
Abstract
Purpose:
Neutrophil-to-lymphocyte ratio (NLR) is considered as a prognostic factor in some patients with hepatocellular carcinoma (HCC). This factor has not been extensively examined in young HCC patients. The objective of this study is to assess whether pre-treatment NLR could predict the survival in young HCC patients implemented minimally invasive treatment.
Methods:
Young HCC patients treated by transarterial chemoembolization (TACE) combined with radiofrequency ablation (RFA) at our institutes from 2008 to 2017 were retrospectively reviewed. The best cutoff value of NLR was determined with time-dependent receiver operating characteristic curve analysis. The associations between overall survival and various potential risk factors, including tumor size, vascular invasion, hepatitis B virus infection, Child–Pugh scores, Barcelona Clinic Liver Cancer (BCLC) stage, aspartate aminotransferase (AST), and NLR, were analyzed.
Results:
Data were collected from 47 HCC patients who were <45 years old (range 30–44). In univariate analysis, vascular invasion (p = 0.001), tumor maximum diameter (p = 0.000), BCLC stage (p = 0.001), HBsAg positive (p = 0.025), AST ≥2 × upper limits of normal (ULN) (p = 0.027), and NLR ≥3.09 (p = 0.027) were predictors for poor survival in young HCC patients treated by TACE combined with RFA. The multivariate Cox proportional hazard model analysis showed that except NLR (hazard ratio [HR] = 0.720, 95% CI 0.287–1.808, p = 0.485), tumor maximum diameter ≥5 cm (HR = 0.444, 95% CI 0.199–0.991, p = 0.047) and AST ≥2 × ULN (HR = 4.578, 95% CI 1.544–13.575, p = 0.006) were independent indicators for poor prognosis.
Conclusion:
Pre-treatment NLR ≥3.09 is related to poor prognosis of young HCC patients implemented minimally invasive treatment. However, it is not an independent indicator for prognosis.
Introduction
Hepatocellular carcinoma (HCC) is one of the most common malignancies and the third leading cause of cancer-related deaths worldwide, especially in Southeast Asia and North Africa. 1 The number of patients in China accounts for more than a half of the world. The age of high-risk population in China ranges from 55 to 65 years old. However, the incidence of young HCC patients shows an increasing tendency in recent years. 2
The young patients with HCC are characterized by occult onset, rapid progress, and poor prognosis. Most of the patients have lost the opportunity of surgery when they are diagnosed. So the patients are usually treated with minimally invasive treatment, such as radiofrequency ablation (RFA), and transarterial chemoembolization (TACE). 3 Exploring an indicator that can assess the severity and predict prognosis in young patients with HCC treated by TACE combined with RFA represents a central issue for improving clinical management.
Systemic inflammatory response has been proved that it plays an important role in tumorigenesis, development, and metastasis. 4 The inflammatory factors secreted by tumor cell can stimulate the tumorigenesis, angiogenesis, vascular invasion, and metastasis. 5
More and more researchers focus on the progression of neutrophil-to-lymphocyte ratio (NLR), which is one of the inflammatory factors and defined as a ratio of the neutrophil-to-lymphocyte count in peripheral blood. Pieces of evidence suggest that NLR is correlated with poor prognosis in different malignancies, including colorectal, gastric, and breast cancer.6–8 In HCC, the impact of NLR on recurrence and survival has been evaluated in large cohorts of patients including those treated by surgical resection, transplantation, RFA, and TACE.9–12 Nevertheless, this factor has not been extensively examined in young patients with HCC implemented minimally invasive treatment. The purpose of this study is to evaluate the prognostic performance of NLR for young patients with HCC who underwent TACE combined with RFA.
Methods
Patients
This retrospective study was conducted on 47 HCC patients (44 male and 3 female, age range 30–44 years, median 40 years) consecutively treated at Beijing Ditan Hospital of Capital Medical University and Peking University International Hospital from 2008 to 2017. Inclusion criteria were as follows: cytological/histological diagnosis by biopsy or two imaging techniques showing typical features of HCC, Eastern Cooperative Oncology Group performance status 0–1, Child–Pugh classification A or B, and no extrahepatic metastases. Exclusion criteria were Child–Pugh classification C, severe underlying cardiac or renal diseases, esophageal or gastric variceal bleeding or hepatic encephalopathy, or active infection. All patients received minimally invasive treatment, including TACE and RFA.
