
Abstract
There is limited research on young adults (YAs) living with cancer and even less concerning those with metastatic/advanced disease. The purpose of this scoping review was to map and summarize the current state of empirical research on the psychosocial experiences of YAs living with metastatic/advanced cancer, highlighting gaps in the published literature. This study was guided by Arksey and O'Malley's scoping review methodology. MEDLINE, CINAHL, and PsycINFO were searched in consultation with a medical research librarian, for English-language articles published until June 2018. Three key journals were hand-searched along with the first 100 hits on Google Scholar. In addition, ProQuest Dissertations and Theses was searched for dissertations published until February 2018. Two authors independently screened titles/abstracts to identify articles for full text review. Data were extracted on study characteristics and outcomes related to the guiding review question. Thematic analysis was used to analyze the data and identify overarching themes. Summary statistics were reported. The search strategy retrieved 2846 published articles. After reviewing 47 in full text, 10 studies were eligible for inclusion. The results from the included studies fell into four themes: (1) search to make meaning of their illness; (2) patient–provider relationships; (3) mental health and psychosocial well-being; and (4) interventions. Research concerning the psychosocial experiences of YAs living with metastatic/advanced cancer is limited. The authors provide four recommendations as a starting point for further research. Understanding the patient experience is imperative for designing effective health policies, programs, and interventions for this population.
Introduction
The lives of young adults (YAs; 18–39 years of age 1 ) are influenced by educational, work, lifestyle, and psychosocial (psychological and social) factors.2–5 Young adulthood is a time for people to develop independence, relationships, families, professional education, and/or careers. 6 These alone are difficult life transitions, which is why a cancer diagnosis during young adulthood can impede important life tasks that are imperative for adulthood (e.g., establishing autonomy, dating, and financial independence).3,7–10 Because of this, YAs diagnosed with cancer have unique psychosocial challenges associated with their stage of development.7–10 YAs may have to deal with interruptions to their education and careers, which can result in lost occupational and financial opportunities.9,10 This financial strain can also be met with challenges in one's intimate and social relationships, fear of recurrence and physiological side effects from treatment, including impaired or reduced fertility. 10 Additionally, YAs with cancer often feel isolated from peers due to their illness. 11 As a result, cancer peers of a similar age, who understand what they are going through, often serve as a source of social support. 11
Cancer control organizations have advocated that person-centered cancer care be delivered by specialist providers in an age-appropriate manner, particularly for YAs due to these unique challenges. 7 However, access for some patients to YA multidisciplinary teams is limited or not feasible. From a biomedical standpoint, the YA cancer population has not seen survival progress comparable with that of pediatric and older adult oncology populations over the past three decades.12,13 YAs often receive delayed diagnoses for many reasons, including delaying seeking help from medical professionals and ignoring their symptoms, and health care providers' disinclination to consider cancer in this age group.7,14 Consequently, at the time of diagnosis, YAs often present with cancers that are at a more advanced stage and are more aggressive. 7 Making decisions about treatment plans can be difficult for the YA and their health care team because there are not always clear treatment outcomes for this population in the literature, as YAs are historically not included in clinical trials.7,9 For many cancers, this then results in poorer overall health outcomes that may include the cancer advancing/metastasizing. 7
Those living with metastatic/advanced cancers have unique needs within the YA cancer population due to the complex decisions that they must make for their cancer care and the uncertainty that they face for their future. 15 However, this is a relatively new area of exploration as the majority of YA research has focused on curative and survivorship issues, with limited research focused on YAs living with metastatic/advanced illness. 15 This information is critical for understanding and improving their care and experiences. The purpose of this scoping review was to map and summarize the current state of empirical knowledge of the experiences of YAs living with metastatic/advanced cancer.
