
Abstract
Although a cancer diagnosis during the adolescent and young adult (AYA) years is a traumatic event, and psychiatric disorders generally manifest during the AYA period, the impact of a cancer diagnosis on long-term mental health outcomes in this population is not well characterized. We conducted a systematic review and meta-analysis to determine if survivors of AYA cancers are more likely to develop psychiatric disorders. A systematic literature search of five databases, MEDLINE, CINAHL, Web of Science, EMBASE, and PsycINFO, was conducted from their inception to November 2018. The outcome measures were psychiatric disorders as per the Diagnostic Statistical Manual criteria, or psychiatric medication use. Study eligibility, appraisal, and data abstraction were independently conducted by two reviewers. Of 7934 total studies, four met eligibility criteria for the systematic review, three of which were included in the meta-analysis. Compared to cancer-free controls, survivors were at an elevated risk of mood disorders (odds ratio [OR] 1.36; 95% CI 1.19–1.55) and anxiety disorders (OR 1.16; 95% CI 1.05–1.28), but not substance-related disorders, (OR 0.88; 95% CI 0.63–1.22). The most commonly identified risk factors were the female sex and older age at diagnosis. We found higher odds of anxiety and mood disorders in AYA-onset cancer survivors. However, few AYA-specific studies currently exist that analyze psychiatric disorders using consistent and standardized methods. Additional studies confirming these findings are warranted.
Introduction
With increasing cure rates, a large number of adolescents and young adults (AYA) with cancer now achieve long-term survival. 1 As a sequelae of the disease and its treatment, these survivors are at risk of both physical and mental health-related late effects. 2 While research studying physical health challenges in AYA-onset cancer survivors continues to advance, a clear understanding of adverse long-term mental health outcomes in this group is still limited.3,4
Majority of the past literature has shown that an AYA cancer diagnosis can increase distress, negatively impact body image, and relationships with loved ones during a critical period of development.5,6 Although psychosocial issues have been explored more extensively, studies on psychiatric disorders in AYA-onset cancer survivors are scarce. Some studies have predominantly reported an elevated frequency of depression, 7 anxiety and posttraumatic stress disorders (PTSD) 8 along with drug abuse5,9,10 in pediatric cancer survivors, which also includes individuals from the AYA age group. It is plausible that acute psychosocial dysfunctions may lead to more severe, long-term psychiatric conditions in this young population. However, the literature has never been formally reviewed.
Therefore, the primary objective of this systematic review was to determine if there is an increased likelihood of psychiatric disorders in AYA-onset cancer survivors. The secondary objective was to identify any demographic, disease or treatment-related variables associated with psychiatric disorders in these survivors. Previously, older age in the pediatric cancer survivors has been linked to drug abuse 9 and female survivors have been reported to be at a higher risk of anxiety and mood disorders.11,12 A meta-analysis was also conducted with the relevant data, wherever appropriate.
Methods
This review followed the PRISMA framework (Appendix 1).
Search strategy
A MEDLINE (Ovid) search strategy was developed and is shown in Appendix 2. Similar strategies were used to search additional databases: Cumulative Index to Nursing and Allied Health Literature (CINAHL), Web of Science, Excerpta Medica Database (EMBASE), and PsycINFO. Each database was searched from inception to November 2018.
Study eligibility/search criteria
Inclusion and exclusion criteria were defined a priori. Inclusion criteria consisted of (1) survivors of any cancer diagnosed between the ages of 15 and 39; (2) outcome of a psychiatric disorder that fell into at least one of the three general categories indicated in the Diagnostic Statistical Manual (DSM-5 or earlier versions) 13 or International Classification of Diseases (ICD-11 or earlier versions as DSM uses the same codes), 14 substance-related disorders, mood/affective disorders, or anxiety disorders. These three psychiatric disorder categories were picked as they are the most commonly reported disorders in AYA-onset cancer survivors. All disorders identified to be a part of the above three umbrella categories were included in this study; and (3) only studies published in English were included. Besides the three main criteria for inclusion, studies looking at psychiatric medication usage were also included. The use of psychiatric medication was considered a proxy for psychiatric disorders.
Exclusion criteria for studies included the following: (1) mental health measures using tools that were not validated against the DSM criteria; (2) case reports, editorials, letters, book chapters, guidelines, commentaries, dissertations, and conference abstracts; and (3) sample size of less than 40 total AYA.
