
Abstract
Purpose:
Adolescents and young adults (AYAs) with cancer are a vulnerable population with decreased attendance at National Cancer Institute (NCI) comprehensive cancer centers and Children's Oncology Group (COG) facilities. Decreased attendance at NCI/COG facilities has been associated with poor cancer outcomes. The objective of this study was to evaluate cancer care patterns of AYAs compared with children, within Pennsylvania, and factors associated with attending an NCI/COG facility.
Methods:
Data from the Pennsylvania Cancer Registry between 2010 and 2015 for patients aged 0–39 years at cancer diagnosis were used. Primary analyses focused on age at diagnosis, insurance status, race, ethnicity, gender, cancer type, stage, diagnosis year, and distance to the NCI/COG facility. The primary outcome was receipt of care at an NCI/COG facility. Odds ratios (ORs) were calculated using multivariable logistic regression models. Sensitivity analyses were conducted to test and estimate robustness.
Results:
A sample of 15,002 patients, ages 0–39, was obtained, including 8857 patients (59%) who attended an NCI/COG facility. Patients were significantly less likely to attend an NCI/COG facility if they were aged 31–39 years (OR 0.054, 95% confidence interval [CI] 0.04–0.07), non-White (OR 0.890, 95% CI 0.80–0.99), Hispanic (OR 0.701, 95% CI 0.59–0.83), female (OR 0.915, 95% CI 0.84–1.00), had Medicaid insurance (OR 0.836, 95% CI 0.75–0.93), and lived further from an NCI/COG facility. Sensitivity analyses largely corroborated the performed estimates.
Conclusions:
AYAs with cancer in Pennsylvania have disproportionate attendance at specialized NCI/COG facilities across a variety of demographic domains. Enhancing the attendance of AYAs with cancer at these specialized centers is crucial to improve cancer outcomes.
Introduction
Adolescents and young adults (AYAs) with cancer, defined as patients diagnosed with cancer between 15 and 39 years of age, are a historically disenfranchised subpopulation of the cancer community with decreased survival improvements compared with pediatric and adult counterparts; recent literature is controversial if survival improvement has changed in recent years.1–3 Epidemiologic studies have sought to understand factors accounting for this survival improvement disparity, known as the AYA gap. 4 Factors such as insurance status and race have been associated with significant survival disparities in this patient population.5,6 Decreased attendance at National Cancer Institute (NCI)-designated comprehensive cancer centers and facilities operating Children's Oncology Group (COG) clinical trials has been cited as another reason for differences in outcomes in AYAs with cancer.7–10 The benefits of such specialized centers include clinical trial access, specialized psychosocial support services, and other medical and supportive care approaches, which are critical to comprehensive care of AYAs with cancer.11–14 Yet, AYAs have consistently had decreased access to such specialized centers.15,16 Additional factors associated with decreased access include geographic distance, underinsurance, Hispanic ethnicity, and advanced disease stage. 17
As per recent census data, Pennsylvania is the fifth most populous state in the United States. 18 Yet, it has the third highest rate of new cancer cases in the United States. 19 A significant proportion (about 25%) live in rural counties. 20 The majority of NCI or COG centers are clustered in metropolitan areas, yet the highest rates of new cancer cases and cancer deaths occur mainly in rural state counties. 19
The objective of this study was to evaluate cancer care patterns of AYAs compared with children, within Pennsylvania, and to understand patient demographic and clinical factors associated with receiving care at NCI/COG facilities. Understanding patterns of oncologic care attendance can inform strategies to improve the infrastructure for access to NCI/COG centers, as well as where and how to target efforts for patient recruitment, and ultimately improve outcomes and survival of children and AYAs with cancer.
Materials and Methods
Study design and data source
The study design was a population-based retrospective analysis of 2010–2015 incidence data from the Pennsylvania Cancer Registry (PCR). Data included incident cancer cases diagnosed among Pennsylvania residents between 2010 and 2015. In addition, the PCR excludes cases due to interstate data exchange, the Health Insurance Portability and Accountability Act, or Veterans Affairs records, which represent <3% of cases. Data were provided by the Bureau of Health Statistics and Registries, Pennsylvania Department of Health, Harrisburg, Pennsylvania.