NLR is defined as a ratio of the neutrophil-to-lymphocyte count in peripheral blood. Patients were stratified into high and low NLR groups based on the levels of NLR within 7 days before TACE. RFA was implemented 1 week after TACE. All patients signed informed consent.
All patients were regularly followed up per month in the first half of a year according to institutional practice, including a complete physical examination, hematologic and biochemistry profiles, serum alpha fetoprotein, chest X-ray, and abdominal computed tomography or magnetic resonance imaging. Half a year later, these were administered every 3 months. Tumor relapse was defined by clinical, radiological, and/or pathological diagnoses. Overall survival (OS) was assessed from the date of diagnosis until death from any cause. The last follow-up date for this study was December 2017.
Statistical analysis
The data were analyzed using SPSS for Windows (Version16.0). The best cutoff value of preoperative NLR was determined by time-dependent receiver operating characteristic (ROC) curve analysis. Independent χ 2 tests were used to compare categorical variables. Continuous variables were compared using unpaired T tests. The OS curves were analyzed using the Kaplan–Meier method and the differences between groups were compared by log-rank test. Unadjusted and adjusted hazard ratios (HRs) by baseline characteristics were calculated by the Cox proportional hazards model. All statistical tests were two sided and differences were considered significant with p < 0.05.
Results
Most patients (61.7%) suffered from cirrhosis and the most frequent etiology of liver disease was hepatitis B virus infection (91.5%). Child–Pugh classification at the time minimally invasive treatment was initiated was A in 87.2% of patients and B in 12.8% of patients. With respect to stage, 51.1% of patients were Barcelona Clinic Liver Cancer (BCLC) stage B and 48.9% of patients were BCLC stage C. The patients' characteristics are given in Table 1.
Comparison of Clinical Parameters of Hepatocellular Carcinoma Patients Between the Low and High Neutrophil-to-Lymphocyte Ratio Groups (Chi-Square Test)
ALF, alpha fetoprotein; BCLC, Barcelona Clinic Liver Cancer; ULN, upper limits of normal.
Selection of the best cutoff value for NLR
The NLR was defined as the ratio derived from division of the neutrophil count by the lymphocyte count. NLR = 3.09 was considered to be evaluated by time-dependent ROC curve (AUC = 0.681; p < 0.05) (Fig. 1). Therefore, all patients were divided into either a low (NLR <3.09) NLR group or a high (NLR ≥3.09) NLR group. There were 26 patients in the low NLR group and 21 patients in the high NLR group.
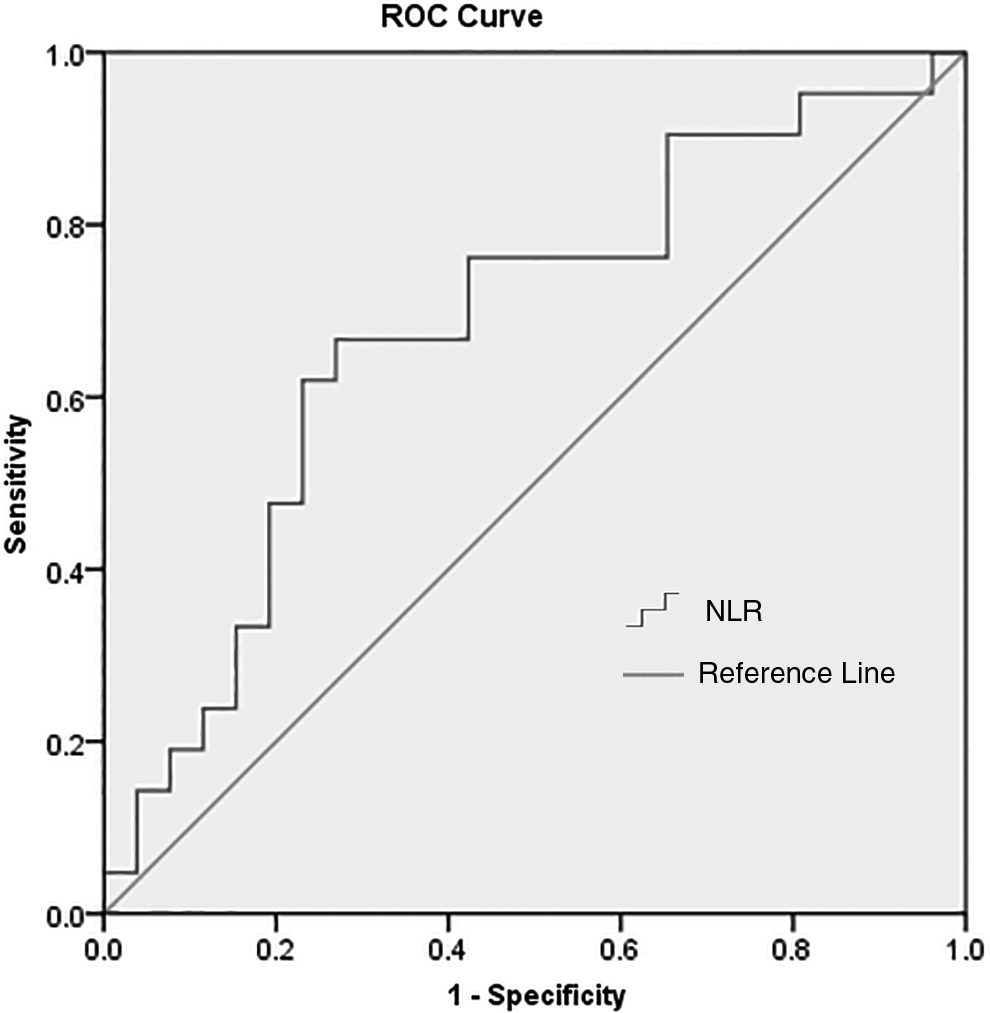
