
Abstract
This review explores the literature on experiences of young people (15–39 years) living with cancer from nonmetropolitan areas, given most available research has focused on those living in major metropolitan areas. The purpose of the review was to inform (a) clinical practice and (b) future research on young people living with cancer in nonmetropolitan areas. An integrative review method explored peer-reviewed publications in CINAHL, Medline, PsycINFO, SSCI, PsycARTICLES, Socindex, and Google Scholar for literature published over the past 20 years. Twelve studies (reported in 17 articles) were eligible for inclusion, of which most (n = 8) had been conducted in Australia. Findings highlighted “the tyranny of distance” from metropolitan specialist cancer care centers negatively affected young people's health (e.g., delayed diagnoses), with financial distress1, psychosocial, cultural, and other challenges resulting. Negative effects were heightened during major treatment transitions at diagnosis, during, and after cancer treatment. One study found some Indigenous Australians did not report symptoms and refused referrals if it necessitated travelling long distances. Five studies did not report greater challenges experienced by nonmetropolitan compared with metropolitan respondents. Health care professionals helping young people can mitigate negative challenges through education and support at diagnosis about financial distress and psychosocial challenges. We recommend further research target ways to minimize delays in diagnosis, reporting of symptoms or accepting allied health referrals, psychosocial upheaval, financial distress, and explore issues particular to First Nations people, to inform services how to meet unique needs of young people living with cancer from nonmetropolitan areas.
Introduction
Young people living with cancer experience many challenges. Survival rates for young people living with cancer are less than those of children (<15 years), or adults older than 29 years.2–5 Adolescence and young adulthood encompasses significant growth, change, and unique psychosocial needs, which can be significantly affected by a cancer diagnosis.2,6–8 Young people diagnosed with cancer during this developmental life stage endure physical, financial, and emotional upheaval through disruptions to education and work, social isolation, and difficulties comprehending medical information.9–12 Young people require disease management strategies to navigate these challenges,6,9,11–14 including more specialized, age-appropriate services.2,6
Greater international incidence and death rates for those with cancer in nonmetropolitan areas, along with Australian data showing young people with cancer from nonmetropolitan areas having higher incidence and death rates of cancer than those from metropolitan areas, form part of the rationale to conduct this literature review.
Rurality was associated with poorer cancer survival in developed countries in a 2018 meta-analysis of 39 studies from the United States, Canada, Australia, New Zealand, the United Kingdom, France, and Europe. 15 Similarly, worse survival rates for cancer patients living in rural areas compared with those living in urban regions in high income countries (Australia, United States, Europe, Canada, and New Zealand) was found in a 2019 systematic literature review. 16 There are limited international research data comparing cancer incidence and death rates between metropolitan and nonmetropolitan young people diagnosed with cancer.
Data in Australia show young people from nonmetropolitan areas have comparatively worse health, 17 higher incidence rates of cancer, and are more likely to die from their cancer than those living in cities. 18 Australia's First Nations people (Indigenous Australians), including young Indigenous Australians with cancer, 19 are more likely to be diagnosed later and with more advanced cancer, wait longer for surgery, and are less likely to have cancer treatment than non-Indigenous Australians. 20 The further an Indigenous Australian cancer patient lives from metropolitan centers, the greater the likelihood they will not survive their cancer. 21
There is heightened anxiety and distress for young people living with cancer at key transition points of diagnosis, treatment changes, and adjustment to life post-treatment. 22 Important decisions are often required at these times around treatment, school or work, personal relationships, and other psychosocial issues. Transition points could impact more on those from nonmetropolitan areas given the need to travel away from, or back home, at such times.
Researchers in Australia have proposed identifying and testing innovative models like tele-health to reach young people living in nonmetropolitan areas, 23 or improving links for young people with dedicated youth cancer services located in metropolitan areas. 24 Although advances in models of care exist,24,25 research informing them has come largely from studies conducted in major metropolitan areas. 26 There is consequently a gap in knowledge to guide multidisciplinary health professionals on the unique experiences of young people living in nonmetropolitan areas across the cancer care trajectory.