Methods
YAs living with metastatic/advanced cancer are a historically marginalized oncology group and not one that has been comprehensively reviewed. 16 An initial search of the literature revealed limited studies on the experiences of YAs living with metastatic/advanced cancer. Therefore, a scoping review, following the methodological framework developed by Arksey and O'Malley 17 and furthered by Levac et al., 18 was chosen as an appropriate method for mapping the current state of empirical knowledge and highlighting relevant gaps around the following research question: What is the current state of empirical knowledge of the psychosocial experiences of YAs living with metastatic/advanced cancer? These types of reviews can serve as a point of departure for future reviews and primary research. The authors used Arksey and O'Malley's 17 five-step approach (identifying the research question, identifying relevant studies, study selection, charting the data, collating, summarizing, and reporting results) to structure the review. Theoretical stances and interpretations are not customary in scoping reviews and therefore were not used in this study. A protocol for this review was not registered and research ethics board approval was not obtained, as the data were publicly available. The manner in which the study was carried out and reported was guided by The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) criteria. 19
Scoping the inquiry
The search strategy was developed with support of an experienced medical research librarian to find both published and unpublished studies using MeSH and key terms (e.g., cancer, metasta*). An initial limited search of CINAHL was conducted. It was followed by an analysis of text words contained in the titles, abstracts, and index terms used to describe key articles. This CINAHL search strategy (Fig. 1) was discussed between the investigators and informed the development of a search strategy that was tailored for each information source.

CINAHL search strategy.
Eligibility criteria
The eligibility criteria for this study were guided by the Population Concept Context (PCC) framework for scoping reviews. 20 For population, this scoping review considered all studies that focused on YAs living with a metastatic/advanced cancer. In the YA oncology field, there are inconsistencies in the defining age range of young adulthood. Although the authors acknowledge and align with the age range of the Journal of Adolescent and Young Adult Oncology (JAYAO; 18–39 years of age), 1 this review considered studies for which the defining age range of young adulthood differed. Studies that investigated adolescents and YAs were included if the data from YAs were presented separately. Research concerning the experiences of other populations (e.g., partners, health care providers, adolescents) were excluded. The concept examined by this scoping review was the psychosocial (psychological and social) experiences of YAs living with metastatic/advanced cancer. Recognizing that cancer is a biopsychosocial experience, studies exploring only the biomedical experience or biomedical health outcomes of participants were excluded. The context for this review concerned any studies that had been conducted in a hospital or community context about the experiences of YAs living with any metastatic/advanced cancer.
Sources
This scoping review considered empirical research of qualitative, quantitative, and mixed-methods designs. Other reviews were not included; however, their included articles were evaluated for inclusion/exclusion in this study. Opinion papers were excluded as the intent of this review was to explore the current state of empirical knowledge, defined as published or unpublished research studies. Additionally, books were not considered due to the logistics of timing and resources to complete this review. Conference proceedings were also excluded. Studies had to have been published in English to be included. Due to the limited amount of information on this marginalized oncology population, no specific date range was employed.
Search strategy and screening process
In collaboration with a medical research librarian, a comprehensive search strategy was developed after the aforementioned preliminary search was complete. One of the investigators (E.K.D.) and the medical research librarian conducted all searches. MEDLINE (Fig. 2), CINAHL, and PsycINFO were searched until June 2018. In addition, JAYAO was hand-searched dating back to its first edition in 2011 to June 2018. Supportive Care in Cancer and Psycho-Oncology were also hand-searched for relevant literature from the past 5 years (June 2013 to June 2018). This timeline was developed to look at these journals over several years in a manner that was feasible for the project. A search for unpublished studies included ProQuest Dissertations and Theses (to June 2018) and the first 100 hits on Google Scholar. Additionally, reference lists of other reviews generated in the search were reviewed for additional studies that met the inclusion criteria.