Participants
Analysis was restricted to persons 0–39 years of age at time of cancer diagnosis and excluded ∼1% with Medicare insurance, likely due to disability. Patients younger than 15 years of age at diagnosis were included in the analyses to serve as a control population for comparison with AYA patients. Those diagnosed by autopsy or death certificate were excluded, as were those missing residential longitude and latitude data at the time of diagnosis (<0.1% of cases). To ensure analyses included only individuals receiving cancer care, the sample was restricted to analytic cases with invasive cancers who received care in Pennsylvania. The sample was restricted to the 78% of individuals living within 60 minutes of an NCI/COG facility at the time of diagnosis to examine associations for patients for whom an NCI/COG facility was most likely in their choice set.
Outcome
The primary outcome of interest was receipt of care at an NCI/COG facility or a non-NCI/COG facility, similar to previous studies.7,17 We identified facilities based on the NCI website of designated, comprehensive cancer centers and the COG website of facilities, and note that some facilities are both NCI and COG facilities.21,22 One challenge was that each facility only listed the primary hospital address, yet many hospitals were part of larger hospital systems, so we included many of the affiliated locations as patients seen at the affiliated location could have access to the benefits of the NCI/COG facility (Supplementary Table S1).
Covariates
We examined the association of demographic and clinical variables with receipt of care at an NCI/COG facility. These variables included age at diagnosis (0–14, 15–18, 19–21, 22–30, and 31–39 years), insurance type (uninsured, Medicaid, private insurance, and other insurance), race (White, non-White, and race missing), ethnicity (Hispanic, non-Hispanic, and ethnicity missing), gender, primary cancer diagnostic group, stage and year at diagnosis, and distance to the nearest NCI/COG facility (<20, 20–39, and 40–60 minutes). We chose age categories similar to prior AYA cancer epidemiology studies.7,17 Additionally, as different facilities choose different AYA age ranges to focus on care, we wanted to account for this in our choice of age categories to evaluate if there are differential outcomes based on age category in attendance at NCI/COG facilities. We chose distance categories similar to other cancer epidemiology studies based on established patterns of how patients with cancer seek care. 23
The AYA National Institutes of Health cancer classification scheme proposed by Barr et al. was used to classify the cancer diagnostic group. 24
Statistical analyses
In baseline analyses, we allowed for the possibility that patients could be treated at more than one facility. To account for possible multiple observations of patients, standard errors were clustered at the patient level. We estimated the odds of receipt of care at an NCI/COG facility from logistic regression models, including all covariates in the unadjusted models (listed above), and reported adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for each covariate. In sensitivity analyses, the sample was restricted to patients who visited a single facility. A broader definition of additional affiliated locations was also included (Supplementary Table S2). Statistical analyses were performed with Stata 14 (StataCorp LP, College Station, TX). Travel time was calculated using the Stata command, osrmtime, which uses the Open Source Routing Machine and OpenStreetMap data to calculate the shortest travel time between two points (in this case, a patient's residential longitude/latitude data at the time of diagnosis and similar coordinates for each hospital).25,26 p-Values were calculated, with a two-sided p-value <0.05 considered statistically significant.
Human patient protection
This study was approved by the Institutional Review Board of the Penn State College of Medicine.
Results
Overall, 15,002 patients were identified, including 8857 (59%) who attended an NCI/COG facility and 6145 who did not. Compared with patients who did not attend an NCI/COG facility, a larger proportion of patients who attended an NCI/COG facility were younger, insured, non-White, non-Hispanic, male, with distant stage disease, and living within 20 minutes of an NCI/COG facility (Table 1). Table 2 shows unadjusted proportions of NCI/COG attendance for each covariate. The highest proportions of attendance occurred for the youngest group; 95.2% of patients aged 0–14 years attended an NCI/COG facility. This proportion significantly dropped with increasing age, with only 51.4% of patients 31–39 years of age attending an NCI/COG facility. Significantly lower NCI/COG attendance was found among uninsured patients compared with those with private insurance. Non-White patients had a significantly higher proportion of attendance at NCI/COG facilities compared with White patients, while Hispanic patients had a significantly lower proportion of attendance at NCI/COG facilities compared with non-Hispanic patients. Increasing proportions of NCI/COG attendance were seen with progressive disease stage, which was statistically significant for those with distant stage disease. A geographic distance gradient was seen, with statistically significant decreased attendance for patients living farther from an NCI/COG facility.
