
Abstract

Adolescent and young adult (AYA) cancer is a broad term and its use in the existing literature is varied. Most commonly, and for the purpose of this article, the term describes any cancer diagnosis received in adolescence or young adulthood*. AYA cancer patients present with unique needs; receiving a cancer diagnosis can disrupt normative development and slow down achievement of crucial milestones for young people. 1 Thus far, AYA patients' unique needs have not been adequately addressed. 2 Resultantly, AYA psycho-oncology is gaining momentum; cancer charities and communities globally are organizing campaigns to raise funds for AYA cancer research, telling inspiring stories of AYA cancer survivorship, and offering support to families and patients impacted by AYA cancer. Such efforts are likely invaluable to anyone involved; the parents may feel better supported, young people may not feel alone in their battle, and researchers may aspire to make a breakthrough with new discoveries.
Compared with childhood cancer, which in most cases exceed 80% 5-year survival rate, 3 the prospects for AYA cancer are yet to reach a similar threshold of success. Only 8 out of 20 common cancer types in AYA patients show evidence for statistically significant improvement in survival rates since 1985 and, as of 2000–2007, a third of most common cancers among AYAs showed a 5-year survival rate <60%. 4 Nevertheless, the number of survivors of AYA cancer is growing, and the research focus has shifted from survival efforts to late effects of cancer.5,6 Among these, psychosocial functioning of young survivors has been recognized as one of the main research priorities. 7
A lot of work in developmental psycho-oncology has already been done, for example, from qualitative studies describing the nature of romantic relationships in young survivors 8 to attempts at quantifying psychological functioning during various phases of cancer treatment. 9
Yet, the results of these studies are often conflicting and seldom treat AYAs as a separate group from childhood cancer. They report a wide range of possible outcomes for young cancer patients: from a subset of survivors experiencing significant psychological distress10,11 to others who report psychosocial growth.12–14 Although limitations and methodological issues form a part of every discussion section of academic articles, there remain areas that pose barriers to progress and that need to be addressed in future research within AYA psychosocial oncology.
The Age Confusion
