
Abstract
Adolescent and young adult (AYA) cancer survivors, here defined as individuals diagnosed with cancer between 15 and 39 years of age, are at high risk for adverse late-term metabolic effects of treatment through adulthood. Diet is a modifiable lifestyle behavior that may improve metabolic health outcomes in AYA cancer survivors. However, the details of dietary interventions for this unique population remain largely undescribed. In this systematic review, we aim to synthesize the results of dietary interventions for adult AYA cancer survivors. Seven databases and clinical trial registries were searched in March 2019 for interventions targeting dietary behaviors in AYA cancer survivors (PROPSERO systematic review number: CRD42019126376). Descriptive statistics and a narrative synthesis were completed to detail intervention participants and components. After full text review of 233 studies, four studies met all inclusion criteria. All studies were heterogeneous for participant age, cancer type, and duration, and were designed for feasibility and preliminary efficacy. Included studies followed different dietary guidance; however, each resulted in a significant change on a primary outcome of either dietary quality or body composition. Three of the four studies included a theoretical framework, where self-efficacy was a central construct. Counseling, in person, telephone, or electronic, provided behavioral support. Results of this systematic review suggest high potential to change dietary behaviors in AYA, but interventions remain limited. AYA cancer survivors demonstrate unique physiological and psychosocial needs, and future interventions designed to address this care gap should be targeted for this population with consideration of social support, delivery mode, and individual tailoring.
Introduction
Adolescent and young adult (AYA) cancer survivors are a rapidly growing population in the United States (US) and globally, with survival rates greater than 80%, largely resulting from improved cancer treatments.1–3 In the US, AYA cancer survivors are defined as those diagnosed with cancer at ages 15–19 for adolescents, 20–24 for early young adults, and 25–39 for young adults. 4 Annually, in the US, there are ∼70,000 new AYA cancer cases, accounting for 5% of all cancer diagnoses. 5 Cancer type and incidence vary by age in AYA. Among individuals 15–24 years of age, leukemia, lymphoma, testicular, and thyroid cancers are the most common cancer diagnoses, while melanoma, breast, colorectal, and uterine/cervical cancers are the most common among individuals 25–39 years of age.1,5
The developmental life stages that comprise the AYA age range are marked by unique physiological and psychosocial changes, making AYA cancer survivors a distinct at-risk population with needs different than those of older adult cancer survivors. AYA cancer survivors are at high risk for experiencing late-term metabolic effects of treatment resulting in higher rates of, and earlier age of, onset for cardiovascular disease, diabetes, and metabolic syndrome, as well as secondary cancer diagnoses.6–10 There has been little improvement in these trends in recent years.11,12
These comorbid conditions experienced after cancer treatment are associated with lower quality of life, higher financial burden, and greater mortality risk, 13 and social support may play an important role in health outcomes for this at-risk population. 14 Efforts to identify modifiable risk factors that can translate to effective lifestyle interventions that alter the trajectory of comorbidity after AYA cancer are therefore essential.
Diet remains a leading modifiable health behavior with significant potential to attenuate the cascade of metabolic comorbidities that are commonly present in AYA cancer survivors. Among adult cancer survivors, previous epidemiological evidence has shown that dietary intake patterns high in vegetables, fruits, and whole grains, and low in red and processed meats, refined carbohydrates, and saturated fat, are associated with lower cancer mortality. 15 Furthermore, evidence persists that adherence to high quality dietary patterns is associated with improved quality of life after treatment. 16 However, these dietary patterns are not always attained in cancer survivors, with fewer than 20% of adult cancer survivors meeting current cancer-preventive dietary recommendations. 17
Previous dietary interventions for adult cancer survivors have demonstrated favorable modulation of weight, metabolic biomarkers, and quality of life.18–20 Rigorous epidemiological evidence of adherence to cancer preventive dietary patterns in AYA is limited. Approximately 80% of adult survivors of AYA cancer report low fruit and vegetable intake. 21 Among AYA-aged survivors of childhood cancers, reported intake of fruits, vegetables, and fiber remains below recommendations.22,23 Poor dietary intake among AYA cancer survivors indicates the need for interventions that are targeted to this population with unique survivorship needs. Although lifestyle interventions in childhood or adolescent cancer survivors have been described in previous systematic reviews,24–26 details of dietary interventions in both AYA cancer survivors have yet to be systematically evaluated.
