
Abstract
Purpose:
With increasing number of childhood cancer survivors, focus has recently shifted to improving future quality of life and long-term complications, such as infertility. Despite national guidelines, fertility preservation is discussed in less than half of the eligible patients. In this study, we sought to discover if education gaps regarding fertility exist within our practice, in efforts to address these gaps to improve the quality of cancer care we provide.
Methods:
A retrospective electronic survey was administered to eligible adolescent and young adult oncology patients.
Results:
Of the 63 patients approached, 47 responded to the survey. Before initiation of antineoplastic therapy, 22/47 (46.8%) stated that they were concerned about their fertility to some degree; however, only 11/47 (23.4%) report pursuing fertility preservation. When asked why they decided against steps to preserve fertility, 15/36 (41.6%) reported that they did not know they had options. Of all patients that completed the survey, 28/47 (59.6%) requested additional information regarding their fertility.
Conclusion:
Majority of respondents recall having a discussion regarding the impact of antineoplastic therapy on their fertility at the time of diagnosis, which was initiated by their oncologist. However, less than half reported satisfaction with these discussions. Although this study did not demonstrate statistical significance, it has resulted in development of a multidisciplinary oncofertility team for fertility preservation referrals, at our institution, as well as education materials for all newly diagnosed oncology patients.
Introduction
The American Cancer Society (ACS) reports that, in 2019 in the United States, an estimated 10,590 new cases of cancer will be diagnosed among children aged 0–14 years. 1 In 2015, there was an estimated 429,000 survivors of childhood cancer in the United States. 2 With advances in early diagnosis and medical breakthroughs in cancer treatment, childhood cancer survival rates have significantly increased. 2 However, with such effective treatments comes the reality of treatment-related complications, such as impaired reproductive capacity, resulting in infertility. While some treatments have marginal effect on reproductive health, others have the potential to result in permanent infertility.
Chemotherapy and radiation, which comprise many treatment regimens used to successfully cure a variety of childhood cancers, are well known to inflict damage to reproductive organs and germ cells, resulting in impaired fertility and ability to conceive a child. 3 For those patients who do get pregnant, the risk of maternal and offspring complications increases. These complications include gestational diabetes, hypertension, pre-eclampsia, postpartum hemorrhage, premature birth, low birth weight, intrauterine growth restriction, and need for resuscitation at the time of delivery.4–7 With this, the field of “oncofertility” has emerged to integrate oncology and reproductive research to provide an improved quality of life and fulfillment for cancer survivors, leading to the development of the oncofertility consortium (OC) in 2007.
The Children's Oncology Group (COG), American Society of Transplantation and Cellular Therapies (ASTCT), American Society of Clinical Oncology (ASCO), American Society of Reproductive Medicine (ASRM), and National Comprehensive Cancer Network (NCCN) adolescent and young adult (AYA) oncology guidelines have recommended that the impact of cancer treatments on fertility be addressed with all cancer patients of reproductive age before the start of therapy, and that options for fertility preservation be discussed routinely.8,9
Despite the emergence of this field, the development of guidelines, and the interest of patients in preserving fertility, data suggest that fertility preservation referral rates remain low.10–13 We recognize the importance of quality of life in our childhood cancer survivors and the role fertility plays in their overall well-being. A recent report from the Pediatric Initiative Network of the OC states that not only do fertility preservation rates increase after the establishment of a formal fertility preservation program but also patient satisfaction. 14 This concept is echoed in other studies across the United States.15,16
Therefore, as our institution currently does not have formal fertility preservation practices, we conducted a study to address if an education gap exists among our practice, in efforts to improve the quality of cancer care we provide.
Design/Methods
Participants and data collection
This was a single-institution cohort study utilizing a convenience sample and survey methodology that was approved by the Institutional Review Board (IRB) at Akron Children's Hospital (ACH), in Akron, Ohio. The study was conducted from February 1, 2018 to December 31, 2018.