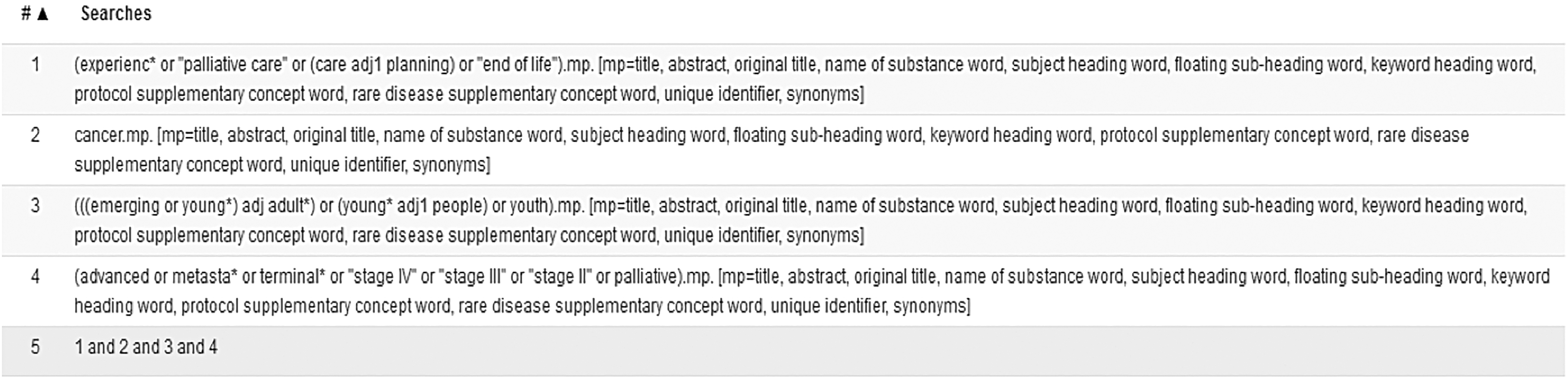
MEDLINE search strategy.
Following the search, all identified citations were uploaded into Covidence 21 and duplicates were removed. Titles and abstracts were screened by two independent reviewers (E.K.D. and R.U.) for assessment of inclusion. The full text of selected studies were retrieved and assessed in detail. Full text studies that did not meet the inclusion criteria were excluded. Any disagreements that arose were discussed between the two reviewers, with a consensus achieved.
Data extraction and summary
A data extraction sheet was developed by the investigators and piloted with three of the included studies to determine if it was extracting all relevant outcomes for the review. The information collected (Table 1) included the publication date, country in which the research was conducted, research design, number of participants, description of participants, measures used (if applicable), and outcomes related to psychosocial experiences. After it was refined, data were extracted from the included studies by one of the reviewers (E.K.D.) and verified by the second reviewer (R.U.). To identify gaps in the empirical knowledge, key findings across all studies were analyzed using thematic analysis to sort the data into themes of experiences described. After the investigators had familiarized themselves with the data by reading and re-reading the results, concepts were assigned initial codes, which were collapsed into overarching themes that were continuously reviewed and revised. 22 The number of studies by country, year of publication, tumor groups, time since diagnosis or before death, and research design were described using summary statistics.
