
Abstract
Purpose:
The French standard chemotherapy for osteosarcoma combines high-dose methotrexate (HDM) and etoposide–ifosfamide (EI) in children and adolescents, and API-AI (doxorubicin–cisplatin–ifosfamide) in adults. We herein present the results of M-EI and API-AI in 18- to 25-year-old patients.
Methods:
Patients, 18–25 years old, received either M-EI or API-AI regimens. M-EI comprised seven M and two EI doses preoperatively then M-EI in standard-risk patients (good histological response without metastasis) and five M-AP (methotrexate–doxorubicin–cisplatin) in high-risk patients (poor histological response, metastasis, and/or unresectable primary), postoperatively. API-AI comprised three API and two AI doses preoperatively, then two AI and two PI in standard-risk patients and five EI in high-risk patients, postoperatively.
Results:
We analyzed 95 patients 18–25 years of age: 55 received M-EI and 40 API-AI. The groups had similar baseline characteristics. Eighty-nine patients (94%) had surgery. Twenty-nine of 55 M-EI patients (60%) and 16/40 API-AI patients (41%) had good histological responses to preoperative chemotherapy. At 5 years, event-free survival was 50% (95% confidence interval [CI]: 39–60) and overall survival was 65% (95% CI: 54–74). Acute toxicity was similar, without treatment-related deaths.
Conclusions:
Survival outcomes with M-EI and API-AI were not significantly different. Tolerance was acceptable with both regimens. HDM is thus feasible for young adults. However, our study limitations preclude any definitive conclusions.
Background
Osteosarcoma occurs most often in children and young adults, and it is the most frequent malignant bone tumor in adolescent and young adults. 1 The standard treatment is chemotherapy with surgery. In the United States and most of Europe, the standard chemotherapy is the methotrexate, doxorubicin and cisplatin (MAP) regimen (high-dose methotrexate [HDM], doxorubicin, and cisplatin).2–5 However, in France, based on the randomized OS94 pediatric trial, the standard chemotherapy combines methotrexate and etoposide–ifosfamide (M-EI) in children and adolescents, whereas most adults are treated with doxorubicin–cisplatin–ifosfamide (API-AI) based on a phase II study performed by the French Sarcoma group.6–8 Postoperative chemotherapy is based on the histological response to the preoperative chemotherapy and the risk group. In patients treated with M-EI, postoperative doxorubicin and cisplatin are only administered to patients with metastases, a poor histological response, or an unresectable tumor. The M-EI protocol aims to limit the long-term side effects of doxorubicin and cisplatin in young patients who have a low risk of relapse: nonmetastatic with a good histological response. This approach proved feasible in the OS94 trial. 6
Whether adults should be treated by a pediatric approach or by specific protocols is still a matter of debate. Age is thought to impact prognosis, with a better prognosis in younger compared with older patients.9,10 This age effect is possibly due to biological differences, but may be related to limited clinical trial enrolment, as well as a lack of compliance and a poorer tolerance to chemotherapy in older patients. The tolerance to HDM in adults has been reported to be worse than in children and adolescents, although data concerning tolerance in young adults are limited, and the therapeutic superiority of HDM-containing regimens in this population is debatable.11,12
In the French OS2006 trial (NCT00470223), we assigned chemotherapy by age. Patients, 18–25 years old, received either M-EI or API-AI chemotherapy according to the predetermined choice at each center. In this article, we present the results for osteosarcoma patients, 18–25 years of age, enrolled in the OS2006 trial and treated with either M-EI or API-AI regimens.
Materials and Methods
Study design and participants
The French multicenter OS2006/Sarcome-09 study enrolled patients with localized or metastatic high-grade osteosarcoma younger than 50 years of age. This study included an open-label, phase III, randomized trial that evaluated zoledronate in combination with chemotherapy (Clinicaltrials.gov Registration No. NCT00470223). The patients who were not randomized could be enrolled in the OS2006 study (EudraCT No. 2006-00337727) and received chemotherapy without zoledronate. The OS2006 study was approved by a French Ethics Committee. All patients gave written informed consent before study participation. The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. Patients with newly diagnosed, biopsy-proven, high-grade osteosarcoma who had normal hematological, renal, cardiac, and hepatic function were eligible. All patients and/or their parents/guardians provided written informed consent before enrolment, even if the patient was not randomized.