One such limitation is the large variety of age ranges, and related terminology employed by different studies. “Pediatric,” “childhood,” “adolescent,” “AYA,” and “adolescent and early young adult” (AeYA) are all terms used to describe young cancer patients (Fig. 1). However, they often describe different groups. The terms “childhood” and “pediatric” cancer are very broad and, according to the National Cancer Institute and Surveillance, Epidemiology, and End Results (SEER) program, include any cancer diagnosis that occurs between birth and 19 years of age. 3 In the United Kingdom, most people between 13 and 24 years will receive local AYA services. 15 Again, in the United States, the definition of AYA seems to be broader yet, including all patients who are between 15 and 39 years of age. To add on to this confusion, some studies started utilizing a smaller age range, describing participants between 13 and 21 years as AeYA (e.g., Johnson et al.). 16 Although most researchers justify their choice of age, these differences make it hard to compare the findings between studies.
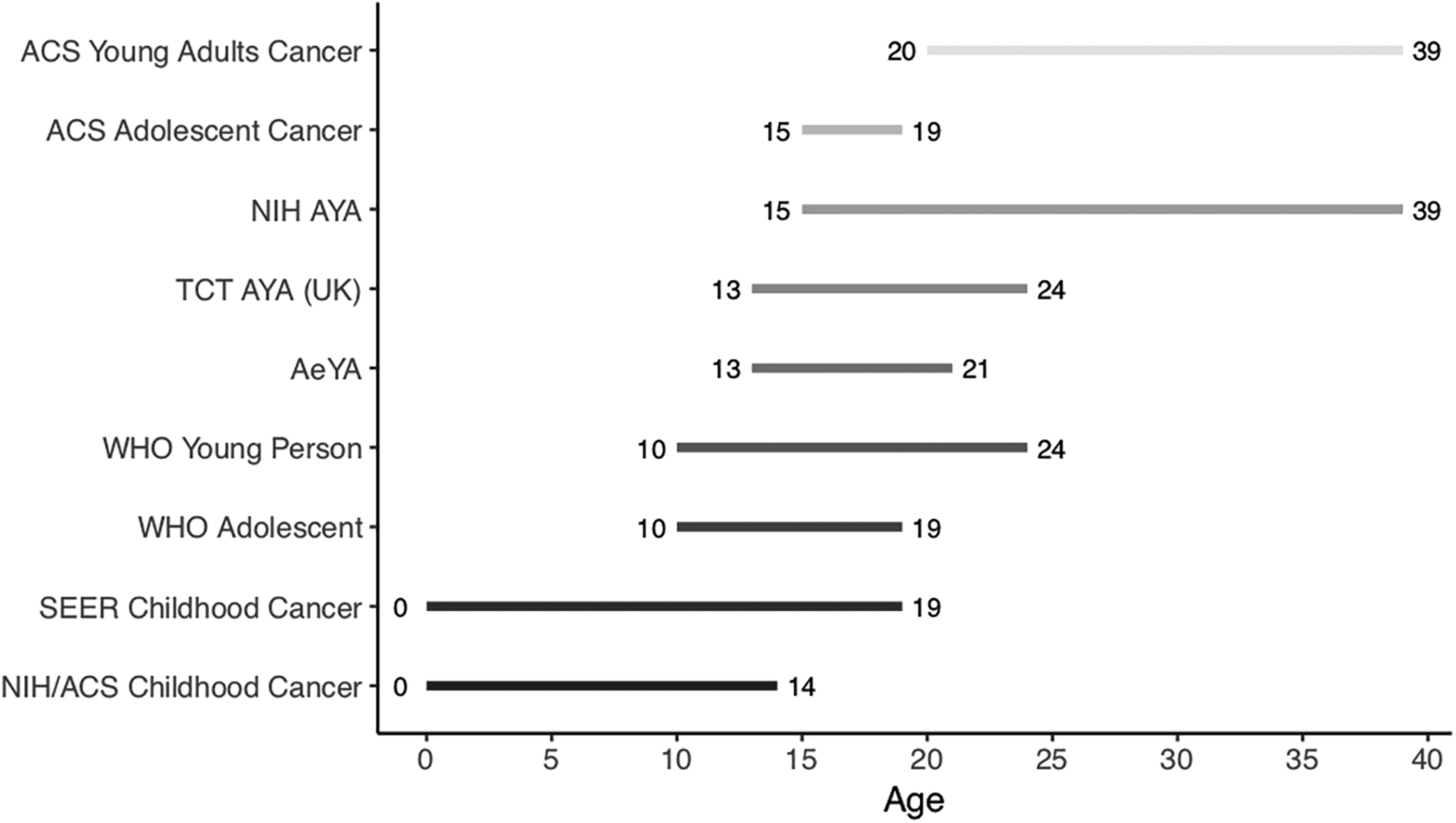
Overlap in definitions of childhood, adolescent, and young adult cancer. ACS, American Cancer Society; AeYA, adolescent and early young adult; AYA, adolescent and young adult; NIH, National Institute of Health; SEER, Surveillance, Epidemiology, and End Results; TCT, Teenage Cancer Trust; UK, United Kingdom; WHO, World Health Organization.
As the age range is not always clearly delineated, adolescents often end up being grouped with younger children or “young” adults. And early young adults may be grouped with older young adults. In both cases, the important factors of psychological adaptation might be overlooked. When studying psychological outcomes of cancer, we ought to consider distinct developmental periods and differences between children, adolescents, and young adults. Although the youngest of the former might still depend on their parents, the oldest of the latter could already be living fully independent lives. Moreover, maturity levels and cognitive ability may contribute to understanding of the illness, and hence, impact one's psychological well-being.
Age differences between samples can make it hard to evaluate best-suited intervention strategies and limit generalizability of findings. While employing a broad age range is acceptable, researchers should strive to clearly outline their reasoning for inclusion, and, whenever possible, conduct separate analyses to test for any age effects on the outcome of interest.
Cancer as a Single Illness
Another limitation is that most often the research treats childhood and AYA cancer diagnoses as a single illness. Although brain tumors are in some cases treated separately (e.g., Carpentieri et al.), 17 other tumors are seldom subcategorized. Cancer etiology will not only vary between different types but might also be significantly different between younger children, adolescents, and young adults (Table 1). 18 As such, different types of cancer may require different treatment modalities and, in turn, result in differential psychological outcomes, needs, and illness late effects.