Building on this existing literature, together with the authors' combined clinical experience working in adolescent and young adult social work and psychology across remote, regional, and metropolitan locations (JS and USD), we undertook a literature review exploring the experiences of young people (15–39 years) with cancer. The purpose of this review was to inform clinical practice with, and future research on, young people living with cancer in nonmetropolitan areas. We aimed to address three research questions:
What challenges exist for young people in nonmetropolitan areas living significant distances from their cancer care? What psychosocial challenges do young people with cancer from nonmetropolitan areas experience? Do young First Nations people with cancer living in nonmetropolitan areas report unique or different experiences of living with cancer?
Methods
The authors conducted an international, integrative literature review27,28 to explore what is currently known about young people living with cancer in nonmetropolitan areas. Integrative literature reviews are helpful in gaining a comprehensive understanding of specific health care issues,27,29 generate new frameworks and perspectives on new and emerging topics, 30 and have been used in other reviews of young people living with cancer. 25 The integrative review allows for inclusion of diverse methodologies27,29 allowing the exploration of qualitative and quantitative data from chosen studies in this review. Summarizing the current state of knowledge of young people living with cancer in nonmetropolitan areas in this article is intended as a service to clinicians working with this health population and other researchers. 28
Eligibility criteria
Peer-reviewed publications eligible for inclusion comprised empirical research, evaluations, and literature reviews related to young people living with cancer in nonmetropolitan areas. Eligible articles contained data on young people 15–39 years of age, allowing for international variations on age ranges used to define adolescents and young adults, and addressed the psychosocial needs and/or experiences of young people living with cancer in nonmetropolitan areas. Our definition of “nonmetropolitan” allowed any regional, rural, or remote area as defined by the authors of each study, relative to their local context. Typically, this meant specialist cancer treatment centers were not nearby, as these were located in metropolitan centers. Publications such as editorials, conference abstracts, theses, and newspaper articles were excluded.
Information sources and search strategy
