
Abstract
Introduction:
Improvements in cancer survival rates for teenagers and young adults (TYAs) have resulted in quality-of-life issues into survivorship becoming increasingly important. However, infertility is a potential late side effect of cancer treatment, which can negatively impact on quality of life. Advances in assisted reproductive technologies have resulted in increasingly effective fertility preservation (FP) options.
Purpose:
This study aimed to explore nurses' experiences of undertaking fertility-related discussions with TYAs with cancer aged 13–24 years.
Methods:
An interpretive phenomenological analysis (IPA) approach was used. Eleven purposively selected nurses working on a specialist TYA cancer unit participated in semistructured interviews. Data were analyzed using IPA.
Results:
Parents/family were experienced as self-appointed informal gatekeepers who were perceived to hold the power to control nurses' access to communicate with young people about fertility issues. Nurses adopted a supportive role, which was enhanced by the positive nature of their relationship with the TYA. Uncertainty was expressed over whether the TYA had been fully informed of their infertility risk and potential FP options.
Conclusions:
Nurses should manage parental involvement sensitively if TYAs are to make informed decisions regarding their future reproductive health. There is a need for clear role delineation in fertility discussions to ensure that TYAs are provided with the opportunity to discuss infertility risk and be referred to a specialist before initiating cancer treatment. Nurses should cultivate the primacy of the nurse-TYA relationship to improve fertility care. Further research into the factors that TYAs may consider beneficial within the nurse–patient relationship is required.
Introduction
Improvements in cancer survival rates for teenagers and young adults (TYAs) 1 have resulted in quality-of-life issues such as infertility becoming increasingly important. Infertility is a sequela of cancer treatment, but determining individual risk is challenging. 2 While some cancer treatments are unlikely to compromise fertility, it is difficult to predict the likelihood of relapse requiring second-line therapy that is likely to cause infertility. 3
Advances in assisted reproductive technologies have resulted in increasingly effective fertility preservation (FP) options for those of reproductive age3,4 (Table 1, FP options). International clinical guidance recognizes the importance of FP for TYAs with cancer and states that discussion of potential infertility risks and FP options/referral before treatment is essential.5–11 The ability to retain reproductive potential is of primary concern for TYAs, both nationally and internationally.12–16 Yet, TYAs often experience inadequate fertility information provision, which may be a source of significant dissatisfaction.17–26
Fertility Preservation Options
TYAs report clear preferences for fertility-related discussion, including a respectful, open, and honest approach,19,27 recognition of the importance of fertility, 23 and improved communication between oncologists and fertility specialists. 28 In addition, TYAs strongly desire a participatory decision-making role.29–32 As research consistently indicates that receiving information about the impact of cancer on fertility is associated with lower patient distress, 19 improved quality of life,10,20,26 less regret,33,34 and improved coping, 15 it is critically important to engage in timely discussions to maximize future FP opportunities.
Despite guideline recommendations, barriers exist which may impede FP discussion. In the limited studies using a nurse-only sample, research from the United States, Netherlands, and Canada demonstrates that a lack of knowledge and training on the topic is a significant barrier to nurse's willingness to undertake fertility discussions.35–39 Research reflective of nurse practices in the United States and Netherlands also indicates role confusion; while some nurses view fertility discussion as their responsibility,36,40 others believe it is outside their scope of practice. 41 Alternatively, some nurses view it as a joint doctor/nurse role. 35 Similarly, no clear consensus exists among oncologists regarding responsibility for discussion. 42 International studies highlight that a patient's poor survival prognosis may negatively influence both nurses' and doctors' willingness to broach the subject.36,39,40,43–47
Given the international consensus indicating the imperative of retaining reproductive potential for TYAs following cancer and the negative effects of not doing so, it is important to further explore factors that influence nurses in undertaking fertility discussions. Research suggests that by virtue of their primary and extended contact, nurses are generally more available to patients than doctors, 48 are in an optimal position to have FP discussions,38,41,49,50 and play a pivotal role in addressing fertility concerns. 51 Consequently, a more comprehensive understanding from the nurse's perspective on this important topic is vital to better support TYAs with fertility concerns.
The aims of this study were to explore and interpret nurses' experiences, feelings, and associated meanings attached to undertaking fertility-related discussions with TYA cancer patients aged 13–24 years (United Kingdom definition for this patient population) 52 to advance understanding of factors that facilitate or hinder such discussions to progress clinical practice.
