
Abstract
Purpose:
This study evaluated the long-term psychological impact of childhood cancer and also sought to identify the risk factors in the development of psychological issues.
Methods:
Young adult (18–38 years) survivors of a childhood cancer (except leukemia), diagnosed younger than 15 years between 1987 and 1999 in the Rhône-Alpes region of France, were invited to a semistandardized psychological interview after a medical follow-up consultation during two successive long-term follow-up studies in Oncology (SALTO-1 and -2). Psychiatric issues from the DSM-IV were diagnosed and compared with the general French population (GFP) through interviews based on the Mini-International Neuropsychiatric Interview (MINI).
Results:
Of the 288 childhood cancer survivors (CCSs) who attended the consultations, 247 completed the MINI interview. Fifty-five percent indicated they had suffered from psychiatric issues after their cancer compared to 31.9% of the GFP (p < 0.0001). These issues were generally anxiety problems (40.5%), mood disorders (28.7%), and substance dependency (10.5%; p < 0.0001). The risk of suicide was, however, less for the CCS group (8.9% vs. 13.6%, p = 0.03). Unemployment was a significant risk factor for mood disorders (p = 0.009). Men were 4.1 times more likely than women to be addicted during their lifetime (p = 0.0004), while adults cured of bone tumors were 14.3 times more likely to be at risk of drug dependence than adults cured of central nervous system tumors (p = 0.01).
Conclusion:
CCSs are particularly vulnerable to psychiatric disorders throughout their life. Systematic and long-term psychological monitoring of these patients will enable their psychiatric issues to be detected sooner.
Introduction
In developed countries, the overall 5-year survival rate for pediatric cancers currently exceeds 80%. 1 Treatments have evolved to optimize the therapeutic strategies with the goal of limiting long-term physical complications. It is essential to evaluate the short- and long-term psychological complications resulting from childhood cancer to optimize the psychological care of patients currently treated. Untreated psychological disorders in childhood cancer survivors (CCSs) may have long-term consequences.2,3
The long-term follow-up studies in oncology (SALTO-1 and -2), conducted from 2011 to 2018, investigated particularly the psychological development of adult survivors of a pediatric cancer (excluding leukemia) diagnosed between 1987 and 1999, while residing in the Rhône-Alpes region (France).4,5 Our hypothesis in SALTO was that, since the care management of children with cancer in the past was not optimal, this would then result in post-cancer psychological disorders, reflecting a lack of prevention and monitoring of these disorders. The findings on this subject are somewhat controversial as some studies6–8 report that most adult CCSs do not report any particular psychological disorder, while other studies4,9 suggest that psychiatric disorders are significantly more prevalent. Indeed, previous studies have highlighted some risk factors for psychological disorders such as female gender, unemployment, and health problems.6,7,10 However, there are currently little data available on substance addictions among CCSs.
The main objective of this study was to verify, in the SALTO-2 population, the results of SALTO-1, which showed that adult CCSs were at greater risk of long-term psychological vulnerability than the general population (the prevalence rate of psychiatric disorders among the CCSs was 56.2%). 4 The secondary objectives were to analyze the overall population SALTO (1 + 2) and the specific risk factors that lead adult CCSs to develop psychiatric disorders.