Study eligibility was determined independently by two reviewers with agreement measured using the kappa statistic. The disagreements were resolved through discussion.
Data abstraction
Two reviewers abstracted study data independently. Variables included (1) country of study (2) diagnosis years (3) type of study (4) sample size (5) anxiety/mood-affective/substance-related disorders with corresponding measurement methods and measures of risk, and (6) any demographic-, treatment-, or disease-related predictors linked to psychiatric disorders.
Critical appraisal
Potential study biases were assessed using a modified version of the Joanna Briggs Institute critical appraisal tool for Prevalence and Cohort studies checklist. 15 This tool evaluated study quality, bias, adequacy of sample size, and methodologic rigor (Appendix 3).
Meta-analysis
Studies were included in the meta-analysis based on whether a measure of association (most often odds ratio) comparing survivors of AYA cancer to controls could be extracted. Since there were a limited number of studies that explored psychiatric disorders in the AYA survivors, we ultimately decided to pool together all cancer-free controls whether they were siblings or population controls. A random-effects meta-analysis model was used to combine study data in Review Manager 5.3 (RevMan). The random-effects model was utilized to take into account any study heterogeneity both within and between studies. Heterogeneity within groups was assessed using the I2 statistic. Odds ratios reported in each study were grouped in RevMan by the three categories of psychiatric disorders. Significance was defined as p < 0.05.
Results
Study characteristics and quality of included studies
A flow diagram illustrating study selection can be seen in Figure 1. First, all internal and external duplicates were identified and removed (N = 2264). Out of 7934 total studies, four met this study's inclusion criteria. The kappa measure of agreement between the two reviewers was 0.74 (95% CI 0.64–0.84) which indicated substantial agreement. Characteristics of the four included studies can be seen in Table 1. Collectively, the substance abuse disorders that were analyzed as part of these studies included alcohol, cannabinoid, and tobacco abuse, along with disorders due to the usage of opioids, sedatives, cocaine, hallucinogens, and psychoactive medications. Mood/affective disorders that were assessed as part of the included studies were depressive disorders, bipolar disorders, manic episodes, and mood disorders. Anxiety disorders explored by the included studies were anxiety episodes, neurotic, dissociative, obsessive compulsive disorders, and stress/adjustment disorders.
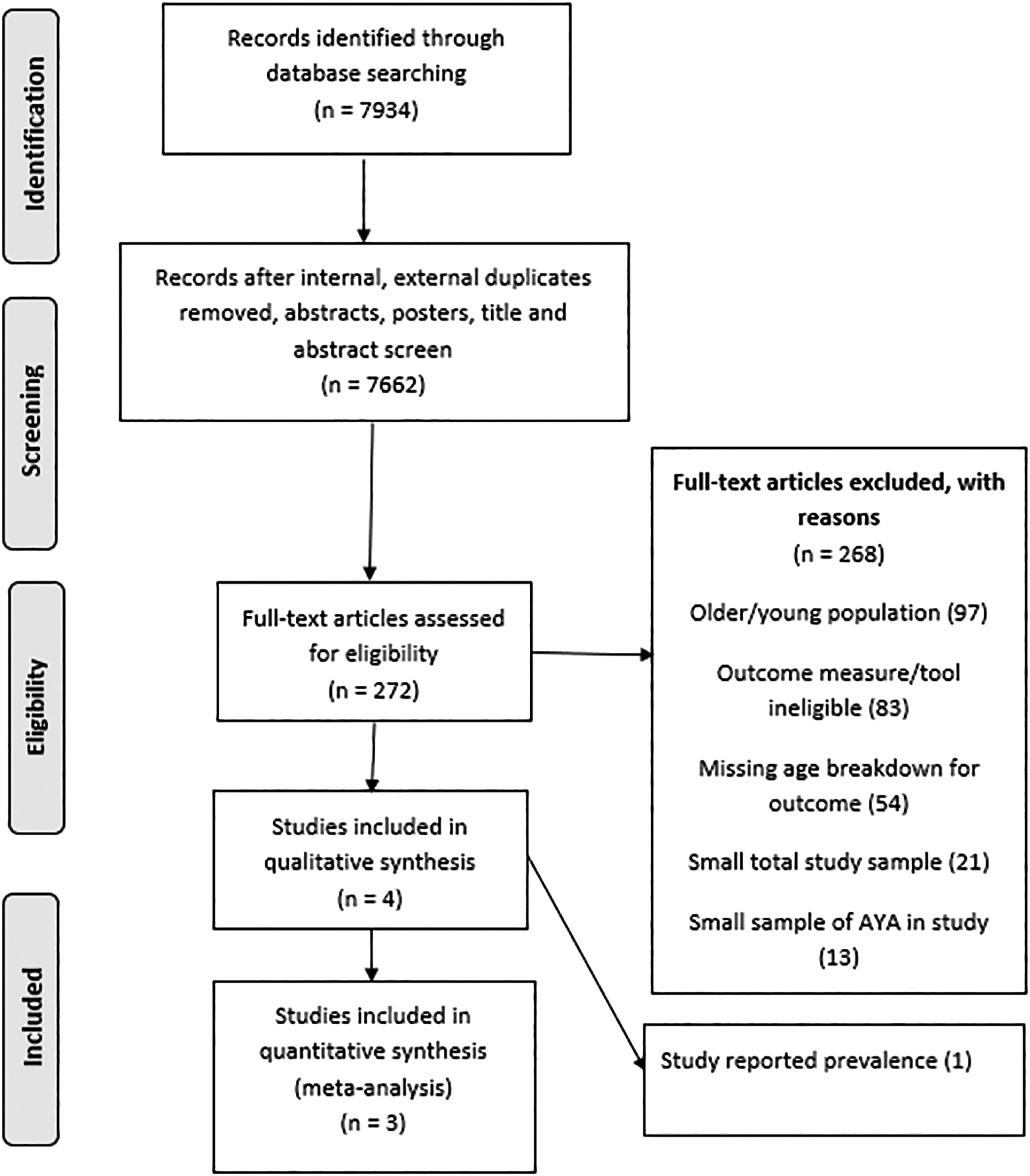
PRISMA diagram.
Characteristics and Extracted Data from Included Studies in Systematic Review
dx, diagnosis.