Sample Characteristics Overall and by Attendance at a National Cancer Institute or Children's Oncology Group facility
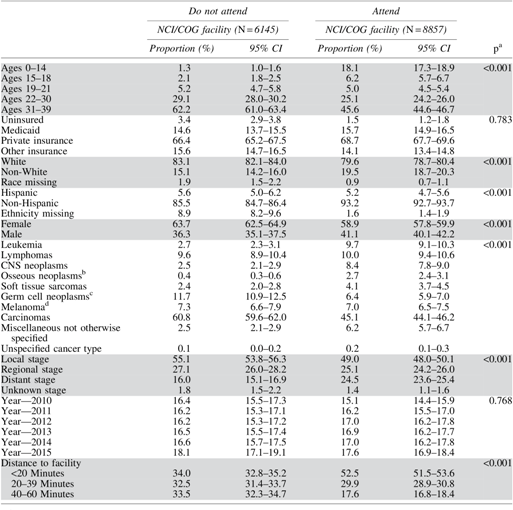
p-Value uses the Wilcoxon rank-sum test to test differences in characteristics by attendance at an NCI/COG facility.
Includes osseous and chondromatous neoplasms, Ewing tumor, and other bone neoplasms.
Includes trophoblastic neoplasms.
Includes skin carcinomas.
CI, confidence interval; CNS, central nervous system; COG, Children's Oncology Group; NCI, National Cancer Institute.
Unadjusted Proportions of Attending a National Cancer Institute/Children's Oncology Group Facility by Covariate
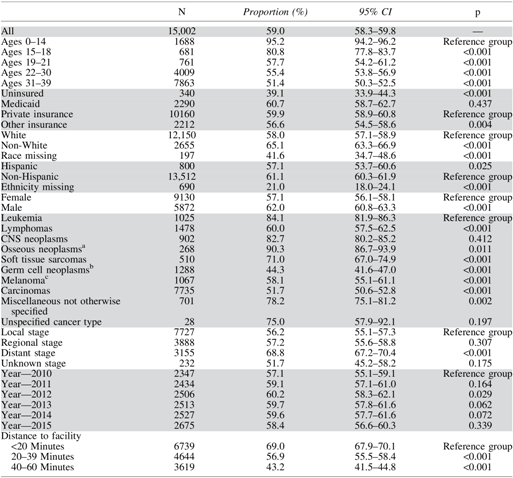
Includes osseous and chondromatous neoplasms, Ewing tumor, and other bone neoplasms.
Includes trophoblastic neoplasms.
Includes skin carcinomas.
In the adjusted estimates, there was a significant trend of decreased likelihood of attending an NCI/COG facility associated with increasing age at diagnosis (Table 3). Compared with younger pediatric patients, AYAs were significantly less likely to attend an NCI/COG facility (adjusted OR 0.224, 95% CI 0.16–0.31, for ages 15–18; adjusted OR 0.069, 95% CI 0.05–0.09, for ages 19–21; adjusted OR 0.061, 95% CI 0.05–0.08, for ages 22–30; and adjusted OR 0.054, 95% CI 0.04–0.07, for ages 31–39). Relative to patients with private insurance, uninsured patients (adjusted OR 0.420, 95% CI 0.33–0.53) were significantly less likely to attend an NCI/COG facility, and patients with Medicaid insurance (adjusted OR 0.836, 95% CI 0.75–0.93) were significantly less likely to attend an NCI/COG facility. Additionally, non-White (adjusted OR 0.890, 95% CI 0.80–0.99) and Hispanic patients (adjusted OR 0.701, 95% CI 0.59–0.83) were significantly less likely to attend an NCI/COG facility compared with White and non-Hispanic patients, respectively. Female patients were significantly less likely to attend an NCI/COG facility compared with males (adjusted OR 0.915, 95% CI 0.84–1.00). More advanced disease stage was modestly associated with greater attendance at NCI/COG facilities. Finally, patients living further from NCI/COG facilities were significantly less likely to attend such a facility—an adjusted OR of 0.542 (95% CI 0.50–0.59) for patients living 20–39 minutes from the nearest NCI/COG facility and 0.287 (95% CI 0.26–0.32) for patients living 40–60 minutes away, relative to patients living within 20 minutes. The proportion of those patients who attended an NCI/COG facility decreased to a greater degree with older age at diagnosis, with patients who were older at the time of diagnosis having decreased NCI/COG facility attendance compared with patients who were younger for the same distance range (Fig. 1).
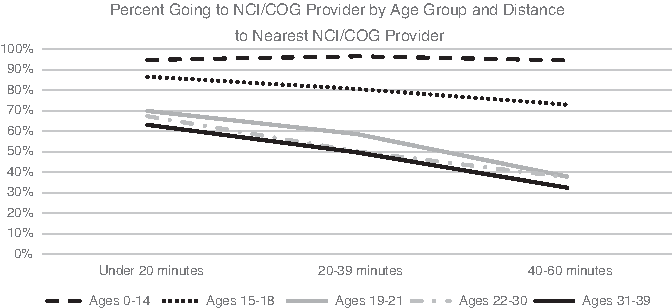
Proportion of patients attending an NCI/COG facility by age group and distance. COG, Children's Oncology Group; NCI, National Cancer Institute.
