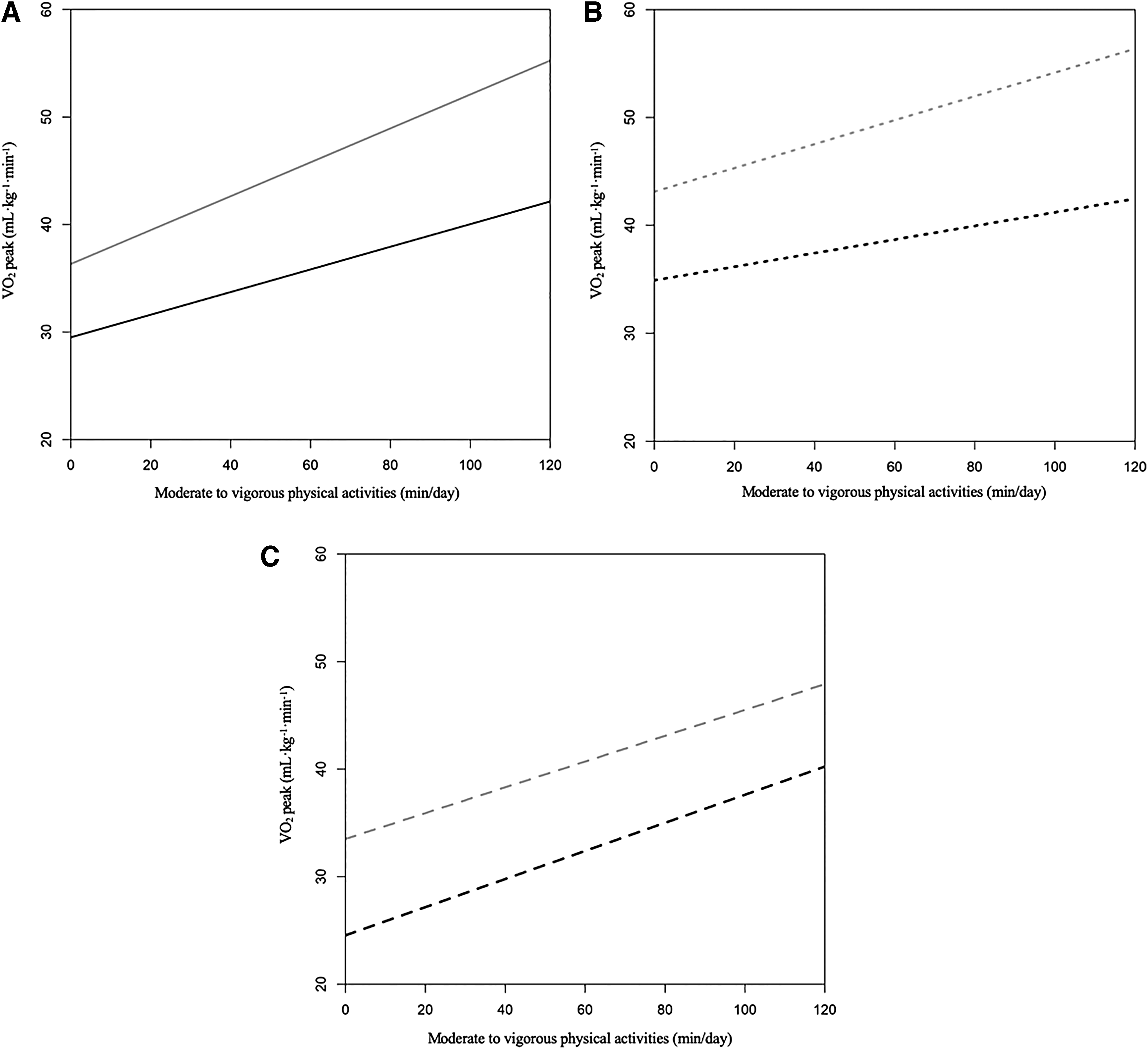
Relationship between V̇O2 peak and MVPAs (min/day) from childhood ALL survivors and controls.