Research articles were selected from these databases—CINAHL, Medline, PsycINFO, Social Sciences Citation Index (SSCI), PsycARTICLES, Socindex, and Google Scholar. Keywords used were cancer, patient*, neoplasm*, adolescent*, young adult*, teenager*, youth, young people, social work, regional, rural, remote, non-metropolitan, urban, metropolitan, psychosocial, information, support, experience*, need*, living with, diagnosed with, comparing, Aboriginal, Torres Strait Islander and Indigenous. Cited studies and reference lists in relevant articles were also used to extend the scope of the search. This search took place between 2017 and 2018. Twelve studies were chosen, reported on in 17 articles, ranging in research time frames from 1997 to 2016. Further searches up to April 2019 yielded no new studies to include.
Study selection
The age range for participants of articles included in the review was 15–39 years. Given the paucity of literature in this area, we took a broad approach to capture the most relevant data, by including studies in adult cancer patients that included young adults. Figure 1 outlines the study/article selection.
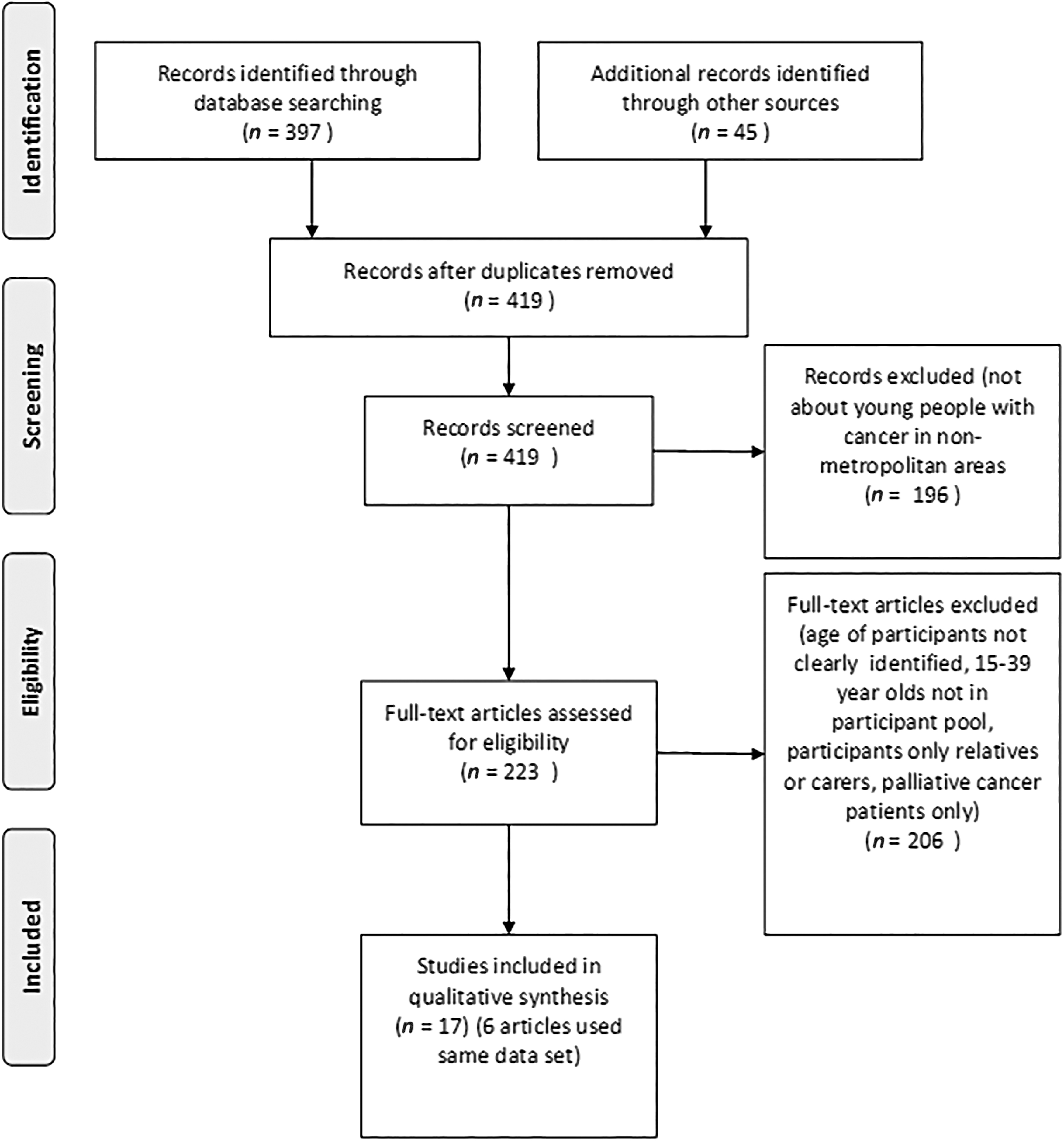
PRISMA Flowchart Illustrating the Literature Search.
Data extraction, evaluation, and synthesis
The final 12 studies chosen contained some data on young people 15–39 years living with cancer in nonmetropolitan areas. It is acknowledged that some of the studies with young people in them did not report specifically on data from those young people—rather, the results reported were for the entire participant age range.
Given the paucity of research on young people living with cancer in nonmetropolitan areas, the authors intend that this literature review at least provides a comparison point for emergent themes and issues arising in future research. No quality assessment was conducted of the studies given the small number of them, some of which may be considered weak against qualitative reporting guidelines. 31 Coding of the findings was conducted line-by-line for included studies, and then grouped into descriptive themes. Data were extracted and thematically coded into descriptive themes, then fields, relevant to the aims through thematic synthesis, 32 reflecting the integrative methodology.27,28 Five final analytical themes were chosen to report on the results through integration and synthesis. 32 A map of the descriptive and analytical themes is given in Table 1.
Map of the Descriptive and Analytical Themes
 The descriptive themes were all grouped into overarching analytical themes.
The descriptive themes were all grouped into overarching analytical themes.
Results
Twelve studies reported over 17 articles were found in the empirical literature that met the inclusion criteria (Table 2). Six of the published articles (McGrath40–46 ) in Table 2 relate to the same data set of 45 participants in Australia—counted as one study. After Australia, where most of the included studies originated (n = 8), the remainder of the studies originated from Canada (n = 2), the UK (n = 1) and the United States (n = 1).