A 10-question retrospective electronic survey (Table 1) was developed to address three domains: (1) whether the impact of antineoplastic therapy, both chemotherapy and radiation (cranial and/or pelvic), on patient's fertility was discussed before, during, or after treatment; (2) whether fertility services, such as oocyte/sperm cryopreservation or ovarian suppression, were offered; and (3) satisfaction of the patient's fertility knowledge. We predicted that a discussion will have been had in <75% of patients, fertility services will have been pursued in <20% of patients, primarily due to the financial cost of preservation, and that patients will not be satisfied with their knowledge of fertility. These predictions were based on similar studies in the literature.17–20 The number of survey questions was limited to 10 based on previous experience of surveys conducted in our department at our institution, with longer surveys resulting in poor compliance as well incomplete responses.
Survey Questions and Responses
Patients eligible to complete the survey included those who were >12 years of age at the time of cancer diagnosis and were 6 months–5 years postcompletion of antineoplastic therapy. Patients with antineoplastic therapy lasting >3 years, who were in the maintenance phase of therapy, were also included. Patient's cognitive ability must be considered by a parent or health care professional to be at least at a 4th-grade level for study participation, per the recommendations of our patient education services; though a formal tool was not used to assess this. All cancer diagnoses were eligible for participation.
To allow Spanish-speaking patients to participate, bilingual health services in the form of in-person interpreter and translated survey in Spanish were provided. For our Spanish-speaking patients, the survey was to be administered on paper versus electronic tablet. In addition, due to the inability to obtain a translated survey in other languages, non-English- or non-Spanish-speaking patients were not eligible to participate. Survey questions were reviewed by our patient education services to ensure appropriate language for the survey population. Patients who were diagnosed at an institution other than ACH were excluded, as well as those with relapsed disease.
All patients scheduled for a provider or nurse appointment at the ACH Hematology Oncology outpatient clinics were assessed for eligibility before arrival. This was conducted by reviewing each individual patient's medical record. If patients were deemed eligible, they were approached regarding their participation in the study. After obtaining a signed written consent and/or assent, patients were provided the survey on an electronic tablet, to complete during the clinic visit, which was then collected upon completion.
Statistical analysis
Examination of data included calculation of full summary statistics for age, as well as calculation of frequencies and percentages for categorical and Likert-type survey data. Primary analysis was descriptive, followed by an exploratory analysis utilizing Fisher's exact test and Cochran-Armitage trend test to evaluate potential associations between patient characteristics and survey responses. Statistical analyses were completed using SAS 9.4/14.2©. Unless otherwise noted, all testing was two tailed and evaluated at the Type I error rate of α = 0.05 level of statistical significance.
Results
Demographics and patient characteristics
Over the 11 months span of the study, 118 patients were scheduled for a clinic visit and reviewed for eligibility. Sixty-three patients were deemed eligible and approached to participate in the study. Of the 63 patients approached, 38 (60.3%) were male and 25 (39.7%) were female. Mean (standard deviation) age in years was 15.0 (2.1), with a range of 12–20. Although patients were eligible for participation up to 5 years postcompletion of antineoplastic therapy, the average time was 20 months postcompletion of therapy, with the longest being 29 months. Cancer types included leukemia (B-cell and T-cell acute lymphoblastic leukemia [ALL], acute myeloid leukemia [AML], and chronic myeloid leukemia), central nervous system tumors (craniopharyngioma, ependymoma, medulloblastoma, and pilocytic astrocytoma), sarcoma (Ewing sarcoma, osteosarcoma, rhabdomyosarcoma), carcinoma (nasopharyngeal carcinoma), and lymphoma (Hodgkin's lymphoma and non-Hodgkin's lymphoma). Patients had received either chemotherapy alone, cranial or pelvic radiation, or a combination of both chemotherapy and radiation. All patient characteristics for survey respondents are summarized in Table 2.