AYA cancer survivors embody a distinct period of the human lifecycle marked by physiological maturation, emergence into independence, and pursuit of social relationships and career goals. 27 Understanding the effect of dietary interventions on health behaviors in AYA cancer survivors is essential to optimize the health outcomes of AYA cancer survivors long term. In this study, we build on the available evidence to systematically review current approaches, including an evaluation of intervention modality and use of theory, implemented in intervention studies designed to change dietary behaviors in AYA cancer survivors.
Research objectives
The purpose of this systematic review was to delineate dietary intervention studies conducted to support diet behavior change to meet current dietary guidelines for adult survivors of AYA cancer. 28 We describe the degree of dietary behavior change achieved and explicate effect on outcomes such as chronic disease, metabolic biomarkers, and/or quality of life in AYA survivors. In addition, we aimed to determine what delivery modalities were employed as well as what behavioral theories or theoretical constructs were included in such interventions. Furthermore, using narrative synthesis, we aim to improve understanding of influencing factors related to dietary intervention effectiveness.
Methods
Following the recommendations outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses, 29 we developed a study protocol for this review, registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD42019126376, 2019).
Eligibility criteria
Studies were considered for inclusion in the systematic review only if they contained any dietary intervention for AYA cancer survivors, including, but not limited to the following: food, diet, dietary patterns, nutrition behaviors, meal preparation or cooking, menu planning or preparation, and nutritional counseling or coaching. Studies were excluded if they were not interventional in nature or if the primary population was not cancer survivors or not within the determined age range for AYA, defined below. Studies were included if they met the following criteria:
Participants were adult survivors of any type of cancer diagnosed either as an adolescent (diagnosed at age 15–18 years) or young adult (diagnosed at age 19–39 years). Historically, enrollment of AYAs in clinical trials has potential to include mixed and highly varied age groups.
30
To address this expected heterogeneity, studies must have (a) reported that eligible and enrolled participants were between the ages of 15–39 years at cancer diagnosis; (b) stratified statistical analyses by age with a cut point, which encompassed any AYA age range; or (c) had a mean/median age of ≤45 years for the enrolled study participants. The age cut point of ≤45 years was determined and agreed upon by all study authors to best capture any young adult cancer survivor, who may have participated within 5 years of their cancer diagnosis or studies, which may have enrolled a large percent of AYA into the trial. Studies in pediatric patients and older adults were excluded. Studies were interventional in design. Specifically excluded were studies that were observational, cross-sectional, case–control, case series, or case reports, protocol articles, reviews, systematic reviews, meta-analyses, opinion pieces, letters to the editor, dissertations, or book chapters. The intervention involved food, nutrition, diet, cooking, meal preparation, or menu planning, either exclusively, or as part of a multicomponent intervention wherein data related to the dietary components could be isolated. Studies were excluded if they were trials involving only dietary supplements or medications. Outcomes such as nutrition behavior change, change in food group/nutritional intake, dietary quality, adherence/compliance, body composition, quality of life, biophysical parameters such as blood pressure, glucose, or lipids, and/or change in prevalence of non-cancer disease such as hypertension, diabetes, or cardiovascular conditions were measured and reported.
Search strategy
An information specialist (C.L.H.) searched the following databases for publications addressing dietary interventions in adult survivors of adolescent or young adult cancer: Ovid/MEDLINE; Elsevier/Embase; Wiley/Cochrane Central Register of Controlled Trials (CENTRAL); Clarivate/Web of Science (WOS); EBSCO/Cumulative Index of Nursing and Allied Health Literature (CINAHL); EBSCO/PsycInfo; EBSCO/Education Resources Information Center (ERIC); and ClinicalTrials.gov; from the dates of their inception to the dates the searches were completed, March 11–12, 2019.