Reviewed Studies Addressing Young People Living with Cancer in Nonmetropolitan Areas, Ordered from Those Specifically About Young People to Those That Include Young People in Participant Pool (McGrath Articles in Chronological Order)
* NA, Not applicable.
** Research base of same 45 participants and data were used in these articles.
Three studies focused exclusively on young people (between 15 and 39 years),22,33,34 two included children in the participant pool,35,36 and the remainder sampled adult populations 18 years and older.37–48 Of the studies included, issues identified included distance from and/or access to specialist cancer care services with the health risk of delayed (financial toxicity 1 ) diagnoses, psychosocial issues, and financial distress; issues for First Nations people living with cancer with the health risk of not reporting symptoms or accepting referrals, and challenges these issues create at key transition points (diagnosis, during, and after cancer treatment) along the cancer care trajectory for young people. Five studies reported no greater negative effects for those from nonmetropolitan areas.22,34,37–39,47 Participants from four studies37,38,41–43,46,48 made suggestions to address identified challenges.
The “tyranny of distance” from specialist cancer care services
Distance from metropolitan centers was a barrier in accessing cancer care services when living in nonmetropolitan areas in eight Australian studies.35,37,41–46 Paul et al. found nonmetropolitan respondents were 17 times more likely to list distance as a barrier than metropolitan respondents. 37 In the same study, half of those living in nonmetropolitan areas needed to relocate to metropolitan specialist centers for cancer care they required. 37 Stress and increased financial costs were associated with the demands of travel and relocating for treatment.41,42,45 One study by McGrath showed long length of stays (up to 281 days) in metropolitan centers as far as 1800 km away from home. 35 Relocation for treatment to metropolitan cancer care centers involved long-term, significant negative repercussions for patients and families psychosocially and financially. 35
Distance from metropolitan centers also led to delayed diagnoses. Delayed diagnosis was another consequence of distance from specialist cancer care centers. 34 Young adults reported delayed diagnoses because of not being taken seriously by health services or physicians, in some cases for years. One young adult stated their physician assumed they were too young to have the kind of cancer they were subsequently diagnosed with, and attributed this to lack of expertise of that physician from the nonmetropolitan area. 34
The research of Marris et al. 33 found young people preferred to travel if required to receive specialist care. Young people benefitted from travelling to metropolitan cancer care centers specializing in treatment for young people for many reasons, including access to age-appropriate environments of care, information, peer support, recreational and vocational support, and staff expert in their cancer types and care needs. 33 Given these benefits, being treated close to home was a low personal priority for the patients. 33 Young people were prepared to travel half a day or more, or “any distance” to receive treatment they needed in a specialist unit. 33
Psychosocial issues and financial distress
Nine studies reported negative psychosocial and financial challenges associated with travelling away for treatment.22,34,36–46,48 Psychosocial challenges related to dislocation from family, friends, work, school, and community. 41 Support structures of home and family are particularly important at times such as cancer diagnosis or relapse. 43 If decisions need to be made at the metropolitan center, being away from usual extended support networks in the community at a time of heightened anxiety and distress could adversely affect decision-making processes if that support is unavailable. 43 McGrath found that despite a reported longing for those from nonmetropolitan areas to return home while having their cancer treatment in metropolitan centers, participants did not always share those feelings with treating staff in metropolitan centers 42 and if they did, they questioned whether staff understood the significance of their desire to return home. 43
Returning home after treatment was identified as a transitional point that brought new/additional challenges. 36 Although participants' needs changed over time, the highest need upon returning home related to emotional, medical, and practical support. 36 Participants wanted emotional support from nonprofessional sources like family, friends, and others going through a cancer experience. 36 Young adults from nonmetropolitan areas reported lower levels of community support than metropolitan participants, with metropolitan participants reporting almost three times more in comparison 34 ; this included practical (e.g., meals, financial assistance) and emotional (e.g., faith-related support, cancer support organizations) support. Returning home after treatment therefore brought both psychosocial challenges and benefits.