Patient Demographics and Clinical Characteristics
Recall and services
Of the 63 patients approached, 47 responded to the survey for a response rate of 74.6%. Of the 12 patients who refused to participate, 8 were male and 4 were female. Reasons for declining participation included additional time commitment (n = 11) and parent refusal (n = 1). The most common cancer diagnosis was ALL (11; 23.4%), followed by Hodgkin's lymphoma (9; 19.1%), Ewing sarcoma (6; 12.8%), osteosarcoma (5; 10.6%), and AML (5; 10.6%). Other cancer types accounted for <5%.
In regard to pre-treatment level of concern, 22 (46.8%) patients stated that they were concerned about their risk of infertility to some degree, with an equal distribution among males and females. Thirty-five (74.5%) patients recalled having a discussion, regarding the impact of antineoplastic therapy on their fertility, happening at the time of diagnosis; with these discussions initiated by the physician in ∼85% of the cases. However, only 11 (23.4%) patients reported pursuing fertility preservation services; with 4 (8.5%) unable to recall. These services included sperm banking (n = 7), oocyte cryopreservation (n = 1), injections for ovarian suppression (n = 3), and general consultation with a reproductive gynecologist (n = 1). This was confirmed by reviewing the medical chart documentation as well as the database of patients who have pursued fertility preservation services. There was no evidence of a significant difference in age for those who did receive fertility services before or during treatment, as compared with those who did not [14.9 (2.2) years vs. 16.2 (1.3) years (Wilcoxon Rank Sum Test with Exact Option, p-value = 0.05)]. Results of the Cochran-Armitage trend test provide no evidence of a significant trend for having a discussion when first diagnosed about the effect of treatment on future fertility or interest in receiving additional information or receiving fertility services with pre-treatment level of concern that cancer treatment would cause infertility (p-value = 0.17 and 0.50, respectively).
The 36 patients who either did not pursue fertility services or did not recall were then asked why they decided against steps to preserve fertility. Fifteen (41.6%) patients stated that they did not know there were options, with an additional 8 (22.2%) patients choosing “other” as a reason. Of those 8, 4 (50%) stated that their parents, not they themselves, decided for them. Of all patients who completed the survey, 28 (59.6%) requested additional information regarding their fertility.
Discussion
For the AYA population, oncofertility, including discussion of risks to reproductive health, fertility, and fertility preservation options, should be an essential part of a comprehensive cancer treatment plan. 15 There have been numerous studies conducted among oncology providers showing inconsistent referrals for fertility preservation counseling before onset of cancer treatment. A survey of pediatric oncologists found that >90% agreed that patients should be offered fertility consultation; however, only 46% indicated that they refer male pubertal patients >50% of the time, and only 12% reported referring female pubertal patients >50% of the time. 21 The survey for preservation of adolescent reproduction (SPARE), administered to oncologists, advanced practice providers, and nurses, found that while 44% of respondents were familiar with the ASCO recommendations, only 39% of those utilized them to guide decision making in greater than half of their patients. 11
Similar surveys and studies, though limited, have been conducted among pediatric and AYA cancer patients in efforts to address execution of national guidelines. A study conducted across the United Kingdom and Europe found that 83.5% of males and 59.3% of females recalled having a discussion about fertility, with 55% reporting dissatisfaction with the information they received. 17 Similarly, in a pilot study conducted in Lurie Children's Hospital (Chicago, IL), it was found that 11 of 19 (58%) adolescent females recalled a discussion about infertility risk and 9 (47%) about fertility preservation. 18
The results of our study are quite similar to the above studies. When selecting patients for study participation, we primarily based this on the age of diagnosis, time from diagnosis, and whether they received any chemotherapy and/or radiation. We did not specifically look at details of their therapy when selecting patients. We understand that this will skew results as not all patients of reproductive age would require fertility preservation services. In our cohort, we found that 74.5% of patients recalled having a discussion, with a majority (85%) of these discussions being initiated by an oncologist, addressing one of the three questions we set out to answer. However, despite the availability of reproductive gynecology and infertility specialists, only 23.4% of patients recall pursuing fertility preservation services, and 40.4% stating satisfaction in their knowledge regarding their risk of infertility. The results regarding a discussion were confirmed with the medical record as providers would document therapy-related risks, including infertility, in their consent. Of the six patients who did not recall having a discussion, only one was confirmed through medical record to have had a discussion; though record bias cannot be ruled out.