Multivariate-Adjusted Estimated Odds Ratio for Attending a National Cancer Institute/Children's Oncology Group Facility

p < 0.001.
p < 0.01.
p < 0.05.
Includes osseous and chondromatous neoplasms, Ewing tumor, and other bone neoplasms.
Includes trophoblastic neoplasms.
Includes skin carcinomas.
OR, odds ratio.
Sensitivity analyses were performed to test the robustness of estimates (Supplementary Table S2). The sample was restricted to the 78.9% of patients who attended a single facility. All estimates had the same sign and significance level, with the exception of the diagnosis stage variable. The modest decline in the OR magnitude led to estimates for regional stage at diagnosis being no longer associated with a significantly increased likelihood of attending an NCI/COG facility. The second set of robustness checks used a less restrictive definition of NCI/COG facility and added several University of Pittsburgh Medical Center (UPMC) sites outside of Pittsburgh and the Lehigh Valley Muhlenberg site as an additional COG site. Again, a minimal effect on estimates was found. The third set of robustness checks included a model where both Thomas Jefferson University and Temple University hospitals were excluded as NCI facilities as Thomas Jefferson University is NCI designated, but not an NCI-designated comprehensive cancer center, and Temple University is not categorized as an NCI center, but is affiliated with the Fox Chase Cancer Center (an NCI-designated comprehensive cancer center). Again, little qualitative change to results was found. Last, we excluded patients <1 year of age. Again, there is little effect on our results when we exclude these 187 patients.
Discussion
This study revealed that the odds of attending an NCI/COG facility were substantially lower for AYAs than for younger pediatric patients. Similar to earlier studies, non-White patients, Hispanic patients, and patients who were uninsured or had Medicaid were significantly less likely to attend NCI/COG facilities when controlling for all other factors. 17 This is consistent with literature describing differential outcomes and, perhaps related, access to quality care for racial and ethnic minority groups, as well as patients who either lack insurance coverage or have Medicaid coverage.5,6,27 Furthermore, we document a significant distance gradient associated with NCI/COG attendance, with patients living within 20 minutes of an NCI/COG facility significantly more likely to attend that facility, compared with patients 20–39 or 40–60 minutes away. Of note, our primary analysis is restricted to patients living within 60 minutes of an NCI/COG facility (78% of the total population of patients) to examine associations for patients for whom an NCI/COG facility was most likely in their choice set.
We found that females were less likely than males to attend an NCI/COG facility, which has not been consistently found in similar studies.7–9,17 One reason for this finding could be explained by the proportion of breast carcinoma in our cohort. When the nearly 2000 cases of breast carcinoma in the cohort were omitted, the adjusted OR for likelihood of females attending an NCI/COG facility versus males was 0.998 and not significant (p = 0.959). These results hold significant implications for health care access for patients with breast carcinoma. Breast cancer is the most common cancer in female AYAs 15–39 years of age. AYAs with breast cancer often present with more aggressive disease and have worse outcomes compared with older women.28,29 This finding raises questions of how AYAs with breast carcinoma access NCI/COG facilities and whether access to such centers could lead to better outcomes. Additionally, as some studies indicate that women living in rural areas are more likely to be diagnosed with more advanced-stage breast cancer compared with women diagnosed with breast cancer living in nonrural areas, access to specialized centers with increased access to clinical trials and specialized services may especially be important to improve survival for AYAs with breast carcinoma living in rural areas.30–32
Additionally, we found that while NCI/COG facility attendance was high for children, attendance decreased significantly for AYAs. Even patients as young as 15–21 years at the time of cancer diagnosis were significantly less likely to attend an NCI/COG facility, with a steady decreased likelihood of attendance with increasing age. This phenomenon could be multifactorial and related to insurance changes as patients age off of parents' insurance coverage, lack of resources for those early in a career or in secondary school to access specialized care, and less experience navigating the health care system.