Financial distress was a negative issue in most studies. Financial costs occurred at diagnosis, during treatment, with travel and accommodation, care of family and friends during relocation, and parking (if driving a vehicle). 45 Costs associated with travelling away included increased cost of the weekly shop in metropolitan areas being greater than at home in the nonmetropolitan area, more telephone calls, loss of local support (family/friends), medical expenses, accommodation, maintaining two households (one's home and also accommodation at the metropolitan site), and other incidental travel costs. Loss of income from work exacerbated these costs. 40 McGrath's40–46 research found financial distress was more likely for those who lose or reduce employment, have limited or no work cover or other leave, limited savings and major financial debts.40–46 A combination of these factors was found to exacerbate acute and long-term financial distress. 44
Associated challenges of financial distress affected decision-making around choices people made for their cancer treatment. Mathews et al. found nonmetropolitan residents were influenced in decisions about kinds of cancer care they undertook if they had travel, medical and childcare costs. The authors stated these findings could mean cancer patients may forgo, or alter, their care because of these costs. 38
Unique considerations/challenges for First Nations peoples
In the only study focused on First Nations peoples, Meiklejohn et al. explored the experiences of Indigenous Australians (18 years and older) from nonmetropolitan areas with cancer. 48 Similar challenges were raised as in other studies, including restricted access to cancer care services and travel to specialist cancer care centers.
Travel challenges included length of time it took to travel to metropolitan treatment centers and associated increased financial costs involved. The burden of potential travel was so significant for some, it was a consideration in whether they reported symptoms to their local family doctor. Travel was also a factor in whether participants would accept referrals to allied health services (e.g., dieticians and physiotherapists) if patients assumed it involved having to travel to access those services. Psychosocial challenges included poor coordination of care between services, lack of specific cancer knowledge by local family doctors and health centers, time away from family and community supports, costs incurred for travel, accommodation and medication, and physical discomfort during long journeys. 48
Studies reporting no greater negative effects for those from nonmetropolitan areas
There were psychosocial benefits associated with living in nonmetropolitan areas, some already noted. Four quantitative studies22,37,39,47 found living in nonmetropolitan areas had no greater negative effects than metropolitan participants' experiences of cancer financially, socially, or otherwise. Miedema et al.'s qualitative study found financial stress was no greater for nonmetropolitan than metropolitan participants. 34 Limited access to specialized cancer care resources did not decrease participants' satisfaction with services. 34 The authors surmised that levels of satisfaction relate to expectations, with participants in nonmetropolitan areas not expecting high levels of care in light of limited resources. 34
Three quantitative studies found no correlation between respondents' reported unmet needs and coming from a nonmetropolitan area.22,39,47 Cox et al. measured unmet needs against racial demographics and found no correlation. 47 It was expected that higher levels of unmet need would be reported by those living in nonmetropolitan areas in the aforementioned three studies.22,39,47 Informal networks like family and friends in nonmetropolitan communities may provide a significant source of support, which White et al. stated could account for lower reported unmet needs in their study. 39
Potential solutions to identified challenges
Participants in four studies offered ways to address the challenges (health risks, distance, financial, psychosocial, transitional, and/or cultural issues) they experienced living in nonmetropolitan areas.37,38,41–43,46,48 Solutions encompassed being treated locally or in their region where possible.37,43 “Fly-in, fly-out” health services (or visiting cancer specialists/services) were recommended by some participants.38,42 Shared cancer care between nonmetropolitan and metropolitan sites42,43 was also offered as a way of keeping people receiving treatment closer to home. Tele-health—the delivery of health care at a distance using information communication technologies—was another suggestion.42,44,48
Tele-health addresses some important cultural needs for Indigenous Australians living in nonmetropolitan areas, such as having other family members, loved ones, or culturally/spiritually important community members present. 48 Tele-health also provides the possibility of virtual multidisciplinary teams.38,42 Indigenous Australian participants further suggested that in the case of multiple follow-up appointments, these should all be coordinated so only one travel journey to the metropolitan center was required. 48
Service delivery improvements were suggested, which included (a) building trusting, long-term relationships with health professionals at specialist cancer care and local health services, especially important for Indigenous Australians to improve equitable access to culturally appropriate care, 48 (b) more flexible services for those requiring treatment but still working, including access to appointments outside of “nine-to-five” office hours or on weekends, 37 (c) discussing financial distress and how to minimize it at diagnosis, 46 and (d) providing financial assistance and free parking, medications, treatments, and transport to tests or treatment. 37
Discussion
This literature review aimed to inform clinical practice and future research by synthesizing current knowledge regarding the unique experience and challenges faced by young people living with cancer in nonmetropolitan areas. All studies contained beneficial information to inform clinical practice to varying degrees. Nine studies reported significant and negative cancer care, financial and social challenges experienced by young people living with cancer in nonmetropolitan areas; however, this was not the case in all studies. Four studies provided potential solutions to identified challenges their participants raised. We explore these health risks, challenges, and potential solutions.