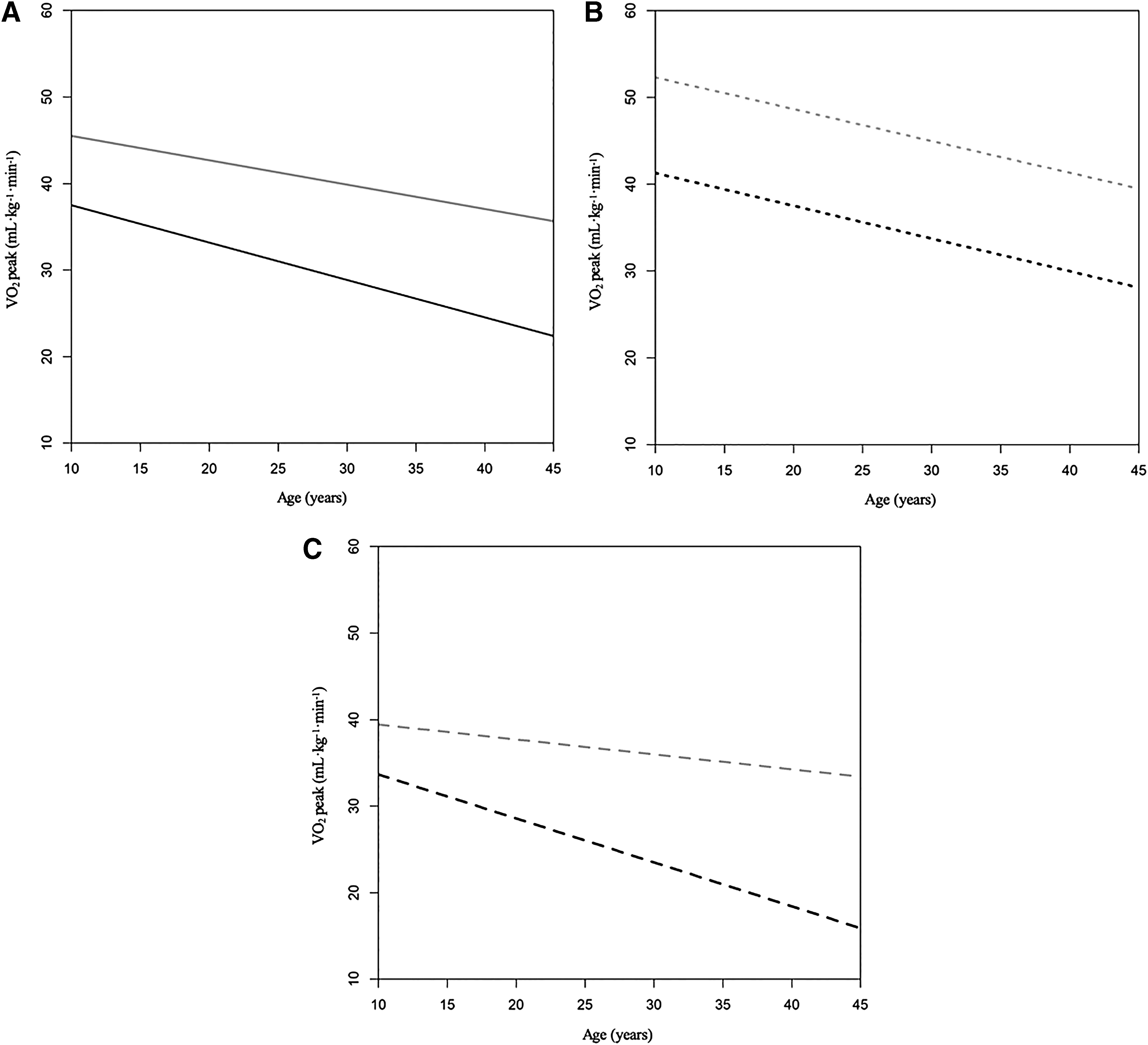
Relationship between V̇O2 peak and age (years) from childhood ALL survivors and controls.
Adjusted linear regression for V̇O2 peak
The results of the adjusted linear regression analyses are presented in Table 3. The status and age of the participants were negatively associated with a lower V̇O2 peak (β = −9.78; 95% CI −10.9 to −8.8 and β = −0.2; 95% CI −0.24 to −0.15, respectively). We also observed that the MVPA and gender (i.e., males) were positively associated with a higher V̇O2 peak (β = 0.07; 95% CI 0.06–0.09) and (β = 9.29; 95% CI 8.43–10.15), respectively.
Adjusted Linear Regression for V̇O2 Peak (N = 1,046)
Status represents the status of the participant (i.e., childhood ALL survivors).
Adjusted linear regression for status, MVPA, gender and age.
CI, confidence interval.