Materials and Methods
Population
The SALTO cohort comes from the population-based Childhood Cancer Registry in the Rhône-Alpes Region (ARCERRA), which includes cases of tumors and leukemia, according to the third revision of the International Classification of Childhood Cancer (ICCC-3), 11 which have occurred since 1987 in children younger than 15 years living in the Rhône-Alpes region, 12 which covers 43,698 km2 (nearly 8% of the French territory) and contained around 6.3 million inhabitants in 2012 (nearly 10% of the French population), at the time of the SALTO studies. 13
Recruitment of participants and inclusion criteria were similar in the two successive SALTO studies. 5 To be eligible for SALTO-1 (conducted from 2011 to 2014) 5 or SALTO-2 (conducted from 2016 to 2018), subjects had to be diagnosed during, respectively, 1987–1992 or 1993–1999, and older than 18 years on December 31st, 2010 or June 1st, 2016, respectively. Patients diagnosed with leukemia were excluded from the research because this type of cancer was assessed in another French long-term follow-up study. After consulting the ARCERRA Registry, 1056 CCSs were found to be eligible for these multicenter prospective studies (including the Grenoble, Saint-Etienne, and Lyon pediatric oncology departments—The Clermont-Ferrand pediatric oncology department participated only in SALTO-1, with 14 Mini-International Neuropsychiatric Interview [MINI] respondents). 5 Patients were considered lost to follow-up if the vital status was unknown after checking with the French National Directory of Identification of Individuals (RNIPP), maintained by the French National Institute of Statistics and Economic Studies (INSEE), or if the address was unknown at the time of the study after checking with the French National Health Insurance Fund.
Method and evaluation
Eligible CCSs received a letter requesting their participation in the study. One month later, a letter of reminder had been sent to nonrespondents. CCSs who agreed to participate in the study received a “pre-consultation” questionnaire at home, which investigated several different domains (socioprofessional life, quality of life by SF-36v2™, 14 quality of sex life, health, and fertility). Thereafter, a pediatric oncologist, in association with an internist, made an appointment with the CCSs to deliver a long-term update on their condition and the treatments that the CCSs had received. This medical consultation was followed by a semistandardized psychological interview consisting of three distinct steps: (1) MINI questionnaire 15 ; (2) complementary psychometric tests based on the results of their self-questionnaires for all the participants, regardless of their responses to the MINI questionnaire (these tests assessed the participants' levels of self-esteem, anxiety, and depression, as well as their use of alcohol, tobacco, and cannabis); and (3) a psychological interview focused on the impact of cancer on the course of their future life.
The MINI was conducted by trained clinicians and explored, in a standardized way, the major Axis I DSM-IV psychiatric problems (mood disorders, anxiety disorders, addiction, psychotic disorders, and eating disorders—both past and present). To ensure the reliability of this multicenter study and to limit bias, the psychologists from each center met up before beginning the interview process to standardize and centralize the data (e.g., when a disorder was recorded as being present “at the time of the study,” it was also recorded as being present throughout the subject's “Entire life,” since by definition, the subject's entire life also includes the time of the study). We studied the risk factors for the three main types of emerging psychiatric disorders among adult CCSs: anxiety disorders (panic attacks, agoraphobia, social phobia, obsessive compulsive disorder, post-traumatic stress disorder, and generalized anxiety disorder), mood disorders (major depressive melancholia, dysthymia, and mania/hypomania), and addictive disorders (abuse and dependence on alcohol or substances such as cocaine, opiates, and cannabinoids).
Statistical analysis
The data were computerized using the EpiData software (EpiData version 3.1; The EpiData Association, Odense, Denmark) and analyzed using SAS software (SAS version 9.2; SAS Institute, Inc., Cary, NC).
The prevalence of psychiatric disorders among the survivors was compared to that of the general French population (GFP) of the same age and gender using the MINI questionnaire data with a nonparametric Fisher's exact test.16,17 Chi-square test was used to determine the characteristics of the MINI respondents compared to the nonrespondents among the contacted CCSs and to analyze the relationship between psychiatric disorders and risk factors, in particular, those related to disease (type of cancer, treatment, age at diagnosis, …) or environmental risk factors (occupational activity, marital status, psychological follow-up, overall health, …). When the conditions of Chi-square test were not met (theoretical number ≤5), the Fischer's exact test was applied. Risk factors that were significantly related to psychiatric disorders in univariate analysis (p ≤ 0.1) were then subjected to a multivariate analysis using a logistic regression model. The threshold for statistical significance was set at p < 0.05.
Ethics committee approval
Volunteers participating in the study were kept fully informed of the aims of the research and gave their informed consent to be included in the study. The ethical research committee Sud-Est I approved the study on December 7, 2015 (number clinical trials NCT 02675166).