Ahomaki et al. compared the risk of psychiatric disorders in 5-year male and female survivors compared to cancer-free siblings. 12 This article provided data broken down by cancer diagnosis for each of the three psychiatric disorder categories being analyzed, which we then extracted. There was a relatively low number of psychiatric disorders (<10%) observed within cancer survivors out of the total sample size. Assuming a rare disease assumption for reported risk, the data presented in table 4 were entered separately into our meta-analysis. This allowed us to derive a pooled odds estimate of psychiatric disorders. Although Ahomaki et al. also reported data for individuals younger than 20 years of age at diagnosis, these data were not included in our AYA-specific cohort review.
Deyell et al. described the likelihood of antidepressant usage in 5-year survivors of AYA cancers compared to population controls. 11 Antidepressant usage was considered a proxy for depression, which therefore fell into the category of mood/affective disorders. The study reported combined data on individuals diagnosed when younger than 25 years of age. Only the data for 15–25-year-old individuals diagnosed during the AYA age range (obtained from the study authors directly) was included in this meta-analysis. Dieluweit et al. described psychotropic medication usage for anxiety-disorders in 5-year AYA-onset cancer survivors, although a breakdown of the medications considered was not provided. 16 This study reported an odds ratio that was grouped in the category of anxiety disorders, and was therefore included in the meta-analysis. Another study by Recklitis et al. reported prevalence among 3-year survivors, but since an odds ratio could not be computed with the reported data, this study was only considered in the systematic review. 17
Study quality was regarded as very good. Using the modified Joanna Briggs critical appraisal tool, all four studies received the highest possible score of 10, likely reflecting our strict inclusion criteria.
Findings by categories of psychiatric disorders
Mood/Affective disorder studies
Three studies looked at mood or affective disorders in 5-year survivors, with one analyzing only the prevalence of depressive disorders. Ahomaki et al. reported the incidence of mood disorders based on the type of cancer malignancy in individuals diagnosed at 20–34 years of age. 12 When compared to siblings, increased odds of mood disorders were seen in survivors of the following AYA cancers: central nervous system (CNS) malignancy, Hodgkin lymphoma (HL), non-Hodgkin lymphoma (NHL), and soft tissue sarcoma (Table 2). The other included study by Deyell et al., examined the incidence of depression in a Canadian AYA population as measured by antidepressant use. Although antidepressants can be administered for a wide range of disorders, they are more commonly prescribed for depressive and anxiety disorders. The study states that there is a strong association between prescription of multiple antidepressants and major depression. There was an elevated likelihood of antidepressant usage in cancer survivors, with an odds ratio of 1.23 (95% CI 1.1–1.4). 11
Predictors of Psychiatric Disorders in Adolescent and Young Adult by Demographic-, Disease-, and Treatment-Related Predictors
Bolded text indicates significant predictors.