Details of the full search strategy for all databases are available as Supplementary Tables S1, S2, S3, S4, S5, S6, S7, S8. There was no restriction on year published. Eligible studies must have been published in English. No age restrictions were used in the preliminary search strategy due to the various definitions and age ranges of AYA that exist in the literature. In addition, citations from relevant review articles and all initially included articles for full text review were hand searched and screened.
Study selection
All records identified through the database searches were exported to the reference management software EndNote Version X9 (Clarivate Analytics, Philadelphia, PA), which was used to document and delete duplicate records. Two reviewers (M.B.S. and J.J.M.) independently screened all titles and abstracts of retrieved references for relevance to the topic. Disagreements were resolved by consensus and consultation with the senior author (C.A.T.). Adhering to the detailed inclusion/exclusion criteria documented above, two reviewers (M.B.S. and J.J.M.) then screened the full text of those publications meeting initial title/abstract screening criteria, resolving disagreements by consensus and consultation with the senior author (C.A.T.).
Data extraction and narrative synthesis
Data from included studies were extracted through a customized REDCap [Research Electronic Data Capture] 31 web-based form and were completed independently and in duplicate by M.B.S. and J.J.M. Extracted information included participant age, cancer diagnosis, sex, study design and duration, key intervention components, including any behavioral theories or constructs, and delivery methods. Study location, additional health behaviors targeted, outcomes, and funding sources were also extracted. Corresponding authors, if required, were contacted through email by MBS to minimize missing data related to participant age at diagnosis to better characterize AYA cancer survivors in each included study.
Narrative synthesis, which aims to summarize and explain findings related to the effects of interventions as well as the factors influencing the implementation of interventions, was completed following The Guidance for Conduct of Narrative Synthesis in Systematic Reviews 32 to both synthesize results and develop a conceptual framework of intervention components. This analysis method, agreed upon by all authors before completing the searches, was chosen both as a means of handling expected study heterogeneity and as a technique to conceptually describe influencing factors of the effectiveness of dietary interventions for AYA cancer survivors.
Risk of bias and study quality assessment
Risk of bias across studies was determined following the guidelines from The Cochrane Handbook for Systematic Reviews of Interventions 33 to document potential selection, attrition, detection, or reporting bias. Studies were determined to be “low risk” (+) or “high risk” (−) for each of the seven domains specified by the Cochrane Collaboration's tool for assessing risk of bias. 22 Internal and external validity of studies were determined using a modified Downs and Black Study Quality checklist 34 to quantify study quality related to behavioral clinical trials.
To capture risk of bias within studies, 15 study quality indices were utilized: (1) the hypothesis, aim, or objective of the study was clearly described; (2) main outcomes were clearly described; (3) participant characteristics were clearly described; (4) the intervention of interest was clearly defined; (5) the main findings were clearly described; (6) characteristics of participants lost to follow-up were described; (7) probability values were reported for main outcomes; (8) statistical tests were appropriate for the main outcome; (9) statistical tests were selected a priori and any additional exploratory analysis was made clear; (10) sufficient power (or lack thereof) was described; (11) intervention compliance information was available; (12) subjects were randomized to groups; (13) subjects approached for participation were representative of target population; (14) participating participants were representative of population from which they were recruited; and (15) the main outcome measures were appropriate, valid, and reliable.
Studies received a score from 0 to 15 where the predetermined cut points of quality were considered: 0, “none”; 1–3, “very low”; 4–6, “low”; 7–9, “moderate”; 10–12, “high”; and 13–15, “very high”. All risk assessments were documented during data extraction on a separate REDCap 31 form in duplicate by M.B.S. and J.J.M. Rater agreement between M.B.S. and J.J.M. was 100% for risk of bias assessment and 96% for study quality assessment; any disagreement was resolved by a third, independent review (C.A.T.).