The literature search was an international one; however, of the 12 studies found, eight were from Australia, two were from Canada, one was from the United Kingdom, and one the United States. One explanation of the more extensive evidence base in Australia could be that it is geographically dispersed with a low population density. 49 The tyranny of distance is a well-known barrier to accessing health services in Australia, which has led to numerous strategies to mitigate its impact. These efforts have ranged from establishing charitably funded accommodation facilities for patients and their families, like Ronald McDonald Houses, 50 Leukaemia Foundation, and Cancer Council Lodges,51,52 to patient travel subsidy schemes run by state government health services. 53
Distance from specialist cancer care services was linked with health risks, psychosocial and financial challenges faced by young people living with cancer in nonmetropolitan areas. Some effects of these challenges were quite serious, such as delays in diagnosing cancer, 34 and in the case of Indigenous Australian patients forgoing cancer treatment or referrals to mitigate the burden of travel. 48 Studies of older cancer patients have similarly found patients would forgo cancer treatment or referrals to avoid having to travel,54,55 so these health risks are not necessarily unique for young people with cancer in nonmetropolitan areas.
In the Australian context, given the higher overall incidence and mortality rates of cancer for young people in nonmetropolitan areas, 18 it does equate to a greater health risk for young people. It similarly increases the risk for young Indigenous Australians living with cancer in nonmetropolitan areas, who typically are diagnosed later with more advanced disease, wait longer for surgery, are less likely to have cancer treatment, and have higher mortality rates that non-Indigenous Australians. 21
The level of specialist care required to diagnose and treat the various forms of cancer young people are diagnosed with is generally not available in most nonmetropolitan areas.33,56 Therefore, travel or relocation is usually required for young people diagnosed with cancer from nonmetropolitan areas.33,34,37,42 Although some young people have expressed preparedness to travel to receive specialist cancer care, 33 others found distance to be a barrier to accessing cancer care.41,42,44,45 Given that financial costs and worse, financial distress are endemic for nonmetropolitan cancer patients, addressing this with patients at diagnosis is important given that many with cancer do not know how to access financial advice or assistance. 46
Although the studies highlighted challenges of living away from specialist cancer care, they also offered ways some challenges could be addressed. These included uses of tele-health where possible and preparing clients for financial distress by early referral to their own superannuation schemes, medical and life insurance schemes, or government and other forms of financial assistance and counseling. We will now explore other clinical implications for practice and ideas for future research.
Clinical Implications and Future Research
Lack of equitable access to health services is a central concern for many helping professions.57–61 This review provides data to inform clinicians on ways to mitigate risks distance causes to the health and well-being of young people living with cancer in nonmetropolitan areas, including (a) coordinating multiple appointments at metropolitan cancer centers to occur during the same visit to reduce some of the negative impacts of having to travel away, 48 (b) building long-term trusting relationships between staff and patients at both metropolitan and nonmetropolitan sites, especially important for First Nations people, 48 (c) flexible appointment times for patients to attend outside work hours, 37 (d) preparing young people at the point of diagnosis for financial distress including where to access advice, 46 (e) making available tele-health facilities or assisting with long-distance telephone calls to enable young people to continue contact with families and loved ones, (f) facilitating financial or accommodation assistance, where available, to bring a loved one to the metropolitan center for a time, and (g) expanding access to clinical services through incorporating new technologies as delivery mechanisms.