AYA, adolescent and young adult
The study by Recklitis et al. was included in the systematic review but not in the meta-analysis, which reported on the prevalence of mood/affective disorders among a sample of 247, 3-year cancer survivors. 17 Although patients in this study could have been aged 0–37 years at the time of cancer diagnosis, 68% of the sample was between 15–37 years at the time of their diagnosis, and thus met our inclusion criteria. In the study population, 17.8% of the sample had clinical mood disorders based on the DSM criteria. 17 The reason for exclusion was due to the fact that an odds ratio could not be calculated from the information provided.
Anxiety disorder studies
Two studies in the review and meta-analysis assessed anxiety disorders in 5-year survivors. Ahomaki et al. did not find an increased risk of anxiety disorders in any specific cancer type. 12 By contrast, Dieluweit et al. found an elevated use of psychotropic medications in their population related to anxiety disorders (OR 1.15, 95% CI 1.03–1.28). 16 The list of psychotropic medications analyzed were not disclosed in the study.
Substance-related disorder studies
Ahomaki et al. reported on substance-related disorders in the AYA survivor cohort. 12 Due to the multiple statistics reported in the article of Ahomaki et al. separated by cancer malignancy, the meta-analysis allowed us to derive an overall estimate for substance-related disorders. The substance disorders that were analyzed in the study considered alcohol, opioids, cannabinoids, sedatives, cocaine, stimulants, hallucinogens, tobacco, volatile, and psychoactive substances. Only survivors of testicular cancers were at an increased likelihood of substance-related disorders, with an HR of 1.9 (95% CI 1.3–2.8).
Meta-analysis
The combined malignancy-specific results reported by Ahomaki et al. did not reveal an increased risk of substance-related disorders (Fig. 2). The OR was 0.88 (95% CI 0.63–1.22, I2 = 78%).
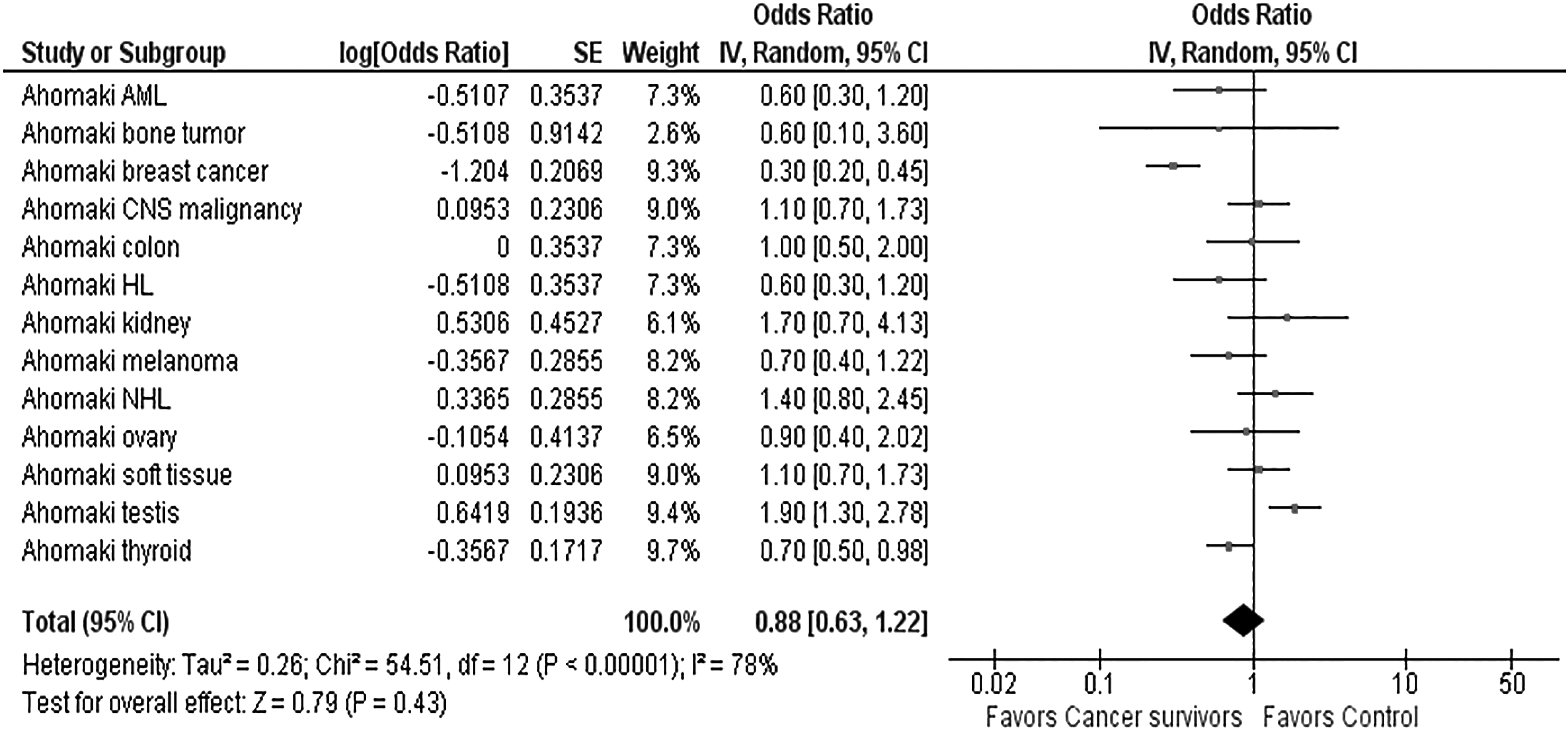
Forest plot showing substance-related disorders in AYA-onset cancer survivors using a random-effects model. AYA, adolescent and young adult.