Treatment and follow-up
In the OS2006 study, patients who were 18–25 years old received either the M-EI or the API-AI regimen. The regimen was predetermined at each center before the inclusion of the first patient in the trial. Younger patients (i.e., <18 years old) received M-EI and those older (i.e., >25 years old) received API-AI (Fig. 1). Preoperative M-EI was administered over a 13-week period and comprised seven cycles of M (HDM, 12 g/m2 no upper dose limit) and two cycles of EI (etoposide, 300 mg/m2; ifosfamide, 12 g/m2). While, preoperative API-AI was administered over a 15-week period and comprised three cycles of API (doxorubicin, 60 mg/m2; ifosfamide, 6 g/m2; and cisplatin, 100 mg/m2) and two cycles of AI (doxorubicin, 60 mg/m2; ifosfamide, 6 g/m2). After preoperative chemotherapy, patients underwent surgery of their primary tumor. This was followed by postoperative chemotherapy, assigned according to their risk factors: good or poor histological response to preoperative chemotherapy, presence of distant metastases, and resectability of primary tumor. A modified Huvos grading assessed the histological response: a good response being <10% viable cells. In the M-EI group, patients with a good histological response and no distant metastases (i.e., standard-risk patients) received 12 cycles of M and 3 cycles of EI (the last cycle was without etoposide). While patients in this group with a poor histological response, initial metastases and/or unresectable primary (i.e., high-risk patients) received five cycles of M and AP (doxorubicin, 75 mg/m2; cisplatin, 120 mg/m2). In the API-AI group, standard-risk patients received two cycles of AI alternating with two cycles of PI (cisplatin, 100 mg/m2; and ifosfamide, 6 g/m2), while high-risk patients received five cycles of EI (etoposide, 300 mg/m2; ifosfamide, 12 g/m2). The scheduled treatment duration varied according to the treatment allocated by risk factors: 37–38 weeks with M-EI and 31–34 weeks with API-AI.

The treatment regimens.
During the preoperative chemotherapy, the tumor response was assessed at weeks 7 and 14 by radiography and magnetic resonance imaging of the primary tumor site, and a chest X-ray (or a thoracic computed tomography scan for patients with initial lung nodules).
After the postoperative chemotherapy, chest X-rays were scheduled every 3 months for 3 years, then every 4 months for the following 2 years, and yearly thereafter. Yearly assessments of the primary tumor sites, by radiography, were recommended.
Endpoints
The baseline characteristics, treatment compliance, and efficacy were assessed in all patients enrolled in the M-EI and API-AI groups.
In the M-EI group, preoperative chemotherapy modifications were considered minor if the patient received ≥5 M cycles and 2 cycles, including etoposide, ifosfamide, or cyclophosphamide, with no other drug, and major in all other cases. Postoperative modifications were classified as minor if the patient received ≥8 M cycles and 2 cycles, including etoposide, ifosfamide, or cyclophosphamide, with no doxorubicin/cisplatin in the standard-risk strata and if the patient received ≥4 M cycles and 4 cycles of AP or doxorubicin–carboplatin in the high-risk strata. All other modifications were considered major.
In the API-AI group, preoperative chemotherapy modifications were considered minor if the patient received ≥4 API- or AI-cycles, or the equivalent (doxorubicin–cisplatin–cyclophosphamide, and doxorubicin–cyclophosphamide), with no other drug; and considered major in all other cases. Postoperative modifications were considered minor if the patient received ≥4 API- or AI-cycles, or equivalent (e.g., doxorubicin–cisplatin–cyclophosphamide or doxorubicin–cyclophosphamide) in the standard-risk strata and ≥4 EI-cycles or the equivalent (e.g., etoposide–cyclophosphamide) in the high-risk strata. All other modifications were considered major. 13 For randomized patients, the preoperative chemotherapy dose intensity was computed as published by Wampler and Fryer. 14
Data on toxicity, collected prospectively, is only available for patients included in the randomized trial. During chemotherapy, adverse events were assessed using the CTCAE (Common Terminology Criteria for Adverse Events) v3.0. Acute toxicity was analyzed using the highest grade observed during chemotherapy. All grade 4 hematological toxicities and grade 3/4 extrahematological toxicities were considered as severe.