Summary Table of Included Studies
Results
Search results
An initial 2846 references were imported for screening from the aforementioned search strategy. Of these, 564 articles were identified by Covidence 21 as duplicates and removed. The remaining 2282 articles were screened by titles and abstracts. From this, 2235 studies were identified as irrelevant. The remaining 47 references were assessed in full text for eligibility. Of these, 37 studies were excluded because they were either of the wrong study design (e.g., did not focus on psychosocial outcomes; [22]), concerned the wrong patient population (11), or were conference proceedings (4). Ten studies remained eligible for inclusion (Fig. 3). See Table 1 for summarized study characteristics and Table 2 for data extracted from included studies.15,23–31
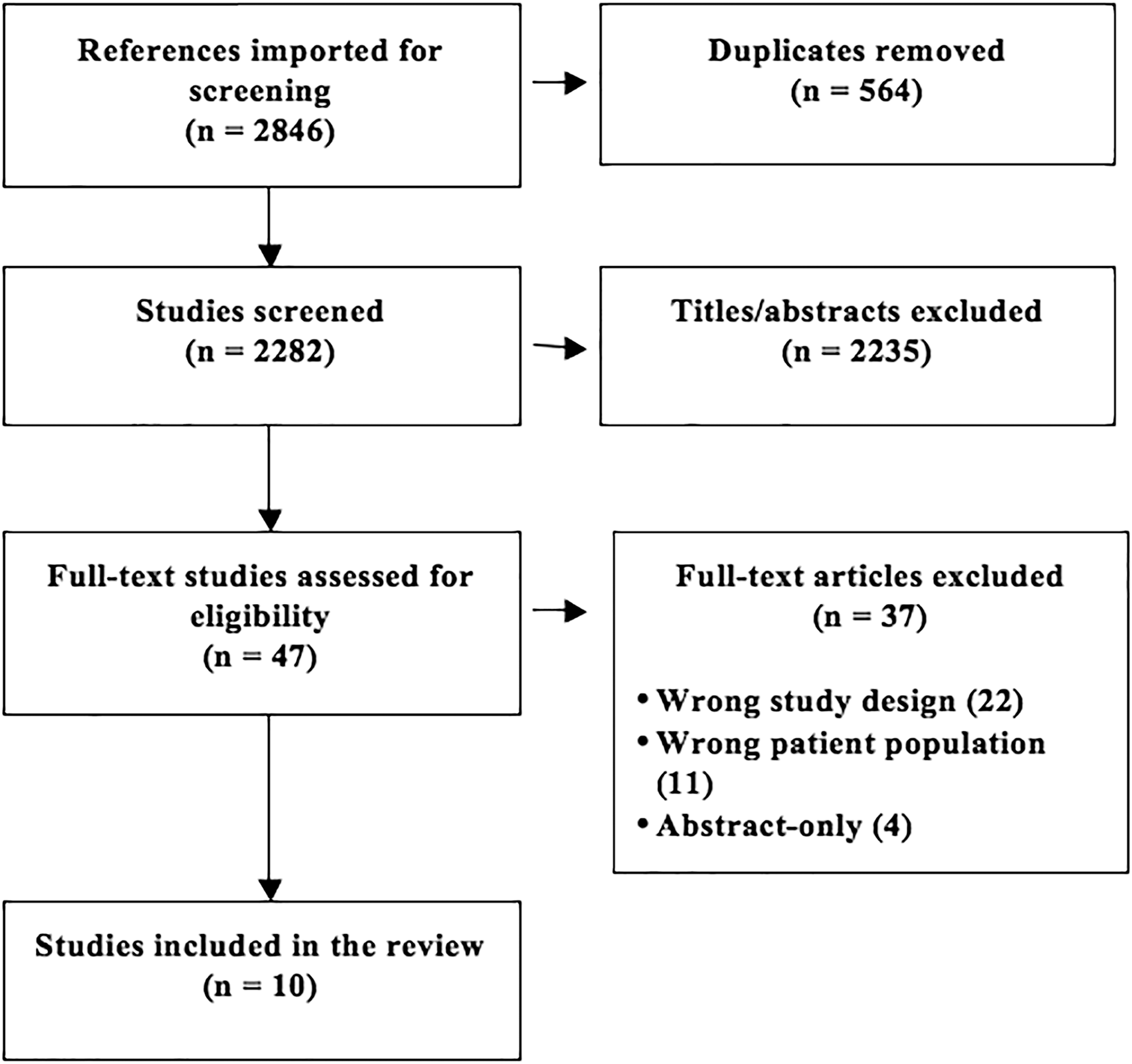
The PRISMA diagram of eligible studies. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Data Extracted from Included Studies
CARES-SF, Cancer Rehabilitation Evaluation System—Short Form; COPE, Coping Orientation to Problems Experienced; HADS, Hospital Anxiety and Depression Scale; ISEL, Interpersonal Support Evaluation List; MBC, metastatic breast cancer; MOS, Medical Outcomes Study; MQOL, McGill Quality of Life Questionnaire; PEACE, Peace, Equanimity, and Acceptance of the Cancer Experience; PG-12, Prolonged Grief Disorder Scale; SCID, Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorder, 4th Edition; SD, standard deviation; THC, The Human Connection; YA, young adult; YES, Yale Evaluation of Suicidality.