Methods
A qualitative interpretive phenomenological analysis (IPA) approach was used. 53 IPA involves a dual interpretive process dedicated to the exploration of meaning; a “double hermeneutic” whereby the researcher is trying to make sense of the participant trying to make sense of their experiences. 54 Ethical approval was granted by the local NHS Research Ethics Committee and University.
The study used a purposive sample of 11 nurses currently working on a Teenage Cancer Trust (TCT) Unit in England. Study details were distributed to all 34 nurses who fulfilled the inclusion criteria: any registered nurse employed on the TCT unit for a minimum of 6 months and who interacted with TYAs before initiation of cancer treatment. IPA utilizes small sample sizes that allow for depth of analysis and an idiographic focus on the “particular” uniquely embodied experience, rather than more general claims. 53 Participation was voluntary, and written consent was obtained.
The interview schedule (Table 2) was constructed by E.W. Interviews were conducted by E.W. between February and May 2016. The interviews, ranging in length from 28 to 44 minutes, were digitally recorded and transcribed verbatim. Data were securely stored, and confidentiality and anonymity were assured by removing all identifiable information. 55
Interview Schedule
Data analysis conformed to the IPA analytical process 53 (Fig. 1). In accordance with Yardley's 56 quality criteria, commitment and rigor were maintained by ongoing discussion of emerging codes between authors to test and develop the coherence and plausibility of the interpretation. Clarifications and modifications were made to increase the consistency of the analysis. Themes were elicited from the responses of over 50% of participants, although the focus was primarily on meaning rather than frequency. 53 The master table of themes (Table 3) allows for transparency of the validity of the interpretation based on the quotations. 56
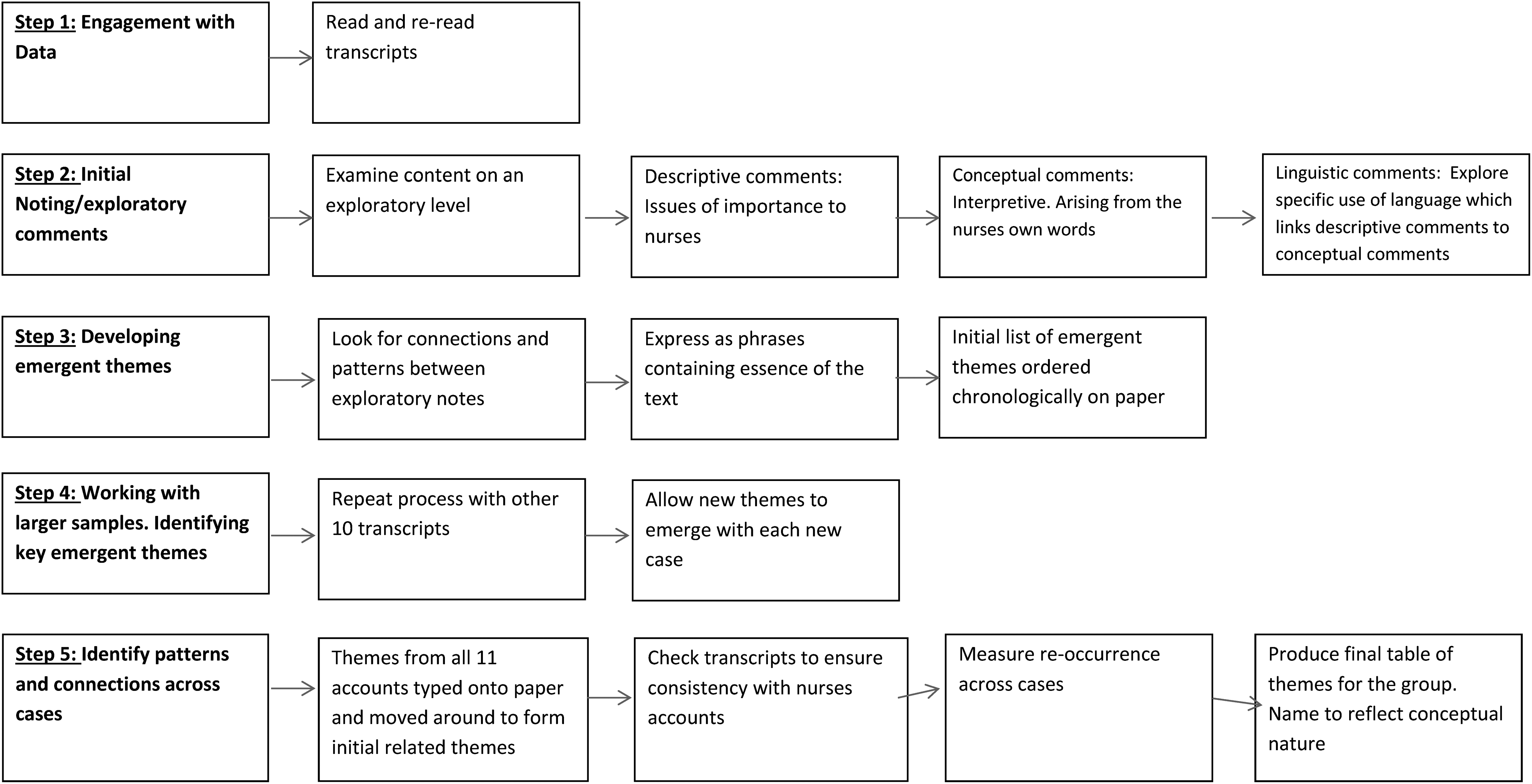
Steps in the interpretive phenomenological analysis analytical process. 53
Master Table of Themes for All 11 Participants Illustrated with Sample Quotations
Results
The 11 participants ranged in age from 21 to over 50 years and reflected various levels of nursing experience and United Kingdom pay scale banding (Table 4, participant demographic data). Two inter-related super-ordinate themes were selected for discussion in this article based on their international relevance in supporting nurses to effectively manage fertility issues.
Participant Demographic Data
Band 5: Initial grade of qualified nurse. Band 6: Experienced senior nurse with more responsibility for the overall running of the ward. Band 7: Ward manager/ward sister responsible for the management of staff and has control of the ward budget. 75
TYAs, teenagers and young adults.
Parents/family control
Nurses experienced parents/family as self-appointed informal gatekeepers, who nurses perceived to control access to the TYA. This hindered them in speaking privately with the TYA about fertility.