Results
We found 6910 records through the database searches (OvidMEDLINE-949; Cochrane Central-418; Embase-3381; WOS-1240; CINAHL-495; PsycInfo-208; ERIC-8; ClinicalTrials.gov- 211) and one additional publication was identified in the reference list of a review article. Of the 4275 publications that remained after duplicates were removed, 4042 were excluded after title and abstract review because of irrelevance to the topic (Fig. 1). Strict inclusion/exclusion criteria, as outlined above, were applied to the full text of 233 articles. Of these, the majority of full text articles did not meet age criteria, participants were a mean age of >45 years, were pediatric cancer survivors, or age during study participation or at cancer diagnosis was not defined in the study. Four studies met the full set of inclusion criteria.35–38
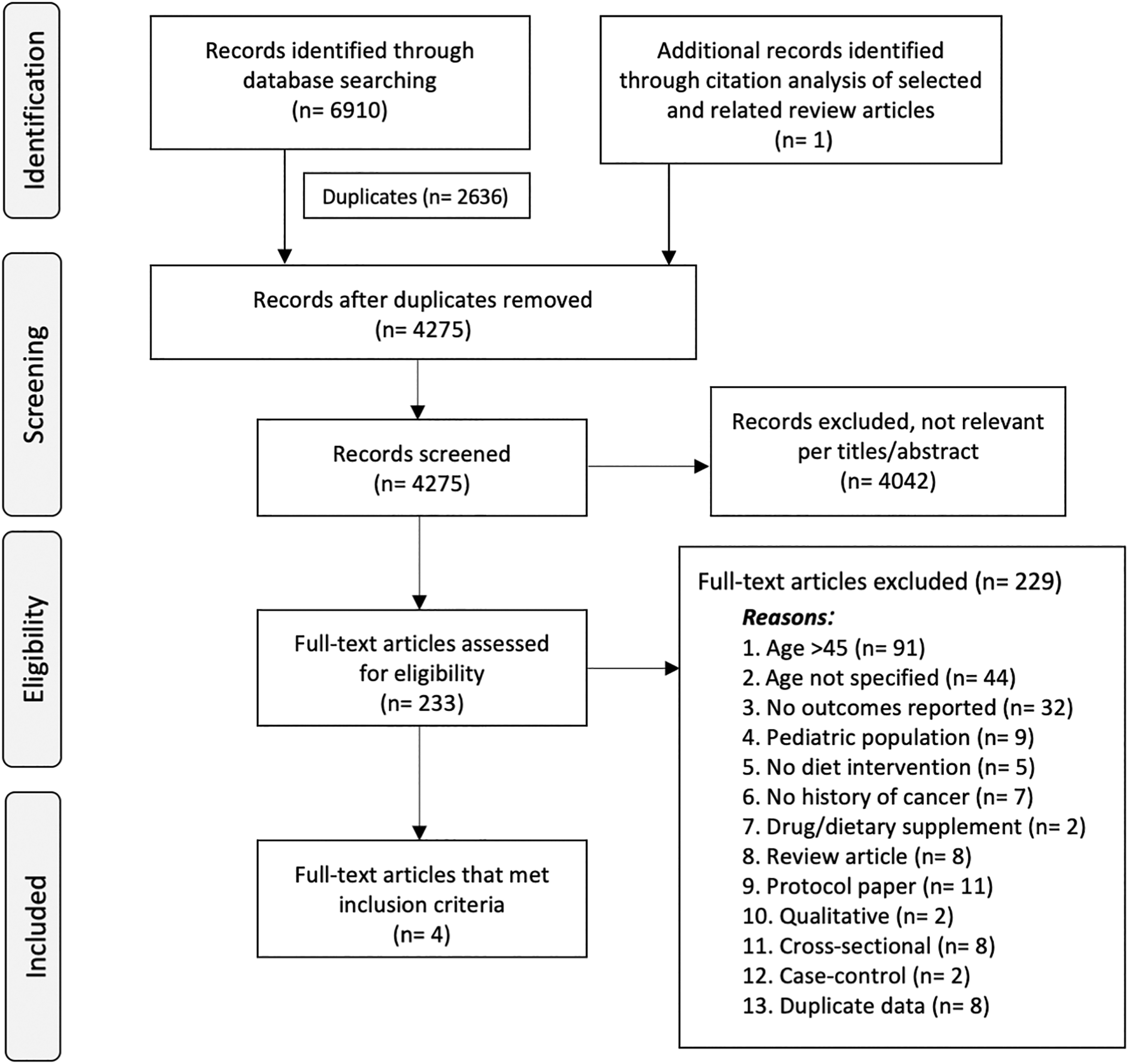
PRISMA Study Flow Diagram.