The Most Common Types of Cancer in a Specific Age Range
Percentages in the brackets account for the prevalence of a given cancer (among all cancers diagnosed) within a particular age group. Data obtained from Surveillance, Epidemiology, and End Results (SEER) (Accessed March 22, 2019 at https://seer.cancer.gov).
Hodgkin's and non-Hodgkin's combined.
CNS, central nervous system.
Cancer is a highly heterogeneous illness. Ideally, AYA patients with the same type of diagnosis would be grouped together in analyses; however, if not feasible, researchers should aim to control and evaluate the extent of different treatments or diagnoses contributing to psychosocial outcomes.
Measures for Psychological Distress and Representativeness
Third, when assessing psychological states and mental health in patients with AYA cancer, we have to develop a better understanding of what a “normal” trajectory is. Although new measures (e.g., for cancer-related worry 19 ) are being developed and used in research, most commonly measures in psychosocial oncology research for assessing psychological constructs are not adapted to AYA cancer experiences. For example, a mood questionnaire might misinterpret one's fatigue as a depressive symptom instead of a side effect of treatment. We should, therefore, be cautious when using such measures so that we do not mistakenly label one's efforts to accept their illness as pathological just because they might deviate from the norm.
In addition, some studies reporting on post-traumatic stress disorder (PTSD) symptomatology make an a priori assumption that cancer was the most traumatic event in one's life, which is not always the case in young cancer survivors; for example, one study found that less than a third of respondents who do report trauma report a cancer-related event as traumatic. 20 So, are those PTSD rates informative of how cancer survivors may cope? Further yet, some studies aiming to assess PTSD reporting participation rates as low as 45% also mentioned that majority of nonrespondents did not participate in research because they wanted to avoid revisiting their illness. 21 In wanting to study psychosocial and mental health outcomes of young survivors, are we really accounting for those most in need of support?
When designing future studies in AYA psycho-oncology, researchers should carefully select measures for psychosocial outcomes and, whenever possible, try to adapt and validate them for a more accurate account of psychosocial outcomes in AYA cancer patients.
Childhood and AYA cancers remain relatively rare compared with incidence in older adults. 3 Therefore, recruiting participants is difficult, requires extensive efforts, and study samples are resultantly often small. 22 Despite employing the widest acceptable age range, as well as grouping all cancers together, one might still end up with a statistically underpowered sample. At best, a study with a large sample is cross-sectional in nature, thus preventing us from making any causal inferences, and making observations across time span.
Nevertheless, the findings thus far give us important insights, and although we are yet to understand why some young people who lived with cancer develop psychosocial difficulties, while others thrive, the first steps have been made. Great collaborative efforts, such as the establishment of the International Childhood Cancer Consortium (I4C), 23 are helping us to overcome some of the current shortcomings. By combining the wealth of data from large longitudinal cohorts, we will not only learn about the causes of childhood and AYA cancer but could also begin to uncover the risk and protective pathways in psychosocial adaptation. Large population-based studies such as Norwegian Mother and Child Cohort Study (MoBA) 24 contain rich information on disease and mental health variables at the individual and family level, repeated over time. Reliance on such large data sets will provide great quantitative insights into how resilience and psychopathology develop in young cancer patients over an extended period of time. These are important steps for a holistic approach to care in AYA oncology.
Addressing the unique needs in AYA cancer populations is crucial for the continued progress and reduction of inequalities of psychosocial outcomes in this vulnerable group of patients. Future research should aim to address the above-described methodological issues and continue employing creative solutions, which will strengthen current theoretical models, render research less burdensome on young patients and their families, and make it more accessible to investigators. Researchers should aim to separate their analyses for younger and older participants, encourage participation in research in clinical settings, consider the impact of different types of treatments and diagnoses, and subsequently aim to adapted and patient-reported outcome measures for AYA cancer patients. Such novel initiatives will continue to inspire international collaboration and invite private companies, policy makers, health care professionals, researchers, and support groups to work in tandem.
Footnotes
Acknowledgments
The author acknowledges the support and helpful comments from Prof. Lucy Bowes and Dr. Lauren Heathcote, and thanks Milan Wiedemann for help with the figure.
Author Disclosure Statement
No competing financial interests exist.