ROC curves analysis for NLR predicating prognosis for young patients with HCC implemented minimally invasive treatment. According to the relationship between NLR in peripheral blood and OS, we established a time-dependent ROC curve. The meaning of vertical coordinate was the sensitivity of NLR, predicating prognosis for young patients with HCC. And the meaning of horizontal coordinate was the outcome that was calculated by subtracting specificity of NLR for young patients with HCC from 1. When NLR was equal to 3.09, the area under curve was 0.681, and the Youden index was the largest. Its sensitivity was 67% and specificity was 73% (p < 0.05). NLR, neutrophil-to-lymphocyte ratio; OS, overall survival; ROC, receiver operating characteristic.
Survival analysis
The 1-, 3-, and 5-year OS rates for all patients were 55.3%, 29.8%, and 14.9%, respectively. The 1-, 3-, and 5-year OS rates for the low NLR group patients were 73.1%, 42.3%, and 19.2%, respectively. However, those for high NLR group were 33.3%, 14.3%, and 9.5% respectively. The median OS of patients in the high NLR group was 8 months (range, 1–73 months) compared with 24.5 months (range 3–86 months) in the low NLR group (Fig. 2).

Comparison of overall survival rates in the low (<3.09) and high (≥3.09) NLR groups. From this figure we found that the 1-, 3-, and 5-year OS rates for the low NLR group patients were higher than that of high NLR group. It had significant difference.
In univariate analysis, vascular invasion (p = 0.001), tumor maximum diameter (p = 0.000), BCLC stage (p = 0.001), hepatitis B surface antigen positive (p = 0.025), AST ≥2 × upper limits of normal (ULN) (p = 0.027), and NLR ≥3.09 (p = 0.027) were predictors for poor prognosis in young HCC patients treated by TACE combined with RFA (Table 2). The multivariate Cox proportional hazard model analysis showed that except NLR (HR = 0.720, 95% CI 0.287–1.808, p = 0.485), tumor maximum diameter ≥5cm (HR = 0.444, 95% CI 0.199–0.991, p = 0.047) and AST ≥2 × ULN (HR = 4.578, 95% CI 1.544–13.575, p = 0.006) were independent indicators for poor prognosis (Table 3).
Prognostic Factors for Overall Survival by Univariate Analysis
OS, overall survival.
Risk Factors for Overall Survival by the Multivariate Cox Proportional Hazards Regression Model
HR, hazard ratio.
Discussion
In recent years, many studies found that the level of NLR was related to OS in HCC patients. Gomez et al. 13 analyzed 96 HCC patients after hepatectomy, which is the first study of the relationship between NLR and prognosis in HCC patients. Many researches14–16 have reported that NLR is not only correlated with OS of HCC patients who underwent radical resection or liver transplantation, but also related to OS of HCC patients treated by minimally invasive treatment or molecular targeting therapy. However, few studies about relationship between NLR and young patients with HCC treated by minimally invasive treatment have been done so far.