Event-free survival (EFS) was defined as the interval between the start of preoperative chemotherapy and disease progression, relapse, secondary malignancy, or death from any cause, or until the last follow-up visit for patients in first complete remission. Overall survival was defined as the interval between initiating preoperative chemotherapy and death from any cause.
Statistical analysis
The baseline characteristics, treatment compliance, and safety data were compared between the two treatment groups (i.e., the M-EI vs. the API-AI group) using the Pearson chi-square or Fisher tests (qualitative variables), or Student's tests (continuous variables). The incidences of severe adverse events were compared using relative risk.
The EFS and overall survival were evaluated using the Kaplan–Meier method and compared using a log-rank test. To control for potential confounders, hazard ratios (HRs) were estimated in a multivariate model adjusted for age and initial disease stage (metastatic vs. localized).
To investigate the impact of age on survival outcomes, we assessed survival by age group in the OS2006 population: patients treated with M-EI (<18 years old vs. 18–25 years old) and those treated with API-AI (18–25 years old vs. >25 years old).
Estimates are provided with their 95% confidence intervals (CIs). All tests were two-sided and analyzed using SAS 9.4 software (SAS Institute, Inc., Cary, NC).
Results
The OS2006 study enrolled 522 patients between April 2007 and March 2014. Ninety-five of them were 18–25 years of age and they were enrolled in 26 centers: 55 in the M-EI group and 40 in the API-AI group (Fig. 2). The majority (i.e., 59/95 patients [62%]) participated in the zoledronate trial, of whom 36 (65%) were in the M-EI group and 23 (58%) were in the API-AI group.
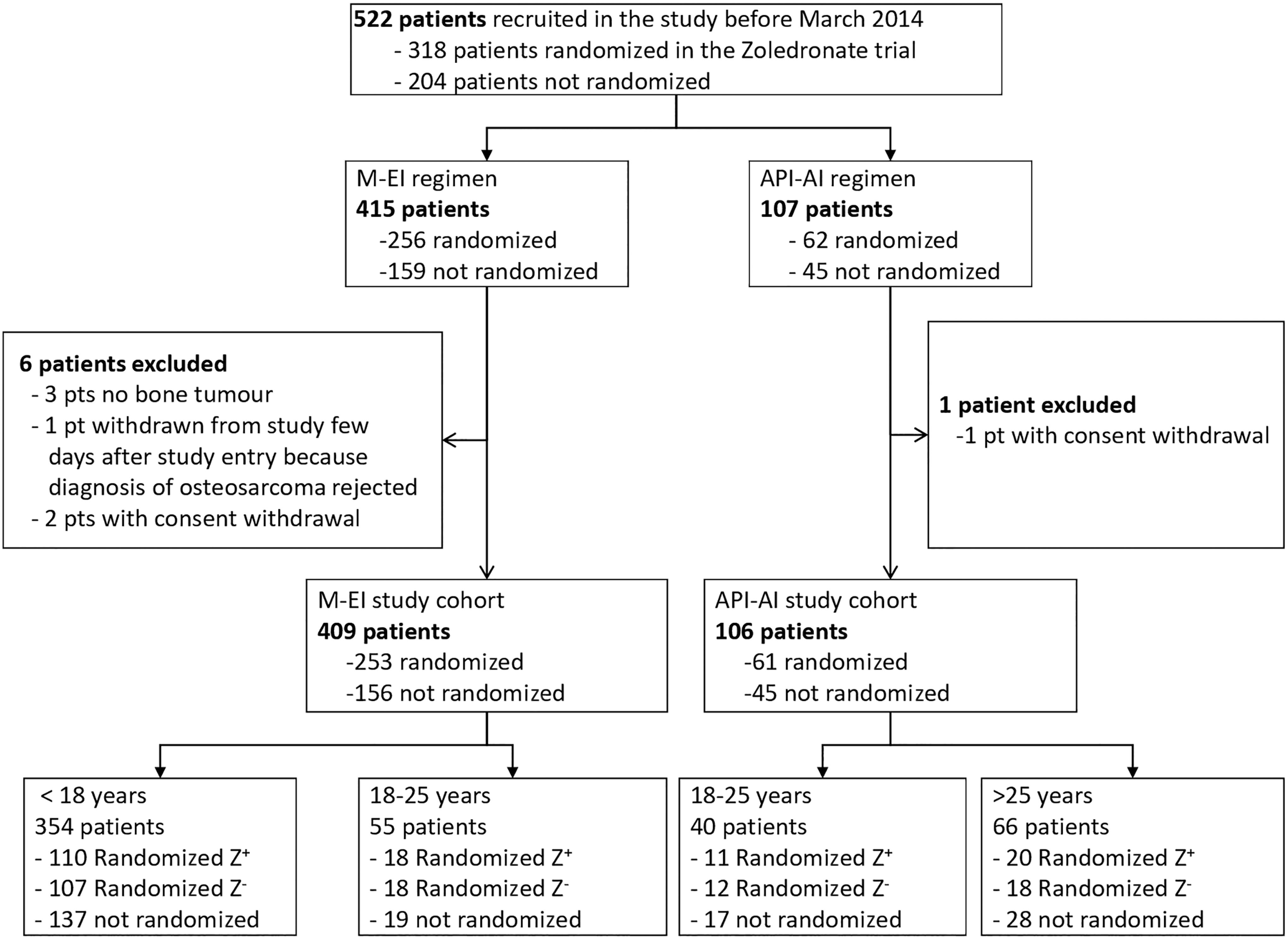
Participant flow chart of trial population.
Description of the population
The baseline demographic characteristics were similar for the two groups (Table 1). Median age was 20.1 years (interquartile range: 19.0–21.3) with a majority of males (65 patients [68%]). In terms of disease characteristics, most patients (87 patients [92%]) had the primary tumors located in the limbs. In addition, 22/95 patients (23%) had metastatic disease at baseline: 10/55 patients (18%) in the M-EI group and 12/40 (30%) in the API-AI group. We did not observe any significant differences in the baseline characteristics between the groups.