Pooling results across three studies demonstrated an overall increased risk of mood/affective disorders (OR 1.36; 95% CI 1.19–1.55, I2 = 31%) and anxiety disorders (OR 1.16; 95% CI 1.05–1.28, I2 = 0%) among survivors of AYA-onset cancer (Figs. 3 and 4, respectively).

Forest plot showing mood/affective disorders in AYA-onset cancer survivors using a random-effects model.
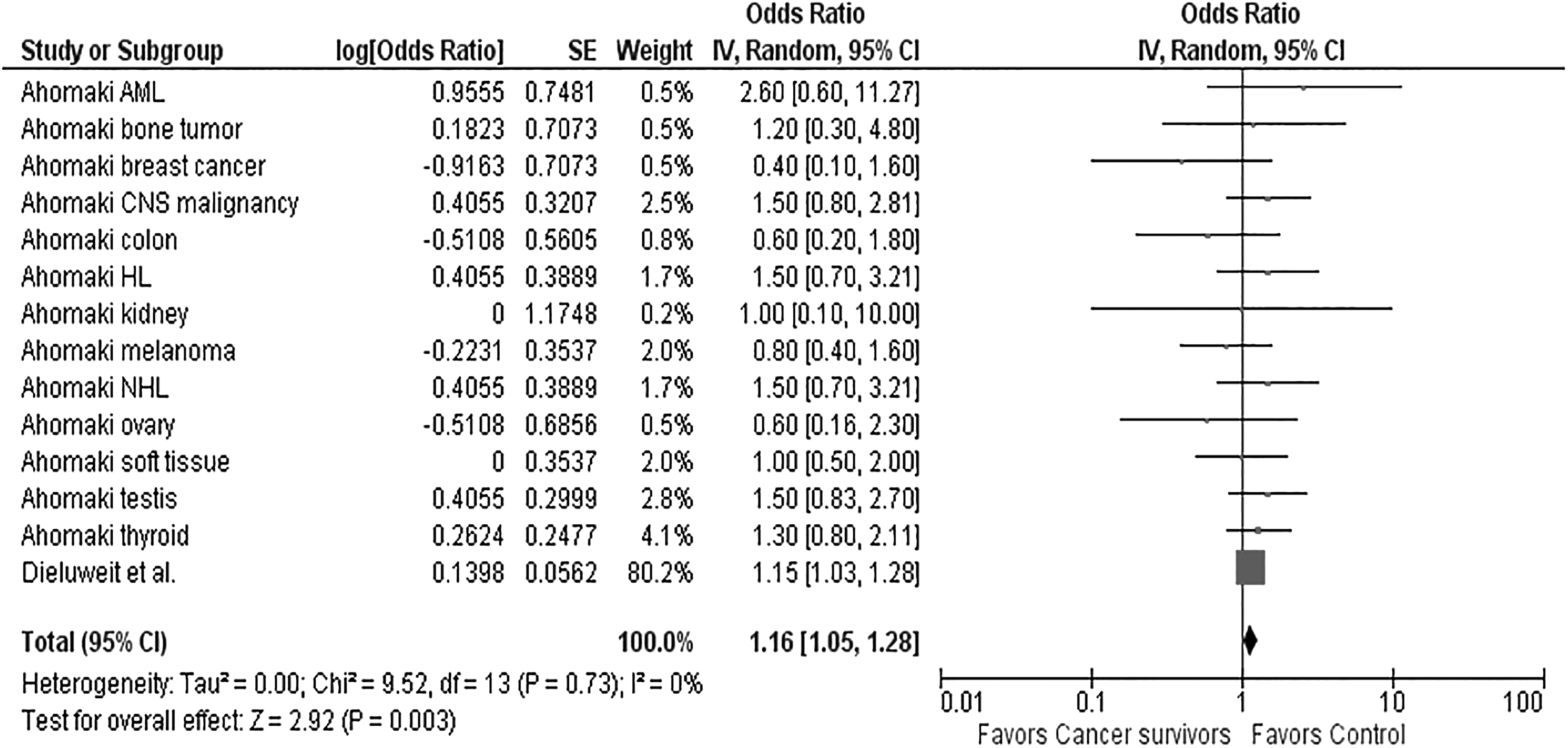
Forest plot showing anxiety disorders in AYA-onset cancer survivors using a random-effects model.
Predictor variables of adverse outcomes
Three of the included studies examined potential predictors of psychiatric disorders. The most consistently identified risk factors were the female sex and older age at diagnosis (Table 2). Treatment era of 1975–1984 in females was also associated with an increased risk of anxiety disorders (HR 1.6; 95% CI 1.2–2.1) in the study by Ahomaki at al. 12 Rurality was not shown to be a predictor of psychiatric disorders. 11 Both Deyell et al. 11 and Ahomaki et al. 12 examined potential associations with specific treatment modalities; neither found any significant association.
Discussion
Only a small number of studies have addressed psychiatric late effects using the DSM or drug usage in AYA-onset cancer survivors rigorously. This is despite the population being at significant theoretical risk, as many mood, anxiety, and substance-related disorders have their onset in the adolescent and young adulthood period.18–20
Our study findings indicated that AYA cancer survivors are at an increased risk of mood (OR 1.36; 95% CI 1.19–1.55) and anxiety disorders (OR 1.16; 95% CI 1.05–1.28), but not necessarily substance-related disorders (OR 0.88; 95% CI 0.63–1.22). The synthesis of data revealed that there was little to no heterogeneity in the mood/affective and anxiety disorder categories. However, high heterogeneity was noted in the category of substance-related disorders. High heterogeneity, despite the results coming from the same study, could potentially be due to random variation within the study itself, or true variance between different cancer malignancies.