Characteristics of eligible studies
Of the 10 included studies, the majority (7) were conducted in the United States,23,24,26–30 with the remaining coming from Canada (2)15,31 and Korea (1). 25 Studies were published between 2011 and 2018. Two were published in 201826,31 and 2015.24,25 One study was published in 2017, 15 2016, 23 2014, 30 2013, 29 2012, 28 and 2011, 27 respectively. The study designs varied considerably: three were qualitative,15,23,24 four were cross-sectional,27–30 one was a one group pretest/posttest plot design, 25 one was a multicenter prospective cohort, 26 and one was a single-arm feasibility study. 31 The time since diagnosis or before death was inconsistently reported, with time not provided for two of the studies.15,25 Seven of the studies involved a mixed group of diagnoses.15,24,27–31 One study explored the experiences of an individual with rhabdomyosarcoma, 23 one examined women with metastatic breast cancer, 26 and another included only those with grade II or III osteosarcoma. 25
The investigators identified four major themes related to the experiences investigated in the 10 included studies: (1) the patient's search to make meaning of their illness; (2) patient–provider relationships; (3) their mental health and psychosocial well-being; and (4) interventions to improve quality of life and well-being (Fig. 4).
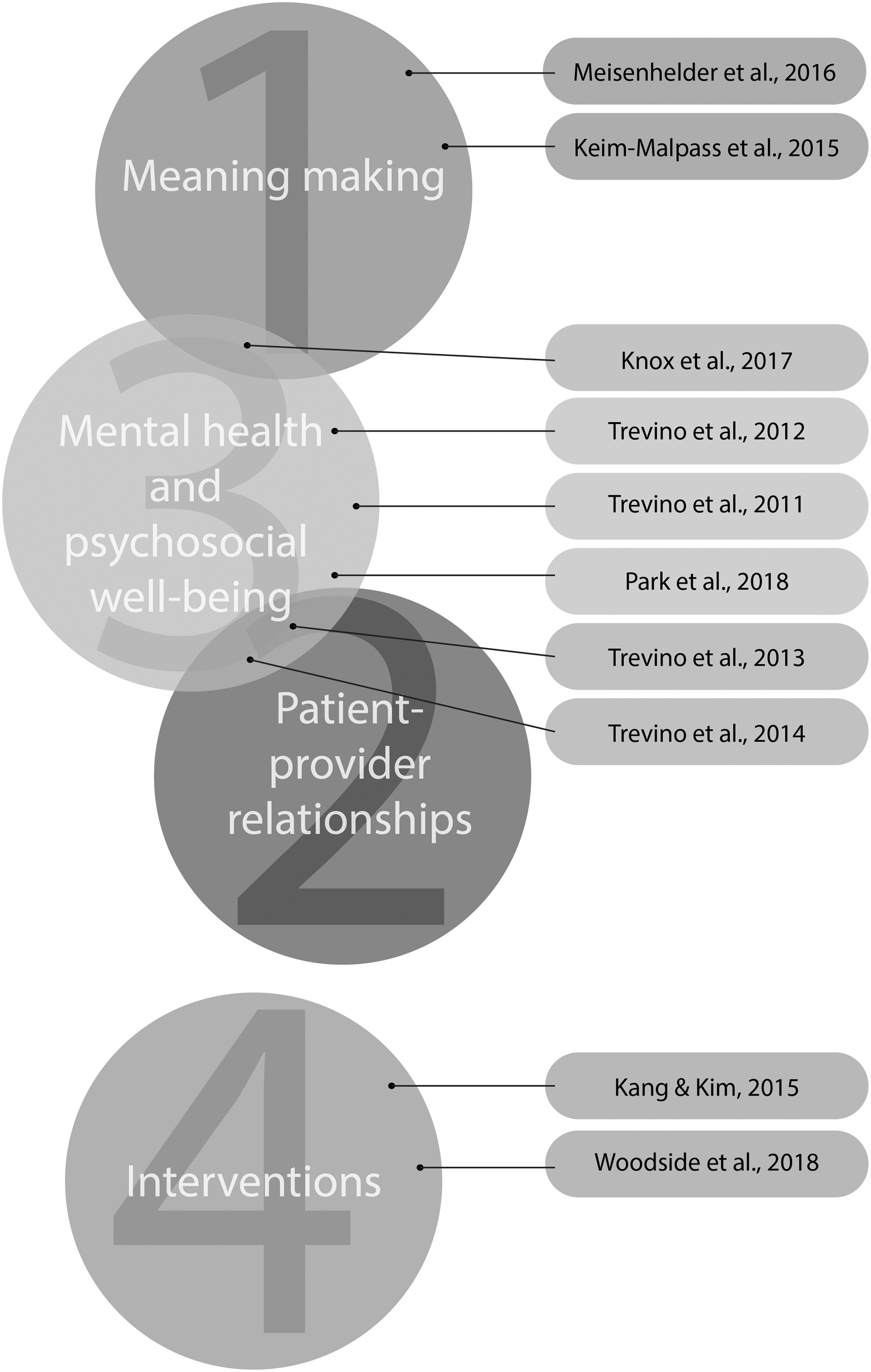
Included studies and their related themes.