Discussion
We report that childhood ALL survivors had a substantially lower cardiorespiratory fitness level compared with controls. These findings were supported by a clinically equivalent level of MVPA in both cohorts, which was never observed earlier. As a matter of fact, we showed that survivors had a V̇O2 peak of 22% lower than controls and that female survivors were most affected, compared with male survivors. Moreover, in female survivors, age has been shown to accelerate the process of cardiorespiratory fitness decline. Our finding confirms and add new insights to these previously published reports.41–44
Cardiorespiratory fitness and physical activity were previously reported as being lower among survivors than in healthy subjects.12,41,42,45–47 One of the first studies that looked at cardiorespiratory fitness reported a reduced exercise capacity of 33% in childhood ALL survivors. 12 A proportion of 30% to 50% of survivors had a cardiorespiratory condition lower than normal, 48 and 14% of survivors had a lower cardiorespiratory fitness than healthy subjects. 41 These differences seem to be accentuated according to the participant status (being survivors). Indeed, the survivors' cardiorespiratory fitness was much lower when compared with trained subjects than untrained subjects. 42 Our findings regarding childhood ALL survivors are supported by a systematic review that revealed a decrease of ∼13% in cardiorespiratory fitness among survivors compared with healthy subjects. 13 This could be explained by differences between survivors and healthy subjects since it has been reported that survivors' cardiorespiratory fitness decreases with the cumulative dose of anthracycline received during treatment. 43 We observed a difference of 13% in cardiorespiratory fitness between male and female survivors. In this regard, it has been reported that female survivors are especially at risk for developing a low cardiorespiratory fitness. 41 Some of these studies suggest that the V̇O2 peak reduction would be more marked in female survivors than in males.44,49 The lack of regular physical activity is one of the most common reasons cited in the literature, which may explain a low cardiorespiratory fitness in female survivors. 11
Very few childhood ALL survivors meet the physical activity guidelines. According to the American Association for Cancer Research, almost 44% of survivors are less likely to respect the physical activity recommendations and more than 74% are less likely to be physically active, compared with the general population. 11 These observations suggest that the non-compliance with recommendations and physical inactivity are responsible for the low cardiorespiratory fitness of the survivors. This is supported by the fact that during cancer treatments, physical activity is reduced in patients.45–47,50 This trend seems to persist among survivors. 41 Overprotection from the parents after the treatments could explain the lower compliance of survivors regarding physical activity guidelines. 51 This may have an impact on children's motivation and engagement to spontaneously practice physical activity, whereas parental support for health guidelines were recognized to be significant predictors of children meeting physical activity guidelines. 52 However, our results demonstrated that there is at least one other explanatory parameter. We observed that for a clinically equivalent level of MVPA, the cardiorespiratory fitness was significantly lower in survivors than in controls. Also, the V̇O2 peak trend as a function of MVPA was not consistent across male and female survivors. Our analyses showed that for females, the improvement of V̇O2 peak relatively to MVPA was similar in both cohorts. For males, this improvement was lower in survivors than in controls. However, for both genders, this trend was inferior in survivors. These results suggest that for a clinically equivalent level of MVPA, female survivors had a better ability to enhance their cardiorespiratory fitness than males. Contrary to the cardiorespiratory fitness level, which is influenced by anthracycline-based cancer treatments, the regular practice of physical activity in survivors is not influenced by anthracycline treatments 11 or the prognostic risk. 53 However, our analyses showed that the age of participants was negatively associated with a lower V̇O2 peak. The decline of V̇O2 peak as a function of age is a known aspect of cardiorespiratory fitness, at least in healthy subjects. 54 Here, we showed that it is also the case in childhood ALL survivors. Nevertheless, our analyses described disparities between the male and female survivors. In males, the decline in cardiorespiratory fitness was similar between both cohorts, but in females, this was faster in survivors. In female survivors, age seemed to be an important factor regarding the difference in cardiorespiratory fitness. This adds new insights on the aggregate role of age in cardiorespiratory fitness decline in childhood ALL survivors.
The clinical implications of this study are important because cardiorespiratory fitness impairment may be explained by many underlying factors. In childhood ALL survivors, a lower cardiorespiratory fitness may be due to their cardiovascular response to the chemotherapeutic agents. 6 We revealed that the participants who had received anthracycline-based cancer treatments were negatively associated with V̇O2 peak. The cardiovascular response is more limited in survivors when considering anthracycline treatments and the related cardiotoxic effects. This is due to subclinical cardiac dysfunctions, 55 such as structural and functional impairments of the myocardium,6,48 reduction of myocardial contractility, 12 systolic and diastolic dysfunction43,48 and left ventricular dysfunction. 56 A previous study has reported that the left ventricular diastolic function was associated with the exercise capacity of survivors. 43 Also, it has been observed in survivors that anthracycline treatments resulted in an impairment of muscle oxygen extraction during exercise in comparison to healthy subjects with a similar V̇O2 peak. 57 Further, one paper showed that anthracycline treatments impair the pulmonary function by inducing a significant reduction in the diffusing capacity of the lungs for carbon monoxide (DLCO) in childhood leukemia survivors. 58 In other words, the cardiopulmonary response of survivors could explain the cardiorespiratory fitness impairment that we observed in our study. Taken together, these studies could explain, in part, why the cardiorespiratory fitness of survivors was significantly lower than of controls with a clinically equivalent level of MVPA.