Risk of bias and quality assessment
Our assessment of risk of bias is detailed in Table 1. Two studies presented low risk of bias determined by the Cochrane Collaboration's tool for assessing risk of bias. 33 Others remained deficient in randomization, allocation concealment, and blinding. Other sources of bias identified were limited to the use of a calcium-rich diet as the control group in one study, 35 which introduced confounding that was not able to be controlled for. Modified Downs and Black Study Quality scores 34 representing study internal and external validity ranged from 9 to 15 (moderate to very high). Reduction in overall score was related to lack of randomization and limited evaluation of compliance and lost-to-follow-up.
Assessment of Study Bias of Eligible Studies (n = 4)
Key: (–): high risk of bias; (+): low risk of bias
Score ranges 0–15, with a higher score indicating higher study quality
Study characteristics and narrative synthesis of intervention components
All eligible studies were designed to assess feasibility and preliminary efficacy of various health or health behavior outcomes. Individual characteristics and descriptors of the included intervention studies are summarized in Table 2. While the included studies were limited and heterogeneous in design, each intervention did result in a significant change in at least one targeted behavioral or physiological outcome and three studies demonstrated an intervention-specific change in at least one dietary behavior. Through the results from our narrative synthesis, Figure 2 provides a proposed conceptual framework to consider when designing future dietary interventions for AYA cancer survivors, wherein external factors, population heterogeneity, and intervention components are antecedent to the feasibility and efficacy of dietary interventions in AYA cancer survivors.
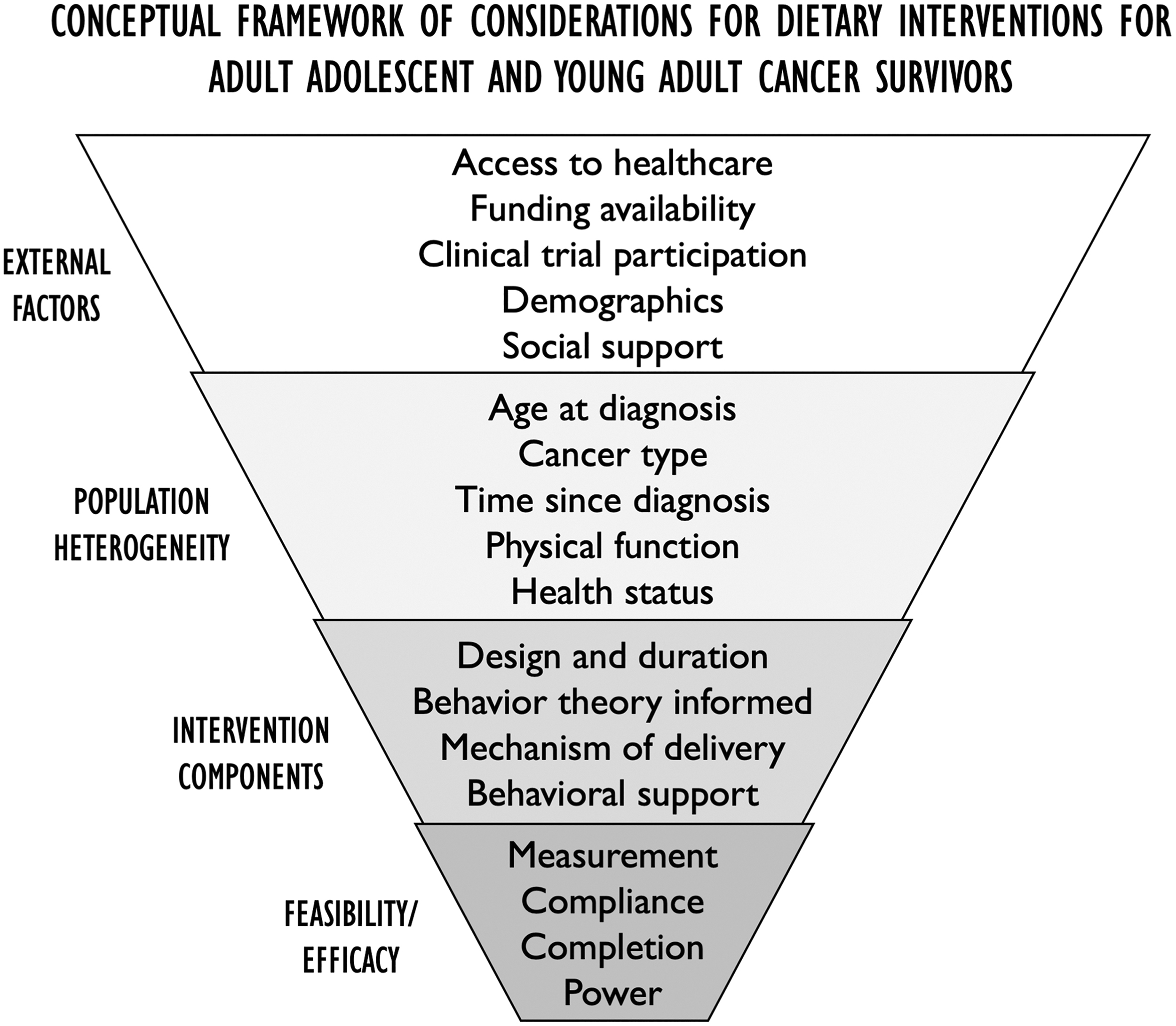
Proposed conceptual framework of four components to consider, which may inform development of dietary interventions for adult survivors of adolescent and young adult cancers, determined from narrative synthesis of included studies.
Summary of Eligible Adult Survivors of Adolescent Young Adult Cancer Dietary Intervention Studies (n = 4): Participant Characteristics, Intervention Descriptors, Measures, and Relevant Significant Findings
Outcome measurements completed at baseline, midpoint, and completion.
Outcome measurements completed at baseline and completion.
Precision Nutrition Coaching, Lean Eating (https://www.precisionnutrition.com).
AYA, Adolescent and young adult, diagnosed with cancer before 40 years of age; NR, not reported; SMS: short message service, text messaging; K-DQI, Korean Dietary Quality Index (score range 0–16, with a higher score indicating better diet quality); BMI, body mass index; MET, metabolic equivalents; HEI-EPIC, Healthy Eating Index- European Prospective Investigation into Cancer and Nutrition (score range: 0–100, with a higher score indicating better diet quality).