Meaning making
Three studies discussed findings around meaning making for YAs living with metastatic/advanced cancer.15,23,24 They were all qualitative in design,15,23,24 with two exploring what participants had written within the last year of their life.23,24 Meisenhelder et al. 23 sought to identify patterns of spiritual coping in a personal prayer journal started at the end of primary treatment of a 19-year-old woman living with terminal rhabdomyosarcoma. One of the themes of the study was her offering her life to God, asking Him to take her, and to use her life to do His work. 23 The researchers also found a theme of thanking God, which included expressions of trust, praise, and thanksgiving. 23 Keim-Malpass et al. 24 explored the illness experience at end-of-life among young women with cancer. The women had varying diagnoses and maintained online illness blogs while living with their disease. 24 The study examined the last 6 months of blogs the women wrote. Although the illness experiences described by the women were greatly different, the overarching theme the investigators found was the importance of the online space for legacy making. 24 A third qualitative study by Knox et al. 15 explored the experience of YAs with advanced cancer and found that meaning making tended to be constructed around future-oriented goals rather than upon the life that had been lived.
Patient–provider relationships
Findings from two studies pertained to the experiences YAs living with metastatic/advanced cancer have with their providers, relating to the positive effect these relationships could have on patients' health.29,30 Trevino et al. 29 conducted a cross-sectional study that sought to evaluate the relationships between patient–oncologist alliance, psychosocial well-being, and treatment adherence. Of the 95 participants, one third had breast cancer and the remaining had a mix of diagnoses. 29 The authors found that alliance was significantly and positively associated with greater perceived social support and less severe illness-related grief. 29 After controlling for significant confounding influences (i.e., metastases, appraised support, and grief), alliance remained significantly associated with greater willingness to adhere to treatment and greater adherence to oral medication. 29 Participants with metastatic disease at the time of interview reported a stronger alliance than participants without metastatic disease. 29 In a similar study, Trevino et al. 30 found that 22.6% of the patients (n = 93) screened positive for suicidal ideation. However, those who had a strong therapeutic alliance with their oncologist were at a reduced risk for suicidal ideation upon controlling for other factors (i.e., cancer diagnosis, social support, mental health discussions with their health care providers, and use of mental health interventions). 30
Mental health and psychosocial well-being
Notably, 6 of the 10 included studies had findings related to mental health experiences.15,26–30 Three reported findings around the experience of grief.27–29 Trevino et al.'s 29 study on alliance between patients and oncologists found that frequent thoughts related to ending cancer treatment were associated with more severe grief and lower levels of psychological quality of life. Better adherence to cancer therapy was associated with better psychological quality of life. 29 They found that younger age was associated with more frequent thoughts around ending cancer therapy. 29 Trevino et al. 27 conducted a cross-sectional study that examined the relationship between grief due to cancer-related losses and life disruption due to cancer symptoms in YAs with advanced cancer. Their sample of 53 people consisted primarily of females, with more than one third of the population having breast cancer and the remainder having a mix of diagnoses. 27 The study found that higher levels of grief were associated with greater life disruption after controlling for an interviewer rating of physical performance status. 27 Grief was a significant positive predictor of life disruption after controlling for performance status. 27 Performance status was inversely related to life disruption. 27 In a similar study, Trevino et al. 28 found that YAs use six coping factors to cope with their illness: proactive, distancing, negative expression, support-seeking, respite-seeking, and acceptance coping. Whereas acceptance and support-seeking were the coping styles used most frequently, the use of negative expression as a coping style was positively associated with severity of grief after controlling for depression, anxiety, and other confounding variables. 28 Anxiety was positively associated with the support-seeking coping style after controlling for depression and grief. 28