Results
Results of the SALTO-1 study are presented in the publication of Bagur et al. 4 Of the 573 CCSs eligible for the SALTO-2 study, 117 responded to the MINI, representing 24.5% of the 478 CCSs contacted (Fig. 1), with a median age of 26.8 years (18.6–38.6) and a median time since diagnosis of 20.1 years (16.5–24.5). Some medical consultation participants (15%) did not benefit from the psychological survey for many reasons (lack of time, change of mind, planning difficulties, …).

Status of SALTO (1 + 2) participants and nonparticipants. SALTO, long-term follow-up studies in oncology.
Characteristics of the SALTO-2 MINI respondents
Among the 221 women contacted, 68 responded to the questionnaire (30.8%), while only 49 of the 257 men responded (19.1%, p = 0.003) (Table 1). Those patients who had been treated for bone tumors or Burkitt lymphoma had the highest participation rate with 51.7% and 36.1% participating, respectively (p = 0.0004). The type of treatment, age at diagnosis, age at the time of assessment, and the consultation center had no significant influence on the participation rate in the MINI interview. Participants who were teenagers when diagnosed (12–15 years) were more likely to participate in the study than the others (32%).
Characteristics of the Long-Term Follow-Up Studies in Oncology-2 Population Group Participating in the Mini-International Neuropsychiatric Interview Questionnaire
Agreement to complete a questionnaire and/or come to a medical consultation and/or meet the psychologist.
Calculated p value in the population of contacted CCS (n = 478).
CCS, childhood cancer survivor; CT, chemotherapy; MINI, Mini-International Neuropsychiatric Interview; NS, not significant; RT, radiotherapy; TBI, total body irradiation.
SALTO-2 compared to GFP
Of the 117 MINI respondents, 54.7% reported having developed at least one psychiatric disorder since the diagnosis of their cancer compared to 31.9% in GFP (p < 0.0001), and 36 of them (30.8%) were still suffering from a psychiatric disorder at the time of the study (Table 2). Anxiety disorders were most prevalent, with 41.9% of participants having developed at least one anxiety disorder in their lifetime compared with only 24.8% in GFP (p < 0.0001). These disorders were mainly generalized anxiety disorders (n = 32; 27.4%), followed by agoraphobia (n = 19; 16.2%), social phobia (n = 17; 14.5%), and panic attacks (n = 13; 11.1%). Agoraphobia was also significantly more likely to be present at the time of the study among adults having been treated for childhood cancers than in the GFP (n = 11; 9.4%; p < 0.0001). Of the 117 participants, 35 (29.9%) reported having developed at least one mood disorder during their lifetime, twice as many as in the GFP (14.9%; p < 0.0001). These mood disorders were almost exclusively major depressive episodes (MDE; 29.9%). SALTO-2 participants were also significantly more likely to develop substance dependence than the GFP (12% vs. 2.5%; p < 0.0001).
Comparison of Psychiatric Disorders at Any Time of Life and at Time of Study Between the Long-Term Follow-Up Studies in Oncology (1 + 2) Population and the General French Population Between 18 and 40 Years of Age
GAD, general anxiety disorder; GFP, general French population; MDD, major depressive disorder; OCD, obsessive compulsive disorder; PTSD, post-traumatic stress disorder; SALTO, long-term follow-up studies in oncology.
SALTO (1 + 2) compared to GFP
There was a significant preponderance of psychiatric disorders over the lifetime of adult CCSs compared to the GFP (55.5% vs. 31.9%; p < 0.0001) (Table 2). Anxiety disorders (40.5%), mood disorders (28.7%), and substance abuse/dependence (10.5%) were also significantly more prevalent in adult CCSs (p < 0.0001). At the time of the study, 82 of the 247 MINI participants (33.2%) reported persistent psychiatric disorders, mainly generalized anxiety disorder (10.9%, p = NS), followed by agoraphobia (7.3%, p < 0.0001), MDE (7.3%, p = NS), and then social phobia (6.5%, p = 0.08). Suicidal risk was significantly lower among the SALTO-2 participants (8.9%) compared to the GFP (13.6%, p = 0.03).