External factors
Half of the studies were conducted in the US and were funded by either federal or foundational grants,35,37 while the remaining half declared no funding source and were conducted internationally in South Korea 36 and Germany. 38 Lack of interest or refusal for study participation ranged between 19% and 50% of approached eligible participants. In the studies that reported participant race and ethnicity (n = 2),35,37 the majority of participants were non-Hispanic white (85%–90%). Three studies35–37 detailed the household composition of study participants, wherein the majority of participants were married and lived in homes with children (range: 70%–90% and 64%–69%, respectively). The impact of household composition or related social support was not directly measured in any of the studies.
Population heterogeneity
Enrollment of AYA cancer survivors among included studies varied, wherein AYA cancer survivors were a subgroup recruited in addition to adults outside the upper AYA age range. One study 38 was the exception, which explicitly recruited solely adult survivors of an AYA cancer diagnosis. All other interventions recruited adults younger than 50 years or premenopausal women. Sample sizes of the studies ranged from 23 to 90, with a total participant sample between all studies of 218. The majority of participants were female (87% overall).
All participants were adults at enrollment, with an age range for included survivors of 20–53 years. In the studies reviewed, the percent of participants who met the definition of AYA at diagnosis ranged from 24% to 100%. One study recruited participants undergoing adjuvant chemotherapy, 35 while three studies recruited participants who were diagnosed and had completed primary cancer treatment (time since treatment range: 5.4–48 months). Cancer diagnoses were varied, but were primarily breast cancer. Additional participant eligibility criteria varied beyond cancer diagnosis and included overweight status, 37 presence of a risk factor for cardiovascular disease, 38 or low dietary intake of fruits and/or vegetables. 36
Intervention components
The studies demonstrated similarities as well as differences in intervention design and delivery methods. Half of the studies were randomized controlled trials35,36 and the other half were single-arm pre-post studies.37,38 Study duration ranged from 12 weeks to 12 months, all with assessments at baseline and follow-up. Two studies had assessments at the halfway point in the study.35,37 All studies had ethical approval and informed consent, and participants in all trials were convenience samples recruited out of clinical cancer centers with assistance of electronic medical record screening for eligibility.