Baseline Demographic and Clinical Characteristics in the Overall Population and According to the Chemotherapy Regimen
Both cases where prior bilateral retinoblastoma; details are presented in Supplementary Table S1.
Lung metastases were considered definite if there was a lesion of at least 10 mm, two or more lesions ≥5 mm, or five or more lesions irrespective of the size.
Skip metastasis was defined as a bone lesion in the same bone as the primary tumor. Transarticular lesions were not counted as skip metastases, but as distant bone lesions.
Other histological types were one periosteal osteosarcoma; one well differentiated; one giant cell osteosarcoma, and one chondroblastic osteosarcoma.
API-AI, doxorubicin–cisplatin–ifosfamide; IQR, interquartile range; MD, missing data; M-EI, methotrexate and etoposide–ifosfamide.
Treatment
All but one of the patients started the predefined chemotherapy at the center (for details see Table 2). Major modifications of the preoperative treatment only occurred with M-EI, in 13/55 patients, due to toxicity (n = 8), suspected early progression (n = 4), or both (n = 1). The reasons for major modifications of preoperative treatment are tabulated in the Supplementary Table S1.
Description of Treatment in the Overall Population and According to the Chemotherapy Regimen
Test of the comparison of the proportion of patients enrolled in the randomized trial, p = 0.43. Test of the distribution across the three categories, p = 0.72; the randomized trial was stratified according to the chemotherapy regimen.
Test of the comparison of any treatment modification versus no modification, p = 0.15; test of the distribution across the three categories, p = 0.003.
Test of the distribution of conservative surgery versus amputation. Six patients were not included because surgery was not assessed.
The histological tumor response to preoperative chemotherapy could be evaluated in 87 patients who underwent surgery after preoperative chemotherapy; it was not evaluated in 6 patients who did not undergo surgery as part of their first-line treatment and in 2 patients who had the initial surgery at diagnosis.
Calculated only for the 86 patients who received postoperative chemotherapy.
Test of the comparison of major modification versus none or minor modification, p = 0.18; test of the distribution across the three categories, p = 0.06.