“…if they have got their parent there urm and their parent is very controlling…his family they weren't very helpful…I think I did ask for his family to leave the room for a minute while I spoke to him, but they were coming in and out still … But I guess you have just got to ask them [TYA about fertility] haven't you.” (P7).
“I don't know whether I would necessarily find it uncomfortable talking directly to a patient, but if they [TYA] were surrounded, a patient with family, I would find that quite challenging…I wanted to speak to them alone” (P6).
Seemingly, parents were viewed by nurses as “controlling” (defined as the power to influence or direct people's behavior or the course of events). 57 Nurses' sense of control appeared to be unwillingly relinquished to the family. This challenged nurses' determination to speak to the TYA about fertility issues while alone, which appeared to be an essential facilitator.
From an alternative viewpoint, the quotation below suggests that nurses feel that TYAs themselves may prefer to be alone when discussing sensitive issues such as fertility and sexual function.
“Whereas if they were on their own [TYA] and you had that conversation…. I feel like they would be more open to it” (P1).
Nurses experienced parents' constant physical presence as an obstacle to open communication, rather than anything they say or do.
“…he was very close to his parents and they didn't often leave him on his own…so it was a big thing to be able to say is there somewhere we can talk to him on his own without you guys being there” (P1).
Here the nurse appears to try to make sense of her experience by her use of the expression “big thing,” which appears to emphasize her perception of the enormity of the task of accommodating the distinctive needs and priorities of the TYA and those of parents. Re-establishment of personal control is viewed as a priority, and she perceives that this will be facilitated by the absence of parents. Participant seven experienced difficulty in “getting through to the young person” because “they [family] can kind of take front stage.” The curious use of this idiom hints at her perception of viewing the family at the forefront of care; this appears to be contrary to her perception of the nursing ideal of patient-centered care.
The following account supports nurses' perceptions that parents' controlled access to the TYA:
“I have had a parent that has said can we not talk about it um, [fertility] say with a 13 year old…” (P5).
A subtle difference in language expression and meaning illustrated in the following nuanced account supports the belief and consequent action that it was unacceptable to speak to the young person:
“I am thinking of one situation where a parent had specifically told the consultant that they didn't want him or us to talk to the child [14 years] at all about fertility. And so, we didn't, rightly or wrongly” (P9).