Three studies were guided by behavior theory (either Social Cognitive Theory35,37 or Trans-theoretical Model 36 ) and incorporated the following behavioral constructs into intervention design: process of change and decisional balance, 36 goal setting,36,37 self-monitoring,35,36 self-regulation, and outcome expectancy. 37 This provided a component of tailoring the interventions to the individual participant. All studies placed an emphasis on promotion of self-efficacy; however, it was only formally measured in one study. 36 Furthermore, in this study, improvement in self-efficacy was promoted through the use of adaptive educational modules within the web-based self-management exercise and diet intervention program (WSEDI) 39 determined by each participant's stage of change (e.g., precontemplation, contemplation, preparation, action, or maintenance).
All studies were considered hybrid designs, combining two or more delivery modes. Two studies were primarily telephone based with counseling,35,38 while two of the studies were primarily web based and integrated electronic health (eHealth; e.g., email and short message service [SMS] text messaging).36,37
During participation in the web-based studies, participants were asked to either complete 10–15-minute daily online lessons about health habits and goal setting related to nutrition and exercise 37 or engage weekly with a platform that included assessment, education, action planning, and feedback to enhance dietary and exercise behaviors. 36 In the studies that included eHealth components, email and SMS were used to enhance intervention adherence through reminders and feedback on goals, suggesting the potential for eHealth to provide support for nutrition behavior change in AYA cancer survivors. Three studies also included in-clinic components for anthropometric measurements35,37 or face-to-face counseling. 38
The majority of behavioral support for nutrition behavior change was provided through coaches or counselors in all studies. Lynch et al. 37 included a multifold approach to enhance support through pairing participants with a same-gender coach, frequent email reminders (both group and personalized), and incorporation of peer discussion boards. Demark-Wahnefried et al. 35 and Lee et al., 36 both reported utilization of a trained coach to facilitate dietary behavior changes, while Quidde et al. 38 involved nutrition counseling provided by a registered dietitian.
Each study followed different dietary guidelines for developing the dietary intervention for AYA cancer survivors. The similarities and differences between dietary guidelines are detailed in Table 3. Although varied, all dietary guidance emphasized consuming a variety of foods and increasing intake of fruits, vegetables, and whole grains while limiting solid dietary fats.40–43 All applied dietary guidelines integrated some component of energy balance related to diet and physical activity. Finally, three of the four studies35–37 incorporated physical activity into the intervention and included educational or supportive materials for this behavior, encompassing the synergistic effect of these lifestyle behaviors.
Summary of Dietary Guidelines and Components Used in Eligible Dietary Interventions for Adolescent and Young Adult Cancer Survivors (n = 4)
Feasibility and efficacy
All studies were designed and powered for feasibility and primary efficacy on specific outcomes. Primary outcomes were change in dietary intake35,36,38 or body weight. 37 One study demonstrated a significant increase in daily servings of fruits and vegetables, 35 another study showed a significant increase both in fruit and vegetable intake and overall dietary quality, 36 while the other study documented a significant increase in dietary quality. 38 For the one study where diet was not measured, body weight, body fat, and body mass index all significantly decreased. 37 Secondary outcomes across studies included quality of life, body composition, psychosocial indicators, metabolic biomarkers, and adherence.
Overall attrition rates in the trials ranged from 3% to 51%. In one study, age was inversely associated with study compliance, and participants who dropped out of the study were on average 4.9 years younger than study completers. 35 In a study that included both men and women, 37 men were significantly younger than women; however, women were more likely to complete the intervention than men. Loss of study interest was a common reason for study discontinuation. 35 Other commonly reported reasons for participant dropout or lost to follow-up in studies were related to a lack of time. Participants reported time commitments to work and family, 37 balancing work and family obligations, 38 and general busyness 36 as reasons for discontinuing participation.