MRI, magnetic resonance imaging.
Five patients had no surgery after the initial chemotherapy: two M-EI patients with disease progression before surgery and three patients with unresectable tumors (two in the M-EI group and one in the API-AI, all of whom received radiotherapy). Furthermore, the local treatment data were missing for one patient, following early withdrawal of consent. Overall, 89 patients (94%) underwent surgery, with a median delay of 23 days after the chemotherapy. As we expected due to the different hematological toxicities associated with each regimen, the median length of time between the chemotherapy and surgery was significantly longer in API-AI group, 30 days, compared with the M-EI group, 14 days (p = 0.01). Surgery was conservative in 76 patients (85%). The histological response could be evaluated in 87 patients and it was rated as good in 45 patients (52%; 95% CI: 41–62): 29/48 patients (60%; 95% CI: 47–74) in the M-EI group and 16/39 patients (41%; 95% CI: 26–56) in the API-AI group (p = 0.07).
Overall, 86 patients started postoperative chemotherapy with a median delay of 22 days. Only 41/86 patients (48%) received postoperative treatment as per protocol. Major modifications of the postoperative treatment occurred in 20/49 (41%) patients in the M-EI group, and in 10/37 (27%) in the API-AI group (p = 0.18). Overall, 23/55 M-EI patients (42%), including 21/45 (47%) with localized disease, received neither doxorubicin nor cisplatin first-line treatment. As expected, the treatment duration was significantly different, with a median of 38.0 weeks with M-EI versus 32.4 with API-AI (p < 0.0001).
The treatment dose intensity was analyzed by age group for the OS2006 study subpopulation randomized in the phase III trial evaluating zoledronate combined with chemotherapy. 8 With M-EI, we observed a significantly lower dose intensity in the patients who were 18–25 years old compared with the patients who were less than 18 years old (p = 0.002). In contrast, no significant difference was observed between patients who were 18–25 years old and those over 25 years of age when they were treated with API-AI (p = 0.13).
The median duration of M-EI treatment was 5 weeks longer than with API-AI. Consequently, the hospitalization for chemotherapy was longer in the M-EI group (101 days for the patients with a good histological response and 73 days for those with a poor response) compared with the duration of the hospitalization for the API-AI group (32 days for the patients with a good histological response and 38 days for those with a poor response).