These nurses present a passive acquiescence within a situation where the decision had been removed from them, with a relinquishing of personal agency connected to a perceived lack of control over events and the ability to influence them.
Further restrictions imposed by parental gatekeeping were experienced:
“Sometimes parents try and hinder your conversations… they don't want to broach that subject [fertility] with children and sometimes feel we shouldn't as healthcare professionals” (P3).
Parents of younger males expressed doubt that their son was capable or mature enough to engage in masturbation [required for semen storage], and several nurses reported an “embarrassment issue” on the young males' part to be a barrier to conversations, due to the intimate nature of the subject.
Discussion of sexually related issues was also a source of apprehension for nurses, compounded by the challenges of parents'/families' presence.
“It can't be your first sexual experience…I had to ask that whilst the ‘commotion’ of his family around” (P7)
As a facilitating action to manage the triadic relationship, nurses placed emphasis on communicating with parents about the importance of FP discussion. This was seen as a way of mitigating parents'/families' capacity to exercise control over access to TYAs, to permit communication. Arguably, the nurses' ability to articulate the benefit of a discussion is seen as a controllable event, helping to reconcile opposing beliefs.
“… to work with families about explaining why we need to have that conversation with young people urm and what we can do about it” (P4).
“…trying to explain to them, to the parents that it is a discussion, it's backed up with information…they [young people] shouldn't be denied that opportunity” (P5).
Nurse as a continuing support role
Ten out of eleven nurses discussed their experiences and feelings associated with fertility discussions which revealed a sense of responsibility for such communication. Rather than being primarily responsible, nurses acknowledged that it was part of their role, but the emphasis was given to providing an ongoing supportive function. This appeared to provide nurses with a sense of purpose and self-worth and opportunity to fulfill what they perceived as a valuable role in responding to evolving queries.
“It's the sort of thing that actually afterwards people do have questions you know, days, weeks, months down the line about. And so it inevitably does fall under a nursing err responsibility as well” (P2).
“I think currently it is our role [discussing fertility] as well, or part of our role because once they [doctors] have done that discussion the patient or family might have more questions and we are the one who be dealing with them day to day” (P10).
The nurses' perception of the supportive nature of their role encompassed a “checking responsibility” to ensure that the doctors had undertaken the discussion. Several nurses attempted to understand their role in fertility care as an ongoing process rather than a “one off” discussion. Nurses described it as a “continuing process” to pick up from the doctor's initial conversation and “carry it on” in a supportive capacity.
“It's a continuing process… they [TYA] may have had the initial conversation but quite often they are under our care when those [FP] appointments happen” (P6).
The use of the phrase “may have had” hints at this nurse's uncertainty as to whether the discussion had definitely occurred and reinforces the nurses' perceived need for a checking responsibility.
There seems to be a sense here of the nurses' willingness to engage with TYAs and contribute in a useful way that was personally meaningful to them, providing ongoing support to TYAs along the continuum of their cancer journey.
The success of the continuing supportive role was often seen to be dependent on the nature of nurse-TYA relationship, and establishment of rapport was viewed as beneficial in facilitating this role. Interestingly, no nurses viewed their relationship with TYAs as a potential barrier; in fact, all perceived it to be a facilitator for open conversation.
“If you have got rapport with them [TYA], then they will start to open up with you and be able to have those discussions” (P5).
“If you get to know them better and you have built up a rapport with them it's a lot easier for them to talk to you and for you to approach it with them” (P9).
Here, a supportive relationship is seen to be potentially beneficial for both the nurse and the TYA.
Nurses also experienced very “different relationships” with TYAs to those held by doctors, which they perceived to be conducive in enabling the conversation to emerge naturally within day-to-day interactions. These beneficial relationships were perceived to facilitate the nurses' ongoing supportive role; notably, while not accepting responsibility for the initial discussion.
Discussion
In this study, an important finding was the significance of the perceived control held by parents/family that nurses experienced as self-appointed informal gatekeepers. Parents/family attempted to control fertility information and their wishes were often acceded to. Similarly, De Vries et al. 58 investigated attitudes of physicians and parents toward discussing infertility risks with young males and also identified that parents were found to exert “strategic control” (p389) regarding their son's involvement in discussions due to concerns about their sexual immaturity. However, in contrast with the current study, 14/15 physicians in De Vries et al's 58 study reported discussing the topic with TYAs, even if parents refused to give permission.