A 17.8% prevalence of mood disorders was found in one study of 3-year AYA cancer survivors, which was included into the systematic review but not the meta-analysis. In the general population, mood disorders in AYA cohorts range from 8.7% to 11.3%. 21 In addition, a narrative component to identify predictors of psychiatric disorders showed that females and those older at cancer diagnosis may be at a higher risk for anxiety and mood disorders. It should be noted, however, that females generally report higher rate of mental health care concerns compared to males. 22
The findings seem to confirm observations made in previous studies, although often the AYA patients studied have been clustered together with the pediatric or older adult cohorts. For example, the Childhood Cancer Survivor Study (CCSS) included some individuals diagnosed during the AYA years, and found that the risk of PTSD was higher in individuals with bone cancer, CNS cancers, HL/NHL, leukemia, soft tissue sarcoma, and neuroblastoma compared to sibling controls. 8 The highest risk groups were those with HL (OR 4.64, p < 0.01), NHL (OR 4.08, p < 0.01), or acute leukemia (OR 3.84, p < 0.01). 8 In another study consisting of 5-year adult-onset cancer survivors diagnosed after 18 years of age, individuals reported higher anxiety disorders on a diagnostic interview based on the DSM-4 criteria (OR 1.49, 95% CI 1.04–2.13). 23
However, no increased likelihood of substance-related disorders was discovered in survivors included in our analysis. In the past, some studies have looked at AYA substance abuse with studies conducted using self-reported questionnaires. In a study by Milam et al., higher self-reported depressive symptoms were related to increased cannabis use in those diagnosed when 21 years or younger. 24 Another CCSS study reported emotional distress to be increased in those cancer survivors who began alcohol consumption at younger than 18 years of age. 10 However, as both studies consisted mainly of pediatric cancer patients, the generalizability of these findings to AYA-onset cancer survivors is unknown. This is emblematic of the suboptimal representation of AYA populations or the lack of AYA-stratified data in cancer survivor cohort studies.