Anxiety and depression were investigated in a study by Park et al. 26 who conducted a multicenter prospective cohort study to determine their prevalence in young women with newly diagnosed de novo metastatic breast cancer and whether sociodemographic and disease characteristics were associated. The study found that these patients experienced depression, but that it was less common than anxiety symptoms, which they frequently experienced. 26
Knox et al.'s 15 qualitative study found that the diagnosis of cancer was universally experienced as isolating and unexpected, as serious illness is seen as an issue for older people. Participants felt forcefully removed from the course of life, believing their achievement of developmental tasks essential to establishing adulthood (e.g., becoming autonomous, forming new relationships) were interrupted. 15 The authors noted that there was a constant presence of the challenge of living in the face of dying but it was typically unarticulated. 15 Many of the participants expressed reluctance to engage in individual psychotherapeutic treatment. 15
Interventions
Two studies explored interventions to improve quality of life and well-being of YAs living with a metastatic/advanced cancer. One explored meaning making through a program titled “Meaning of My Life”. Kang and Kim 25 conducted a one-group pretest/posttest plot design to develop this meaning-centered program. The study investigated 12 men diagnosed with either grade II or III osteosarcoma. The program, titled “Meaning of My Life,” consisted of five individual sessions geared toward understanding the meaning of life. The authors found that after the intervention the meaning of life (from the Meaning in Life for Adolescents 32 questionnaire) and quality of life scores of the participants significantly improved. 25
Woodside et al. 31 were the only researchers to explore a physical health intervention for YAs living with a metastatic/advanced cancer. Their intervention spanned 7 weeks and used a DVD to introduce yoga to this population. 31 All four of the participants were female and the majority had breast cancer, while one had lung cancer. 31 In terms of physical improvement, participants cited improved range of motion, an opportunity to improve their health (separate from medical interventions) and improvements in functional and physical well-being as reasons they benefitted from the intervention. 31 Participants also reported the intervention helped to improve spirituality, palliative specific and general quality of life. Participants felt better as a result of their program and it was viewed as an occasion for self-care. 31 Obstacles to participating included being on vacation, feeling unwell, having physical pain, or caregiver responsibilities. 31 Distractions (pets, etc.) were challenges and reasons participants took part in the program for shorter durations. 31 Knowing they would feel better after completing the yoga session was the motivation some of the participants used to keep going. 31 In general, it was felt that having a home-based program was an asset. 31 At follow-up, all participants indicated that they were continuing to do the yoga. 31 All felt others in a similar situation would benefit from the program. 31 Participants felt that connecting with others doing the same yoga-based intervention could potentially improve motivation to complete the program. 31
Discussion
The results of this study confirm the initial observation of a scarcity of empirical data on the experiences of YAs living with metastatic/advanced cancer. The studies, which were primarily conducted in North America, also employed inconsistent definitions of the age range of young adulthood. Amongst the 10 studies, mental health and well-being was the most commonly investigated experience of YAs.15,25–31 However, the aspects of mental health that were reported on were diverse. Throughout the four identified themes, a wide range of personal and interpersonal experiences were explored. With limited empirical research on the topic, it is clear that research has yet to comprehensively examine the experiences of YAs who are living with metastatic/advanced cancer. To the best of the authors' knowledge, this study is among the first to map and summarize the state of empirical data on the experiences of YAs living with metastatic/advanced cancer.
The included studies concerned a combined sample of 380 people, highlighting how few people's experiences have been studied from this largely underfunded oncology population. 7 In addition to the challenge of securing funding for YA oncology studies, the article by Knox et al. 15 highlighted some of the barriers that researchers face when conducting research with this population. For Knox et al. 15 these challenges included parents not allowing researchers to have direct contact with potential participants, YAs not returning phone calls to schedule their research interview, and potential participants not attending their scheduled interview time.