Safety
No treatment-related deaths were reported. The 58 patients randomized in the phase III study were assessed for safety: 35 treated with M-EI and 23 with API-AI. The results are shown in Figure 3 (for details see the Supplementary Table S2).
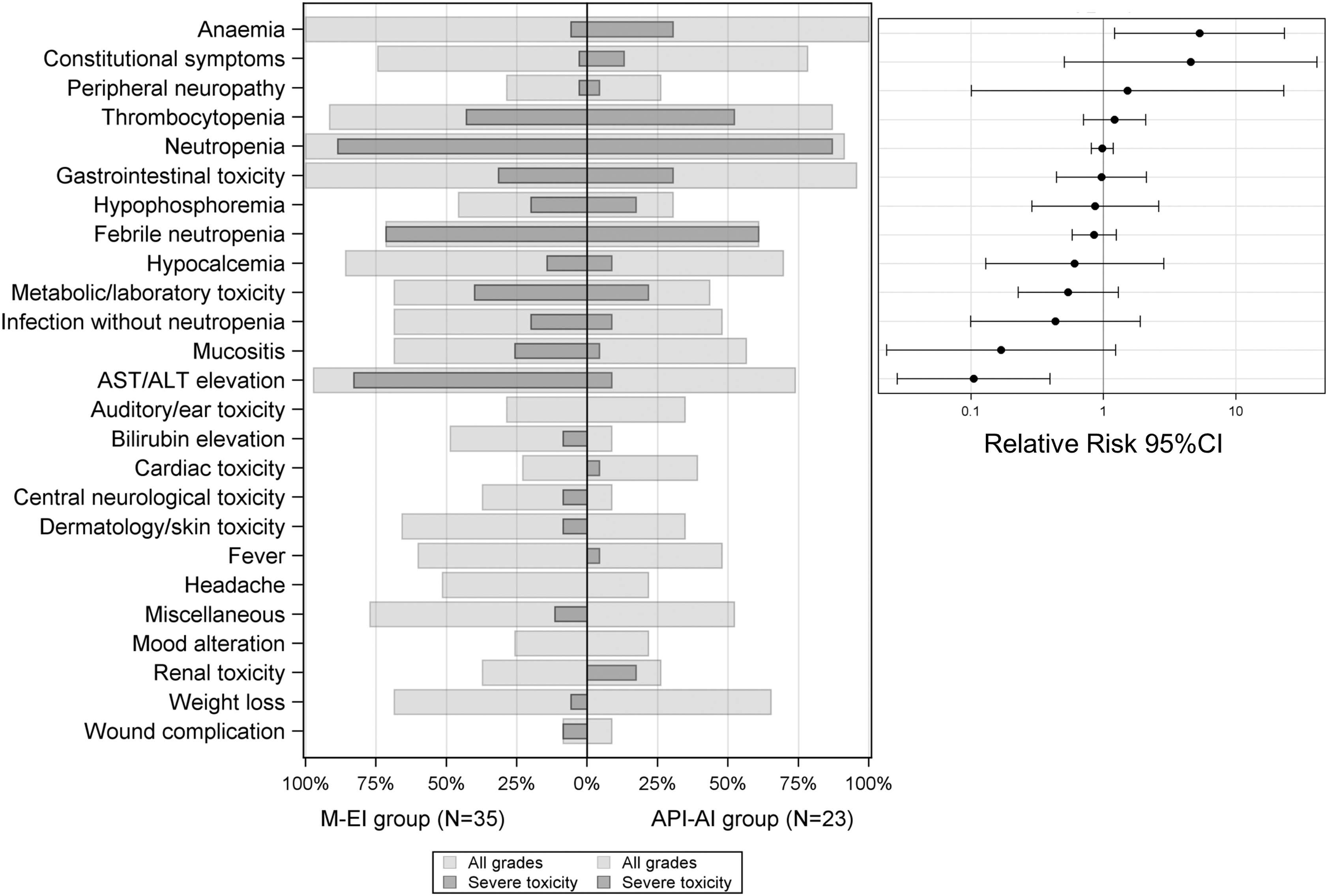
Adverse events according to the chemotherapy group (analysis performed for the randomized subpopulation only, n = 58). Left panel: The proportion of patients who had an adverse event, any grade (light blue for the M-EI group and light red for the API-AI group), and a severe adverse event (dark blue for the M-EI group and dark red for the API-AI group) in the 95 patients 18–25 years of age. Grade 4 hematological toxicities and grade ≥3 for all extrahematological toxicities were considered to be severe toxicities. Right panel: Relative risk of a severe adverse event in the API-AI group compared with the M-EI group, with the 95% CIs. Adverse events were assessed after each chemotherapy course using a list of 25 selected items from the National Cancer Institute–Common Terminology Criteria for Adverse Events version 3.0; a free-text area was available to document other adverse events. The adverse event types for which there were fewer than five patients with this adverse event have been pooled in the Miscellaneous category. For each adverse event type, the analysis was based on the maximum grade observed over the entire duration of the treatment. The adverse event types are ordered by relative risk. ALT, alanine aminotransferase; API-AI, doxorubicin–cisplatin–ifosfamide; AST, aspartate aminotransferase; CI, confidence interval; M-EI, methotrexate and etoposide–ifosfamide.
Most of the patients assessed for safety experienced at least one severe toxicity (grade 4 hematological or grade 3/4 extrahematological). The chemotherapy regimens exhibited different toxicity profiles, with more severe anemia with API-AI compared with M-EI and more transaminase elevations with M-EI. Mucositis occurred more often with M-EI. Only four patients in the API-AI group had severe renal toxicities. An API-AI patient exhibited cardiac toxicity (grade 3) and three M-EI patients had central neurological toxicities (grade 3). The incidence of acute ototoxicity was similar in the two groups (29% with M-EI and 35% with API-AI, none of which was severe).