Risk factors from the SALTO (1 + 2) overall population
Table 3 shows the univariate analysis of the relationship between the three main groups of psychiatric disorders (anxiety disorders, mood disorders, and dependence) throughout the subjects' entire life and certain risk factors related to the disease or way of life at the time of the study. CCSs with a mood disorder or an anxiety disorder, who received psychological counseling (past or current), represented 46.5% (p < 0.0001) and 52.3% (p = 0.006), respectively. Unemployed people were significantly more at risk of mood disorders (44%, p = 0.01) as were those participants treated for a childhood bone tumor (47.8%; p = 0.03) and those 30–38 years of age (35.3%; p = 0.03). Men were more at risk of addictive disorders than women (26.7% vs. 9.2%, p = 0.0003), while the type of cancer also had an influence on the occurrence of substance abuse/dependence, with CCSs who suffered from Burkitt lymphoma (36.8%) or a bone tumor (34.8%) most at risk of addiction to substances (p = 0.003).
Univariate Analysis of Risk Factors for Psychiatric Disorders in the Long-Term Follow-Up Studies in Oncology (1 + 2) Population (247 Patients)
Bold indicates p < 0.05.
Multivariate analysis (Table 4) showed that unemployment was a significant risk factor for mood disorders (p = 0.009). Those CCSs with mood disorders were four times more likely to have needed psychological support than CCSs without these disorders (p < 0.001). Notably, men were 4.1 times more likely than women to be addicted during their lifetime (p = 0.0004), while adults cured of bone tumors were 14.3 times more likely to be at risk of drug dependence than adults cured of central nervous system tumors (p = 0.01).
Multivariate Analysis of Risk Factors for Mood and Dependency Disorders Among 247 Mini-International Neuropsychiatric Interview Respondents in Long-Term Follow-Up Studies in Oncology (1 + 2)
CI, confidence interval; OR, odds ratio; Ref., reference.
Discussion
SALTO-2 included the same reference population as SALTO-14,5 and a cohort of CCSs in the same age group (18–38 years), thereby allowing the final data of both studies to be compared. The results of these two successive studies were concordant and showed the greater long-term psychological vulnerability of adult CCSs compared to the GFP. As the method of recruiting patients, the diagnostic tools used (MINI), and the GFP were very similar in the two studies, combining their results enabled us to increase the statistical power, accuracy, and analysis.
One of the strengths of the study was the use of the MINI interview, which was used to assess psychiatric disorders in a standardized way, and which also provided better objectivity than self-questionnaires. Semidirected questionnaires allowed limiting the memory bias. Previous studies7,18,19 found that there was, in general, less psychological distress among adult CCSs than in the GFP, but were also in agreement on the fact that some survivor subgroups were more at risk of psychological problems. However, it should be noted that all previous studies had exclusively used self-questionnaires (notably the Brief Symptom Inventory).6,7,10 At the same time, another study using the MINI interview on a group of adult CCSs in France 9 found a greater proportion of mood disorders and anxiety disorders among these former patients compared to the general population. It should be noted that leukemias were excluded from the study, but according to the literature, the long-term psychological consequences are comparable to other types of cancer. Gandemer et al. 20 and Berbis et al. 21 showed that a long-term subgroup of survivors can benefit from a psychological assessment and targeted intervention because of the psychological impact of the disease.