As mentioned previously, our initial hypothesis regarding the lack of pursuing services involved cost, as fertility preservation services, especially for females, are expensive without support from charitable foundations. However, only 5.6% of those who did not pursue services or did not recall stated their reasoning to be expense. In fact, majority of the patients reported that they either did not know there were options or that their parents decided for them. These results suggest that oncofertility discussions should involve both the parent and adolescent patient. The news of a cancer diagnosis is in fact life changing and difficult to accept, therefore it is reasonable that such discussions may have been had with the adolescent patient simply being unable to recall. In addition, should the parents have been surveyed, the financial cost for preservation may truly have been a reason for not pursuing services. Given this, we acknowledge this as a weakness of our study, and aim for future such studies to include both the parent and adolescent patient for accuracy of results.
We recognize the importance of a formalized fertility preservation program and its impact on the overall quality of cancer care provided. The OC, which includes >100 institutions nationwide, has established over recent years that a formalized fertility preservation program leads to increased rates of fertility consultations, fertility preservation services, and patient satisfaction.14,16,22 In addition, regardless of whether preservation is pursued, a consultation itself leads to improved reproductive knowledge and informed decision making. 23
At our institution, this study has resulted in the development of a formalized fertility preservation program with a multidisciplinary oncofertility team dedicated to addressing every reproductive need of a patient undergoing antineoplastic therapy. Per the guidance of the OC and their literature on program building, our team will include physicians and advanced practice providers with a special interest in reproductive health and oncofertility.3,14 The primary goal of this team will be determining therapy-related infertility risk as well as developing a proposed plan of care to address risk of impaired fertility, including coordinating referrals to fertility specialist and procedures. Additional members will include reproductive gynecology and infertility specialists, urologist, social services, as well as a clinical navigator. Team members will undergo education training regarding the impact of antineoplastic therapy on reproductive health as well as approach to consultation and counseling. This will include the use of resources provided by the OC, such as Reprotopia, as well as attending education conferences held by members of the OC. Team members will also complete an online fertility preservation course provided by ASRM.
In addition, a standard operating procedure for fertility preservation referrals has been implemented in an attempt to capture all newly diagnosed oncology patients eligible for fertility preservation services (Fig. 1). Finally, per patient request, individualized education material in the form of a pamphlet has been created that will be provided to all newly diagnosed oncology patients. As for patients who have completed therapy, consultation will be available for those inquiring about their reproductive health or interested in additional information.