So this study retrospectively analyzed clinical data from 47 young patients with HCC treated by minimally invasive treatment to make a primary exploration. The purpose of this study is to explore the relationship among pre-treatment NLR, clinicopathological characteristics, and OS. We found that the 1-, 3-, and 5-year OS rates for two groups of patients were different obviously, the survival rate in the low NLR group was higher than that in the high NLR group.
The median OS in the low NLR group was significantly higher than that in the high NLR group (23 months vs. 7 months, p = 0.027). The results showed that pre-treatment high NLR in young patients with HCC predicted shorter survival. Tan et al. 17 also confirmed it. The outcome was the low NLR group patients had a survival advantage, the OS of two groups was 31 and 24 months, respectively (p < 0.05). So the study suggested that pre-treatment NLR ≥2.2 predicted poor survival, and NLR could be a prognosis factor for the locally advanced HCC patients treated by RFA.
One research 18 suggested these factors including NLR, AST, BCLC stage, tumor size, tumor number, and portal venous emboli were prognosis predictors in HCC patients treated by TACE. Our study also supported the argument. In univariate analysis, NLR ≥3.09, AST ≥2 × ULN, vascular invasion, tumor maximum diameter ≥5 cm, BCLC stage, and hepatitis B surface antigen positive were predictors of poor prognosis in young HCC patients treated by RFA combined with TACE.
Our study took into account the baseline situation and univariate analysis, and adjusted these factors including NLR, AST, vascular invasion, tumor maximum diameter, BCLC stage, and hepatitis B surface antigen positive. The multivariate Cox proportional hazard model analysis showed that NLR was not an independent indicator for OS, but tumor maximum diameter ≥5 cm (HR = 0.444, 95% CI 0.199–0.991, p = 0.047) and AST ≥2 × ULN (HR = 4.578, 95% CI 1.544–13.575, p = 0.006) were independent indicators for poor prognosis.
He et al. 19 analyzed 216 HCC patients treated by TACE, and found that pre-treatment NLR correlated with the prognosis of these patients. Higher NLR predicted poor survival in advanced HCC patients after TACE. Higher NLR was an independent unfavorable prognostic factor in the patients. Taussig et al. 20 reviewed the data of 86 HCC patients treated by intra-arterial therapy. NLR >3 predicted worse disease control in HCC patients and was a predictor of tumor early progression. In our study, the best cutoff value for NLR was 3.09, which was in accordance with the literature. It was evaluated by time-dependent ROC curve.
There was no significant difference in BCLC stage through multivariate Cox proportional hazard model analysis. As the sample size was not enough, the outcome had divergence deviation. AST was a sensitive and reliable biomarker of liver injury. Some liver diseases could lead to hepatocyte mitochondria damage, thus causing AST to release into blood. 18 Witjes et al. 21 reported that higher AST had something with OS in HCC patients. In our study, it also proved that pre-treatment higher AST predicted poor survival in young HCC patients treated by minimally invasive treatment. NLR was an influencing factor for survival of HCC patients implemented minimally invasive treatment, but were not an independent prognostic factor. This was similar to Fan et al.'s 22 clinical findings.
In our centers, treatment strategy of TACE combined with fractionated RFA was selected for patients with large or multiple tumors, and the survival data would come out in the near future. Owing to insurance reimbursement and high cost of medicine, the patients were never given sorafenib according to their wishes during the study.
Pre-treatment NLR ≥3.09 is only related to poor OS, not an indicator for prognosis in young patients with HCC implemented minimally invasive treatment. In addition, tumor maximum diameter ≥5 cm and AST ≥2 × ULN are independent unfavorable prognostic factors.
NLR, as a predictor for survival, is convenient and economy. In future, NLR may become a valuable biomarker for prognosis in cancer patients. However, there are some insufficiencies in these researches. First of all, the selection of the best cutoff value for NLR is different. Most cutoff values for NLR range from 2 to 5. Some are evaluated by time-dependent ROC curve, but some are evaluated by sample mean. Second, this sample size is not enough. So some outcomes are discrepant. In future we need to choose the best cutoff value for high NLR, large sample size, and multicenter prospective random study, which can provide adequate theoretical basis to guide clinical treatment.
Footnotes
Author Disclosure Statement
No financial interests exist.
Funding Information
There is no funding for this study.