In SALTO-2, CCSs who were sick during adolescence had the highest participation rate (30–38 years old today). It is likely that the onset of cancer in adolescence causes greater trauma than at any other time in life because it is a critical phase in psychobehavioral development. Some longitudinal studies have shown that untreated distress in adolescence can have long-term consequences. 22 The study highlighted the importance of anxiety disorders that can be considered residues of traumatic experiences due to cancer, possibly because the CCSs experienced social isolation when the disease was diagnosed and consequently experienced difficulty in developing social relationships that might explain the emergence of disorders such as agoraphobia or social phobia. In addition, the experience of being diagnosed with cancer generates major anxiety for the patient who is often heightened by the anxiety of the patient's family. 23 It was also found that mood disorders are very common among adult CCSs, a result that is broadly in line with previously recorded data and research.24–26
Adults treated for bone tumors as children were significantly more likely to be at risk of substance abuse/dependence. As this type of cancer can be very painful, we can hypothesize that the administration of opioids during childhood could induce a greater long-term vulnerability to the risk of addiction. Peck et al. 27 have shown that undertreated pain or major anxiety during the illness can lead to opioid abuse in the drive to feel a sense of “well-being.” It is possible that, even a long time after their cancer, and in a context of persistent anxiety, the CCSs seek this sensation again by consuming opiates in particular. This addictive behavior could also be a way of maintaining control over their lives by voluntarily exposing themselves to a risk as suggested by previous studies. 28
Even if CCSs do have significantly more psychological disorders than GFP, it has not been proven that this is directly due to their cancer. In accordance with the results reported by Mertens et al., 29 adult CCSs do not have an excessively high rate of mortality by suicide. Indeed, De Laage et al. 9 stated that they actually had less suicidal thoughts than the GFP. Since former patients are often defined as “survivors,” we can assume that they refuse to consider suicide, although they are sometimes found to have serious psychological issues.
Prevention can thus be identified as the key aspect of the management and treatment of these younger patients in the drive to minimize the psychological issues of the patients, with important roles for both relatives and health professionals.6,30 Since it does not seem possible to identify a certain population more at risk of developing psychiatric disorders, it is essential to target all of the CCSs by putting in place preventative measures as soon as cancer is diagnosed, as recommended by some clinical guides. 31 Coughtrey et al. 32 have shown the positive impact of psychosocial interventions in children with cancer. The temporality between the physical and psychic well-being of the patient is not the same. It is possible that the trauma caused by cancer cannot be treated by psychotherapy simultaneously with the physical treatment of the disease, but that psychotherapy treatments become more beneficial and necessary later on, especially at the onset of psychological distress symptoms. The simultaneous use of nonmedicated forms of stress management and cancer treatment is, however, a possibility.
A way of preventing this onset would be to make parents aware that their child is likely to have some long-term psychological symptoms (anxiety, mood disorders, or other issues). The family environment plays an important role in the psychosocial outcome of patients.33,34 They must know that they can receive psychological support for their child even after remission if necessary. Oncologists and general practitioners who follow these CCSs over the long term should be made aware of the greater psychological vulnerability of this patient population. As such, at the end of this work, we propose a brief questionnaire designed to help practitioners to identify early major psychiatric disorders (anxiety, depression, and addictions) in adult CCSs to guide them, with their agreement of course, toward obtaining suitable psychological care and treatment (Fig. 2).