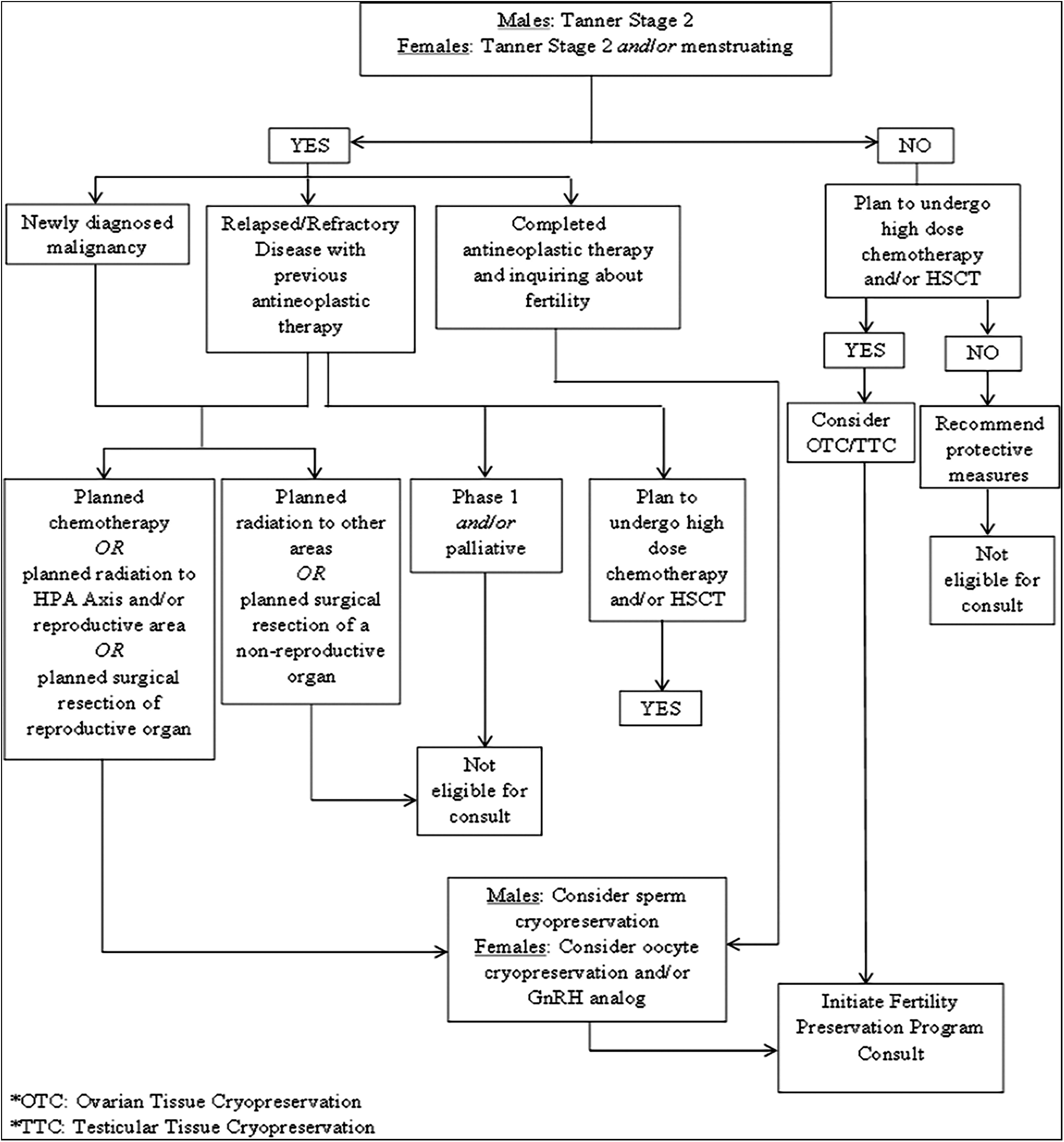
Fertility preservation referral process.
This survey was limited by its survey methodology, recall bias, and lack of parental involvement. Although there are many validated oncofertility surveys in adult breast cancer patients, a validated patient survey for the pediatric population is currently unavailable. Therefore, it is difficult to measure if the questions posed in our survey truly measure issues of importance. In addition, as mentioned previously, recall of adolescent patients can be limited and would the parents have been surveyed, this would have provided a stronger case of our results. Despite this, the study addresses an important gap in the education provided as well as insufficient communication with our AYA patients, suggesting the need for formalized fertility preservation programs at pediatric cancer centers to increase preservation rates as well as general reproductive health education.
Footnotes
Acknowledgments
We thank biostatistician, Neil L. McNinch, MS RN PSTAT®, for his contribution to this work. We also thank our patients, survivors, and caregivers for participation in the study, as well as our AYA program and committee for their support in conducting this survey. In addition, formal IRB approval was obtained as well as informed consent/assent for this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.