This review and meta-analysis had several strengths. One is that the study data came from cross-sectional or cohort studies, using objective measures in the identification of psychiatric disorders and without the known limitations of self-reported data. This allowed for selection biases to be minimized. In addition, as these cohort studies were large in number, the interpretation of the overall effects was done with greater confidence.
There were also some clear challenges since very few studies met our inclusion criteria, due, in large part, to the paucity of AYA-specific data as noted above. The majority of study data came from Ahomaki et al., which used sibling controls. This may underestimate the true risk in survivors as siblings may also have elevated levels of distress compared to general population controls. 25 Furthermore, two of the included studies found an elevated risk of mood and anxiety disorders in older AYA as indicated by psychotropic medication usage. Although this may reflect true elevated risk, it may also reflect different prescribing patterns of psychotropic medications. For example, physicians may be less likely to prescribe selective serotonin reuptake inhibitors to younger AYA, given concerns about suicide risk in younger populations. 26 In addition, studies using psychotropic medications as proxies for anxiety may capture use for alternative indications, including sleep difficulties, neuropathic pain, and migraines. Such misclassification is likely rare: a CCSS report found that among cancer survivors prescribed psychotropic medications, almost 70% had either anxiety or depression. 27 These limitations further validate the great need for future studies involving the AYA.
In addition, many studies did not measure psychiatric disorders using standardized methodologies or used tools with different cutoff scores, making consistent comparisons between studies impossible. Several studies identified by our search strategy described self-reported tools that did not encompass all DSM criteria and thus did not capture a reliable measurement of true psychiatric disorders.. Those studies that involved a larger number of AYA-onset survivors were predominantly psychosocial in nature. Standardization of methods to analyze psychiatric disorders is therefore a key in this population in addition to the already existing studies on psychosocial distress. Furthermore, we only included studies in English which would have limited our scope to capture important studies published in different languages. Other articles were excluded for reasons such as a small AYA sample size or missing age breakdowns for the study population. Finally, as all of the studies captured in this systematic review were conducted in developed countries, the generalizability to AYA cancer survivors in low- and middle-income countries is unknown.
Conclusion
In AYA-onset cancer survivors, mood and anxiety disorders are more likely to occur compared to cancer-free control populations, although further research is needed to confirm these results. Our findings have several notable implications. For researchers, it is essential to note that measurements of psychiatric outcomes need to be standardized to allow proper comparisons between studies. For health care professionals as well as policymakers, survivorship guidelines may need to include screening methods for psychiatric disorders. This is especially true for AYA cancer survivors who are recognized to be high-risk subgroups. Finally, studies examining whether psychosocial resources both during and following cancer treatment can mitigate the increased risk of psychiatric conditions are merited.
Footnotes
Acknowledgments
I thank all authors who have taken the time to answer article-specific questions. R.D.'s salary was supported by a grant from the Canadian Cancer Society Research Institute.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by a grant from the Canadian Cancer Society Research Institute.
Appendix
Critical Appraisal Checklist Based on Joanna Briggs Institute Checklist
| Question | Yes(1)/No (0) |
|---|---|
| 1. Was the sample frame appropriate to address the target population? | |
| 2. Were study participants sampled in an appropriate way? | |
| 3. Was the sample size adequate? | |
| 4. Were the study subjects and the setting described in detail? | |
| 5. Was the data analysis conducted with sufficient coverage of the identified sample? | |
| 6. Were valid methods used for the identification of the condition? | |
| 7. Was the condition measured in a standard, reliable way for all participants? | |
| 8. Was the follow-up time reported and sufficient to be long enough for outcomes to occur? | |
| 9. Was there appropriate statistical analysis? | |
| 10. Was the response rate adequate, and if not, was the low response rate managed appropriately? | |
|
|