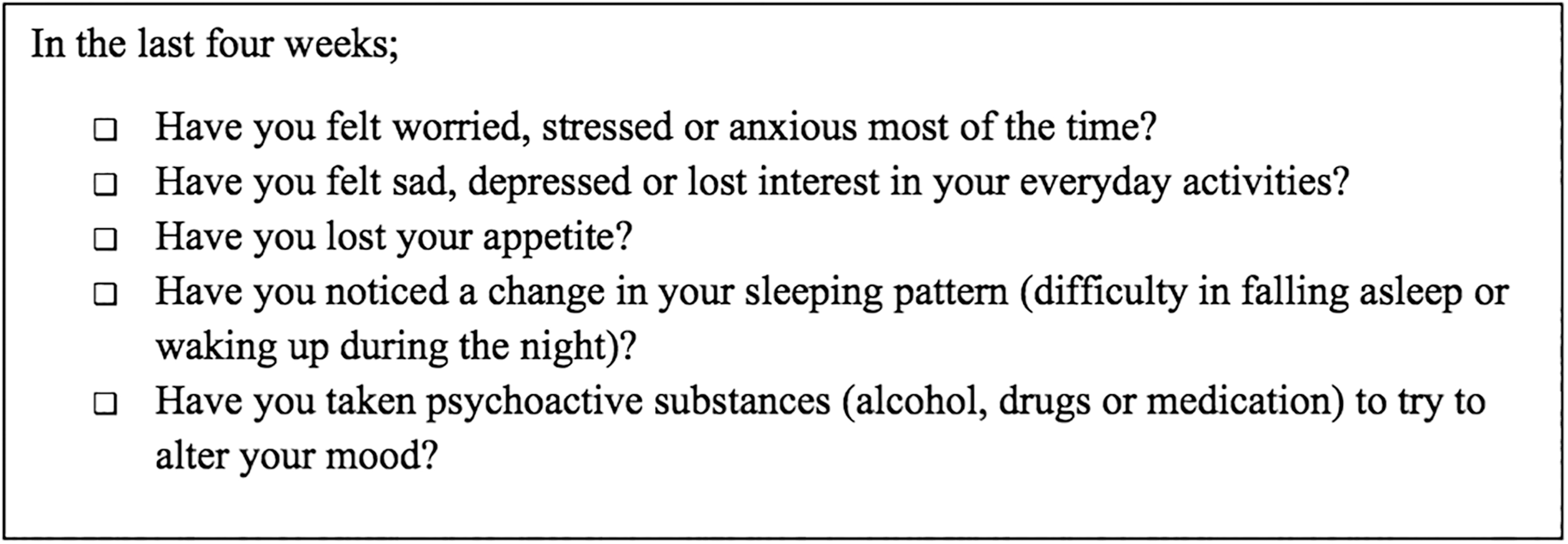
Quick outline of the major psychiatric issues arising from childhood cancer treatment.
However, it should be noted that the reference population is from 2009 as it was not possible to have more recent data using the Mini evaluation tool. This is a limit to our study and must be taken into account so as not to overestimate our results. We must also take into account a potential selection bias. Indeed, nonrespondents may be experiencing depression or anxiety that prevents them from participating.
Conclusion
In line with our initial hypothesis, young adults cured of childhood cancer develop significantly more psychiatric disorders than the GFP. This manifests mainly as anxiety disorders, mood disorders, and substance dependence/abuse several years after the cancer diagnosis. Certain risk factors have been identified for each of these disorders, including the gender of the patient (with males being more at risk of developing psychological issues) or a history of bone tumors for addictive disorders. Unemployment is associated with the occurrence of mood disorders.
In addition to a somatic plan monitoring the remission of pediatric cancer, it would be useful to also plan a long-term psychological follow-up of these patients. SALTO-2 has enabled us to identify the occurrence of disorders without precisely identifying when those disorders began. The main purpose of the study was to establish an overview of the patients' psychological state across their whole life as well as at the time of the study. It would therefore be interesting to undertake a new group study by proposing regular psychological interviews to analyze the resilience processes and identify those periods where the CCSs are most at risk in the emergence of psychological disorders.
Footnotes
Acknowledgments
We would like to thank all the former patients who agreed to participate in the SALTO-2 study. We would also like to thank the following people for their collaboration and contributions: the oncologists, Prof. Jean-Louis Stephan, Prof. Dominique Plantaz, Prof. François Déméocq, Dr. Nadège Corradini, Dr. Eliane Tarral, and Dr. Corinne Armari-Alla; the internists, Prof. Isabelle Durieu, Dr. Isabelle Guichard, Dr. Safia Khenifer, and Dr. Catherine Le Quang; the psychologists, Chloé Do Nascimento, Valérie Saulnier, and Sophie Domaison; the Clinical Research Associates, Françoise Odier, Meredith Mercier, Pierre Métral, Sandrine Billet, Isabelle Schiff, Camille Celette, and Aurélie Chausset; our secretary, Audrey Loubier; and the translator, David Lewis.
Author Disclosure Statement
This research was not the subject of any competing financial interests.
Funding Information
We would like to thank The French League Against Cancer for its financial support.