Survival outcome
After a median follow-up of 5.0 years, 44 disease progressions/relapses were reported: 6 were local, 37 metastatic, and 1 was both local and metastatic (Table 3). An M-EI patient, previously treated for a retinoblastoma, reported a second cancer: a radio-induced osteosarcoma. There were 31 deaths due to osteosarcoma. Overall, the 5-year EFS was 50% (95% CI: 39–60) and the 5-year overall survival was 65% (95% CI: 54–74) (Fig. 4).

Event-free survival
Outcomes in the Overall Population and According to the Chemotherapy Regimen
Multivariate analysis, including initial staging (metastatic vs. localized disease) and age as a continuous variable.
CI, confidence interval; EFS, event-free survival; HR, hazard ratio.
In the univariate analysis, the 5-year EFS were not significantly different between both groups: 53% (95% CI: 40–66) in the M-EI group and 45% (95% CI: 30–61) in the API-AI group (HR = 1.30; 95% CI: 0.72–2.34, p = 0.38). The results were relatively stable in the multivariable analysis, adjusted for age and initial staging, with a HR (API-AI/M-EI) = 1.23 (95% CI: 0.68–2.22, p = 0.50). The overall survival was not significantly different between the treatment groups in univariate and in multivariate analyses.
For the OS2006 trial population that received M-EI (n = 409), the 5-year EFS of the 354 patients who were less than 18 years old was 57% (95% CI: 51–62) versus 53% (95% CI: 40–66) for the group of 55 patients who were 18–25 years old (HR = 1.1, 95% CI: 0.71–1.7; p = 0.67). Similarly, in the 106 patients treated with API-AI, the 5-year EFS was 46% (95% CI: 34–59) in the 66 patients who were over 25 years of age versus 40% (95% CI: 30–61) in the 40 patients who were 18–25 years of age (HR = 1.00, 95% CI: 0.58–1.73; p = 1.00).
Discussion
No statistically significant differences were observed in terms of survival and acute toxicities between patients treated with M-EI or API-AI regimens in the population of young adults with osteosarcoma prospectively included in the OS2006 trial. However, we cannot formally claim equivalence of the treatments due to possible selection bias without randomization. Moreover, the small sample size limits the statistical power (the posterior power is only 18% for 45 events).
Even though the MAP regimen is the standard treatment for osteosarcoma patients in most centers in Europe and North America, the feasibility of HDM in adults is controversial.7,12,15 This reluctance to treat adults with HDM may partially explain why the participation of 18- to 40-year-old patients in osteosarcoma trials is lower than expected, despite the fact that they account for 22% of all appendicular osteosarcoma cases.
However, our study has a number of limitations that make it difficult to conclude equivalence of the M-EI and API-AI regimens. First, certain investigational centers prefer either M-EI or API-AI for treating patients between 18 and 25 years of age. Thus to optimize enrollment we decided not to randomly allocate treatment but to allow each center to choose either M-EI or API-AI for the study. Baseline characteristics of patient populations in the M-EI and API-AI groups are similar and even if more patients had metastatic disease at diagnosis in the API-AI group compared with the M-EI group, this difference was not significant. Even so, metastatic disease at diagnosis is an important negative prognostic factor for treatment efficacy that probably reduced survival outcomes in the API-AI group. 16 Second, treatment duration and compliance was not equivalent in the two groups making it difficult to compare these chemotherapies. API-AI treatment was planned for 15 weeks compared with 13 weeks for M-EI. Even if more major modifications in pre- and postoperative treatments were reported in the M-EI group compared with the API-AI group (respectively 24% vs. 0 and 41% vs. 27%), these differences are not significant (p = 0.18). In addition, four patients in the M-EI group and one in the API-AI did not undergo surgery. Finally, our study results are limited by the small size of the datasets analyzed. This limited sample size and the absence of randomization precludes drawing any definitive conclusions from our data.