Tele-health technologies have proven to be acceptable, feasible, and safe when used to increase access to psychosocial screening assessments among adolescent and young adult cancer patients in Australia, 62 as well as in facilitating access to group-based psychological support in early cancer survivorship. 63 Particularly in settings where low patient numbers/density preclude a “critical mass” of young cancer patients at nonmetropolitan sites, it will be important for clinical teams to develop ways of integrating tele-health technologies into their delivery of routine care to expand access to gold-standard treatment and support. 64
Only three studies were specifically on young people (15–39 years),22,33,34 with just one focusing on First Nations people. 48 Thus, limited studies have explored young people's experiences living with cancer in nonmetropolitan areas. The implications of limited evidence are that health care professionals in nonmetropolitan areas struggle to enhance service delivery in the absence of research to guide them. A further implication is that young people with cancer in nonmetropolitan areas cannot expect improvements in care given the limited understanding of their needs.
Many theoretical practice frameworks in helping fields are patient-centered.59,60 These approaches require asking about people's needs and preferences. 65 Attempts to improve care for young people living with cancer involves research strategies that ask young people themselves.66,67 Research exploring patient experiences where disadvantage, health inequalities, and knowledge gaps exist, can better inform practice.57,58,61 Current lack of research into young people living with cancer from nonmetropolitan areas, including First Nations people, seems reflective of barriers to care generally. Perhaps they are not being invited to participate in research as frequently as young people from metropolitan areas. Further research into health, psychosocial, and financial challenges over the course of a young person's cancer care trajectory, especially for First Nations young people, is required to better understand and care for nonmetropolitan young people.
Strengths and Limitations
This review fills a considerable gap in the literature on young people living with cancer from nonmetropolitan areas, and to our knowledge is the first to explore unique challenges experienced by young people living in nonmetropolitan areas. As models of care evolve, these data will be increasingly important to ensure gold-standard cancer care tailored to the needs of young people from a variety of demographic backgrounds including nonmetropolitan residency. Our findings must be considered in the context of several limitations.
We did not quality assess the articles and acknowledge that some of the study sample sizes were small. Furthermore, given that eight studies originated from Australia, conclusions regarding issues young people living in nonmetropolitan regions experience are most applicable to the Australian context.
The current overrepresentation of Australian research in the literature focusing on the experiences of nonmetropolitan cancer patients/survivors reflects the fact that as a country with the third lowest population density in the world, 49 Australia has led the field in this area. Other countries might have further layers of psychosocial complexity to consider in meeting needs of young people from nonmetropolitan areas. For example, financial distress reflected in this review may be even worse in countries such as the United States where young people may not have access to subsidized health care. Some studies68,69 have addressed financial distress impacts on young people living with cancer in the United States, but these were not in conjunction with nonmetropolitan experiences thus not captured in this study.
Our results indicate a gap in understanding the needs of nonmetropolitan dwelling young people living with cancer that researchers across the world need to address. Finally, only three studies were exclusively on participants within the age range of 15–39 years. However, given the paucity of published research on young people with cancer from nonmetropolitan areas, we included studies with broader age ranges that had young people in the participant pool given they addressed issues experienced living in nonmetropolitan areas for those with cancer.
Conclusion
Young people living with cancer in nonmetropolitan areas experience greater risk of health, psychosocial and financial problems compared with those from metropolitan areas. These problems are heightened during times of major transitions at diagnosis, during, and after treatment. Distance from specialist cancer care services was the central issue affecting all the challenges young people faced, with delayed diagnoses, reluctance to report symptoms or accept allied health referrals, separation from families, and financial distress being major risks identified. Future work investigating ways to minimize diagnosis delays, symptom reporting or accepting allied health referrals, psychosocial upheaval, financial distress, and issues particular to First Nations young people will be critical in developing age-appropriate services to meet unique needs of young people living with cancer from nonmetropolitan areas.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
This literature review was partially sponsored through a Scholarship for J.A.S. from Services for Rural and Remote Allied Health (SARRAH). U.S.-D. is supported by an Early Career Fellowship from the Cancer Institute of New South Wales (ID: 14/ECF/1–11) and an Early Career Fellowship from the NHMRC, Australia (APP1111800). The Behavioural Sciences Unit is proudly supported by the Kids with Cancer Foundation and by the Kids Cancer Alliance and a Cancer Council New South Wales Program Grant PG16–02 with the support of the Estate of the Late Harry McPaul.