There are a number of gaps in the current state of this research and all four of the identified themes require further investigation (e.g., exploring end-of-life communication in the patient–oncologist alliance). For the purpose of this review, the authors identified four specific knowledge gaps to provide a starting point for further research. First, there is a significant gap in research surrounding the experiences of health care service delivery, limiting our understanding of how YAs experience the health care system. As the Canadian Partnership Against Cancer 7 has stated, YAs deserve age-appropriate, person-centered care. To do so, we need to address the evidence gaps, which include defining what age-appropriate care is, understanding what YA patients experience in the health care system, and identifying what these experiences mean to them. Only two studies explored the experiences of patients by investigating the patient–oncologist alliance.29,30 None explored their experiences with palliative care or other health care providers. Knox et al. 15 was the only study that explicitly cited in their results a need for YA-specific services, although they did not describe specific services that would be beneficial. Additionally, the majority of the research was conducted in the United States.23,24,26–30 It is unclear whether the experiences of YAs living with metastatic/advanced cancer in navigating and advocating for themselves within the U.S. medical system is transferable to those receiving care in diverse health systems (e.g., publicly-funded health care).
Second, another key area that warrants further research is that of relationships. No studies explored YAs' experiences with their children or their inability to have children. YA experiences in romantic relationships also were not investigated. One study indicated that some participants lived at home with their parents. 15 However, none explored relationships with parents, or the role of relationships in cancer communities between YAs with metastatic/advanced disease. As the study by Woodside et al. 31 highlighted, participants had a desire to partake in their yoga program with others. Exploring this need to connect with other YAs and identifying how other relationships are experienced would help inform the development and testing of YA psychosocial programs.
Third, it is also important to determine how interventions can be effectively delivered to YAs. With only two studies, it is evident that further research is needed that will select, tailor, and test interventions to improve the quality of life and well-being for YAs living with a metastatic/advanced diagnosis. Finally, it is imperative that researchers in this area explore and elucidate how sociodemographics (i.e., sex, geography, gender, race, socioeconomic status, and sexual orientation) influence the experiences of this population. These studies focused predominately on the experiences of white people26–30 or the race(s) of their participants were not indicated.15,23–25,31 None of the included studies collected demographic data on the sexual orientation of their participants. Our personal identities shape and influence our worldview and experiences. Understanding how sociodemographic factors influence YAs experiences could help us better understand and meet their needs. This knowledge is imperative for designing effective health policies, programs, and interventions for this population. Research related to these knowledge gaps would also provide findings that are needed to help train clinicians, who report feeling unprepared to meet the needs of this population. 33
This review offers a comprehensive overview of the empirical research on this topic, including suggestions for future research. The rigorous search conducted for relevant articles was strengthened by the inclusion of gray literature and by hand searching relevant journals. Despite the extensive search strategy used in this review and the use of two independent reviewers, it is possible that applicable research was not included. Studies that were eligible concerned the experiences of the patient [YA(s) living with metastatic/advanced cancer] with those that focused on the experiences of other key stakeholders excluded. Although a diagnosis of cancer affects more than the person with the disease, it was felt that the experiences of others (partners, parents, health care providers, children, friends and other people involved in the family life or care of the patient) represent separate research questions that need to be explored in further research. Additionally, by including only English-language studies, it is possible that this limited the research included in the review.
Conclusion
The body of empirical knowledge around the experiences of YAs living with metastatic/advanced cancer is scarce. Of the articles retrieved in this review's search strategy, few were eligible and those that were included explored a wide range of personal and interpersonal experiences. The included studies were summarized and four knowledge gaps were highlighted. These can serve as a starting point for future reviews and primary research.
Footnotes
Acknowledgments
Author Disclosure Statement
No competing financial interests exist.
Funding Information
E.K.D. is a Killam Laureate whose doctoral work is supported by the Nova Scotia Research and Innovation Graduate Scholarship and the Department of Surgery, Faculty of Health and Faculty of Graduate Studies at Dalhousie University. She is a trainee in the Cancer Research Training Program of the Beatrice Hunter Cancer Research Institute, with funds provided by the Terry Fox Research Institute and the GIVETOLIVE Donald Francis MacDougall, PhD award.