Safety data were only available and analyzed for the subpopulation of patients randomized in the zoledronate phase III study. Treatment toxicity is reported to vary with age: adults with osteosarcoma having an increased risk of toxicity and treatment-related mortality compared with children and adolescents.10,11,17 In the OS2006 study, the toxicity observed in patients 18–25 years of age and those younger than 18 years of age treated with the M-EI were similar. 18 Thus, our results confirm the acceptable tolerance of M-EI in young adults 18–25 years of age and that HDM is feasible for young adults. It is noteworthy that the acute toxicities were comparable to those reported with the standard MAP regimen. 5
In 1982, Rosen et al. introduced preoperative chemotherapy, with HDM, in the T10 protocol. 19 Since then, no research has shown the benefit of intensifying postoperative chemotherapy in poor responders. 20 Even if the early introduction of cisplatin and ifosfamide seems to increase the rate of good responders, this does not confer a significant survival benefit. 5 In France, the choice of chemotherapy takes into account treatment tolerance and safety. The French OS2006 trial confirmed the efficacy of the M-EI regimen that spared 40% of osteosarcoma patients from the toxicity associated with anthracycline and cisplatin treatment. 6 Indeed, anthracyclines were avoided in patients with good prognoses and the anthracycline dose reduced to 300 mg/m2 in patients with poor prognoses (i.e., poor responders and/or metastatic disease). This benefit is worthwhile even though doxorubicin-induced long-term cardiotoxicity is probably lower in young adults compared with children. Cardiotoxicity is probably underestimated in most reports on osteosarcoma treatment in children, since pediatric studies suggest that the development of anthracycline-related congestive heart failure may take more than 20 years.21,22 Indeed, cardiotoxicity is a major cause of hospitalization in long-term osteosarcoma survivors.23,24 Acute cardiotoxicity may be a surrogate for late cardiac toxicity. 22 In our study, acute cardiotoxicity was reported in 39% of patients treated with API-AI (35% grade 1–2 and 4% grade 3–4), versus 23% in those treated with M-EI (23% grade 1 and no grade 3–4). Cardiotoxicity reported in the M-EI arm was mostly in patients who received postoperative cisplatin and doxorubicin.
In terms of treatment and the resulting duration of the hospitalization, there was a more substantial treatment burden in patients treated with M-EI compared with API-AI. Median hospital duration was extended by 5 weeks in patients treated with M-EI. The duration of hospitalization is of major importance for young adult cancer patients. Hospitalization causes social, educational, and professional disruptions. In addition, it can influence compliance and reduce the dose intensity, which in turn can influence survival.25–27 Moreover, the substantial difference in hospitalization duration may have financial consequences that could influence the choice of chemotherapy.
Despite the limitations of this study, our analysis adjusted for initial disease staging and age, did not show any significant difference in survival between the regimens. Thus, M-EI and API-AI regimens are both viable options for treating young adults with osteosarcoma. The treatment choice should take into account the shorter treatment duration and improve the dose intensity with API-AI, as well as the higher risk of long-term cardiotoxicity.
Footnotes
Acknowledgments
The authors would like to thank all patients and their families, the investigators and their staff, the data management and data analysis teams, and the Unicancer team for coordinating and managing the study. They would also like to thank Trevor Stanbury (Unicancer) for medical writing support. In addition, they would like to thank the study pathologists, the members of the Independent Data Monitoring Committee, and the study funders.
Data Availability
Unicancer will share deidentified individual data that underlie the results reported under the following conditions: the data shared will be limited to that required for independent mandated verification of the published results, the reviewer will need authorization from Unicancer for personal access, and data will only be transferred after signing of a data access agreement. A decision concerning the sharing of other study documents, including protocol and statistical analysis plan, will be examined upon request. Unicancer will consider access to study data upon written request from 6 months until 5 years after the publication of this article.
Ethics Approval and Consent to Participate
All patients and/or their families provided written consent before any study-related activity. The study was performed according to the principles indicated in the declaration of Helsinki and Good Clinical Practice. The study was approved by a French Ethics Committee: Les Comités de Protection des Personnes—Ile-de-France VII (94000), reference: 06-017.
Authors' Contributions
The following authors were involved in study conception and design: L.B., S.P.-N., B.-V.O., M.-C.L.D. All authors were involved in the acquisition, analysis, and interpretation of the study data, as well as drafting and revising of this article. All authors have reviewed and approved this article for publication.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the French National Cancer Institute (INCa), NOVARTIS, Chugai, the Ligue Nationale contre le Cancer, the Fédération Enfants et Santé, and the Société Française des Cancers et Leucémies de l'Enfant.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.