However, the contribution of genetic predispositions to a low cardiorespiratory fitness level should not be dismissed. Indeed, it has been reported that survivors may increase their cardiorespiratory fitness through regular physical activity. 59 On the contrary, there remains a great inter-individual variability in subjects' capacity to improve their cardiorespiratory fitness in response to regular physical activity. 60 Studies have reported a high heterogeneity degree in the ability of subjects to improve their cardiorespiratory fitness.61,62 Different associations between genetic variants and cardiorespiratory fitness in response to regular physical activity have been previously shown. 63 This is the reason that the association between genetic variants and cardiorespiratory fitness should be considered, especially because anthracycline-based cancer treatments can modify gene expression. 64
It should be noted that our methodology has certain limitations that are necessary to discuss. We decided to analyze only the MVPA data, without taking into consideration the low-intensity activities data. This was to maintain the validity of our data because our assessment tools (i.e., physical activity questionnaires and accelerometers) had limitations that did not enable analyses of low-intensity exercises. 65 Indeed, physical activity questionnaires may overestimate or underestimate the physical activity of participants, especially for low-intensity activities. 66 As for accelerometers, they do not measure all the body movements, which can underestimate low-intensity activities. 66 The use of these two different assessment tools could also have been a limitation to our study. Indeed, the use of a questionnaire to obtain a self-reported level of physical activity can be considered a subjective measure, whereas the use of an accelerometer can be considered an objective measure of physical activity level. However, as reported by Sabia et al., 35 the use of accelerometers were initially used in epidemiological research to validate physical activity questionnaires. No consensus on the best methods to validate physical activity levels has been reached in the past few years, allowing both methods to maintain their legitimacy in measuring physical activity. Moreover, they are considered the gold standard for measuring levels of physical activity in the general population and it has been reported that the correlation between both methods is strong to compare the data.36,37,67 The precision of the statements in physical activity questionnaires can be improved by expert administration, as was performed in our study. In the same order of ideas, tests used to measure cardiopulmonary fitness in both cohorts were different. Indeed, we used a sub-maximal test in controls and a maximal test in survivors. It would have been possible to evaluate the cardiorespiratory fitness with aerobic field tests.68–70 However, it has been reported that outcomes during cardiopulmonary exercise tests in survivors may be limited by their symptoms. 71 For this reason, the survivors performed a cardiopulmonary exercise test to ensure that they had reached their V̇O2 peak, confirmed by clinical recommendations, 19 and that their outcomes were not limited by potential overprotection72,73 or musculoskeletal issues,74,75 as previously reported. The exclusion of these biases, which can limit the survivors' V̇O2 peak, is the strength of this study, which is mainly concerned with the valid physiological measurement of its participants.
In conclusion, this study showed that for a clinically equivalent level of MVPA, cardiorespiratory fitness was significantly lower in survivors. Our findings showed that female survivors were most affected, compared with male survivors. These findings increase our knowledge regarding the physiological differences between childhood ALL survivors and controls and have an important implication for the high-risk population of survivors.
Footnotes
Acknowledgments
This work was supported by the Institute of Cancer Research (ICR) of the Canadian Institutes of Health Research (CIHR), in collaboration with C17 Council, Canadian Cancer Society (CCS), Cancer Research Society (CRS), Garron Family Cancer Center at the Hospital for Sick Children, Ontario Institute for Cancer Research (OICR), and Pediatric Oncology Group of Ontario (POGO) (grant number: TCF 118694). This research was also supported in part by PhD study grants from Cole Foundation, Fonds de Recherche du Québec–Santé (FRQS), Sainte-Justine University Hospital Center Foundation, and Foundation of Stars. The analysis presented in this article was conducted at the Quebec Interuniversity Center for Social Statistics (QICSS), which is part of the Canadian Research Data Center Network (CRDCN). The services and activities provided by the QICSS are made possible by the financial or in-kind support of the Social Sciences and Humanities Research Council (SSHRC), the Canadian Institutes of Health Research (CIHR), the Canada Foundation for Innovation (CFI), Statistics Canada, the Fonds de recherche du Québec–Société et culture (FRQSC), the Fonds de recherche du Québec–Santé (FRQS), and the Quebec universities. The views expressed in this article are those of the authors, and not necessarily those of the CRDCN or its partners. The authors appreciate the assistance of Ariane Levesque (McGill University) for her review of the article in the English language.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.