These contrasting findings may be explained by the sample composition of physicians rather than nurses. Previous research has identified that nurses feel less knowledgeable59,60 and less comfortable 49 discussing fertility issues than physicians. Hence, nurses in the present study may have felt less confident in disregarding and overriding parent's wishes.
One possible explanation why parents may not allow TYAs to be approached may be attributed to their sole preoccupation with immediate survival, 47 assumption that TYAs cannot comprehend the process,61,62 and parental/family concerns about further distressing the TYA who may be emotionally overwhelmed following a traumatic cancer diagnosis.29,44,48 However, research has demonstrated that patient and parent discomfort/anxiety levels are often overestimated by health care professionals.30,63
TYAs desire to be active decision makers29–32 and can indeed cope with fertility matters being raised alongside a cancer diagnosis with support. 64 While parental concerns are understandable, evidence suggests that parenthood priorities shift over time and become a significant concern into survivorship.14,30 Furthermore, cancer survivors diagnosed when aged 10–21 years often regretted that infertility was not discussed at the time of diagnosis. 30
Nurses in this study experienced the necessity to negotiate what they perceived as the “challenges” of parental control. They reported the need “to work with families…” (p4) and to “try to explain to them…” (p5), as facilitating actions in an effort to emphasize the significance of a FP discussion to parents/families. Nurses saw this as a way of supporting TYA participatory decision-making. Balancing TYA engagement with parental involvement is pivotal, considering that parents and TYAs do not view oncofertility decision-making in the same way 29 and may have discrepant priorities regarding future fertility intentions. 65 If they desire, TYAs should participate in discussions, taking account of their emotional and mental maturity to freely voice their preferences.64,66
Paradoxically, even those TYAs who do not prioritize future parenthood value information regardless of their decision to proceed with FP or not.14,21,63,67 This suggests that further explanatory communication with parents about the value of a FP discussion, as advocated in this study, is indeed required to facilitate the TYAs' reproductive priorities to be voiced. Potential difficulties should be skillfully anticipated and managed by nurses. Further research is needed to explore ways of effectively engaging with parents to ensure that TYA views are considered, given the diversity of this patient population in terms of age and levels of autonomy, which may be factors influencing communication strategies.
In this study, nurses' perceptions of their role in fertility discussions were clearly expressed as forming part of a “continuing process” rather than a “one off” discussion, which supports the findings of previous United States research. 36 In addition, nurses also acknowledged the need for a “checking responsibility” and expressed doubts whether the TYA “may have had” (P6) a discussion. These findings reinforce the need for clear role delineation; allocating nurse responsibility for establishing and maintaining links with fertility specialists may contribute to ensuring that TYAs' reproductive needs are met.
Research suggests that having access to a FP specialist38,68,69 and close collaboration with the fertility team70,71 are important determinants in discussing FP. Therefore, while there is a need for a clearly defined role for nurses' in raising the issue of fertility routinely, 51 all members of the multidisciplinary team are integral in providing oncofertility support,72,73 considering that fertility concerns may be present at any stage of the cancer trajectory. 74
In the current study, nurses perceived the nature of their relationship with TYAs as “very different” to those experienced by doctors and a potential facilitator underpinning effective fertility communication and support. The establishment of rapport was seen to enhance such relationships. These findings highlight the importance of utilizing the benefits of the nurse–patient relationship if nurses are to be effective advocates for TYAs.
Limitations
While providing valuable data on this under-researched issue, the small self-selected homogenous sample, recruited from one specialist unit in England, limits generalization to a wider population. A self-selected sample may have resulted in participants with a greater interest in the fertility topic. In addition, TCT Units in England provide care for the 13–24 year age range. 52 Further research investigating the age-specific challenges relating to FP discussions within this age group is warranted, to expand upon our observations and inform TYA care providers of these patients' specific needs.
Conclusion
This study offers new insights into this significant contemporary issue from the perspective of nurses themselves. Biological parenthood may not be a priority for all TYAs. However, nurses are uniquely positioned to play a significant role in helping to fulfill hopes of parenthood after cancer for those TYAs who desire it and improve overall quality of life into survivorship.
Footnotes
Acknowledgment
The authors acknowledge the support and guidance provided by Martyn Geary during the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.