Finally, the results highlight the interplay between patient factors and NCI/COG attendance. The unadjusted mean attendance at NCI/COG facilities was higher among non-White patients compared with White patients; and attendance by Medicaid-insured patients was slightly higher when compared with those with private insurance (Table 2). However, both non-White and Medicaid-insured patients were significantly less likely to attend an NCI/COG facility in our adjusted models (Table 3). A large part of the explanation is that in Pennsylvania, as in many states, NCI/COG facilities are located in urban areas where there are greater numbers of both non-White and Medicaid-insured patients. 33
Our results, while consistent across sensitivity analyses, must be interpreted in the context of several limitations. First, this is a single-state study due to data restrictions. However, as Pennsylvania is the fifth most populous state in the United States and includes a number of different regions with significant urban and rural populations, this study represents a significant proportion of children and AYAs with cancer. Furthermore, despite using single-state information, our study complements and corroborates themes explored in other AYA-focused, state-based epidemiologic studies.15,17 Second, while we controlled for travel time, our measure is based on car travel. Although this is a commonly used transportation mode, many patients use public transportation, with perhaps significantly different travel times.34–38 Additionally, we did not evaluate the oncologic treatments that patients received, which for some malignancies, such as acute lymphoblastic leukemia, may carry more importance than the facility type where patients received treatment. 39 Furthermore, as this is a single-state study, we were unable to capture patients who received care at NCI/COG facilities in neighboring states. Last, while we focus on receipt of care at an NCI/COG facility, there may be other important metrics of quality care to evaluate health care access for AYAs with cancer. This study's results are by no means inclusive of all factors that account for quality care, including expertise of the treating physician, access to clinical trials, adherence to evidence-based guidelines, and implementation of medical and psychosocial support.
One of the study's strengths was using PCR data, which allowed us to capture all pediatric and AYA patients in the state. Based upon multiple factors, including completeness and accuracy, the PCR data received gold (highest) recognition for the years 2010–2011 and 2013–2015, and silver for 2012 from the North American Association of Central Cancer Registries. Compared with studies that used hospital admission data, we were able to capture data of all patients, not just those admitted to a hospital, and were also able to control for diagnosis stage. 17 Finally, we add to the epidemiology literature of AYA cancer care by focusing on a state not previously studied to understand whether care patterns at NCI/COG facilities were consistent with other states.
Our study's results have significant implications for understanding how AYAs access cancer care. Observing that AYAs with cancer who are non-White or Hispanic, uninsured or with Medicaid coverage, female, and those living further from NCI/COG institutions were all significantly less likely to receive care at NCI/COG facilities, the study highlights patients that providers need to particularly target to ensure receipt of quality care. Furthermore, as the rural Pennsylvania population grows, it is imperative for patients living in this area to have access to specialized care centers. The disproportionate access of NCI/COG facilities for patients in rural areas may only continue to grow across racial and ethnic lines, as the minority population in rural Pennsylvania continues to grow. From 2000 to 2015, the population of residents who identified as non-White and/or Hispanic increased from 5% to 9% of the rural Pennsylvania population. 20
One strategy that may increase attendance at NCI/COG facilities is creation of more satellite or affiliate facilities, as is occurring in several Pennsylvania hospital systems. However, it is unclear whether the quality of care at satellite facilities mimics the main institution insofar as access to and quality of all aspects of care. 40 Quality measures to ensure the same access to clinical trials and supportive care programs could be implemented to ensure the same caliber of care at satellite or affiliate facilities as at the main institution, although this is often challenging and unrealistic to maintain. An area of future research could focus on whether affiliates or satellite facilities of NCI-designated comprehensive cancer centers or COG centers offer the same quality of care as the main institution. An additional area of future focus could evaluate how AYAs access cancer care at other consortium models such as NCI Community Oncology Research Program (NCORP) or National Clinical Trial Network (NCTN) sites. These models have been preliminarily studied in AYAs.41,42
Conclusions
In conclusion, compared with pediatric patients with cancer, AYAs with cancer in Pennsylvania have disproportionate attendance at NCI/COG facilities after controlling for covariates, including age, insurance status, race, ethnicity, gender, cancer type, stage, year of diagnosis, and geographic distance. Efforts to ameliorate the infrastructure within which AYAs receive cancer care must focus on addressing these covariates accounting for disproportionate attendance to improve the access to care and outcomes of this vulnerable patient population.
Footnotes
Acknowledgments
The authors acknowledge the assistance of the Community Sciences and Health Outcomes Shared Resource of Penn State Cancer Institute for access to cancer registry data. The Pennsylvania Department of Health specifically disclaims responsibility for any analyses, interpretations, or conclusions. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Disclaimer
Portions of these data were presented at the 2017 Penn State Cancer Institute Retreat.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Penn State Cancer Institute and the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant UL1 TR002014.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.