Discussion
The aim of this systematic review was to describe the current evidence regarding dietary interventions delivered to AYA cancer survivors. Our search results yielded four studies that met our inclusion criteria. The main findings from these studies suggested that external factors, population heterogeneity, intervention-relevant components (e.g., behavioral theory and delivery modality), as well as feasibility and efficacy are key considerations when delivering interventions to AYA cancer survivors to promote healthy dietary behaviors. Outcomes from three included studies showed a positive effect on behavior change, despite poor dietary intake at baseline reflective of current estimates of AYA cancer survivors' dietary intake after treatment.21,44
Our results highlight the paucity of both targeted and tailored dietary interventions for AYA cancer survivors reported in published literature, as well as the lack of specific outcome data related to dietary influences on metabolic health and quality of life after an AYA cancer diagnosis. Lifestyle interventions targeted for adult AYA cancer survivors are increasingly relevant as the incidence rates of early-onset cancers continue to increase, and mortality rates from breast, lung, and colorectal cancer are on the rise in young adults. 45
AYA cancer survivors have an average estimated 25–45 years of lifespan remaining after treatment. 46 Therefore, developing healthy dietary habits that can last a lifetime remains critically important. It remains possible that the low prevalence of dietary interventions for AYA cancer survivors included in this systematic review is influenced by the historically lower enrollment of AYAs in clinical trials. 47 The majority of included participants were breast cancer survivors. The current gap in addressing late effects in AYA cancer survivors through diet was emphasized by the fact that most studies were excluded from our review based on a recruitment focused on adults (>45 years of age) diagnosed with cancer at a later age.
Despite improved survival rates overall for AYA cancer survivors, survival disparities persist among minority racial/ethnic groups and those of lower socioeconomic status. 48 The majority of participants detailed in our included studies were white and well educated, further highlighting the need for culturally appropriate and cost-effective interventions of diverse samples.
Three of the four included studies formally assessed dietary intake. Those that did measure dietary intake evaluated using different diet scores or dietary components, thus limiting across-study comparisons. Within all the studies included in our review, nutrition education and counseling were utilized to promote dietary change. Furthermore, nutrition coaching and counseling provided individualized tailoring of the interventions through goal setting and feedback on progress. Education and counseling provide participant access to resources and tools, collaborative development of new skills and habits, acquisition of health information, and social connection, all of which have been considered facilitators to achieving healthy dietary behaviors in AYA cancer survivors. 49 Nutrition education and counseling present as crucial components of future research efforts to promote healthy dietary behaviors in AYA cancer survivors.
Notably, the studies included in this systematic review employed behavioral theories in dietary intervention planning and measurement, including Social Cognitive Theory and the Trans-theoretical Model. Behavioral theory provides a framework during study design and evaluation for understanding mediators of intervention effectiveness and studies including behavioral theory are considered more rigorous scientifically than those that do not.50,51 In addition, theory-based lifestyle interventions support positive health behavior changes and maintenance in adult cancer survivors, 52 and often improve intervention adherence. 53
Self-efficacy, which was a central construct in the three studies with formative behavior theories, is related to maintenance of health behaviors for cancer survivors postlifestyle interventions. 54 In the included studies that collected demographic information, the majority of participants reported being married and residing in homes with children, providing an element of external social support. Literature has previously reported that familial relationships are associated with dietary quality, 22 yet none of the studies included in this review utilized a family- or dyad-based approach. Other qualitative research has indicated that interventions for AYA cancer survivors should give consideration to family and work obligations, be convenient, and provide social support. 55
Furthermore, social support has been reported to be a catalyst of changing health behaviors and improving self-efficacy. 56 Social support was not measured in any of the included studies, while self-efficacy was formally measured in only one study. Interventions may benefit from the promotion of self-efficacy as well as integrated social support through both the inclusion of behavior theory during the development stages and design elements such as tailoring and dyad- or family-based approaches.
In terms of intervention delivery modality, a survey of AYA cancer survivors reported that 92% were using the internet to seek diet and physical activity health information, 57 and previous semistructured interviews with AYA cancer survivors identified a preference for remote-delivered lifestyle interventions compared to face-to-face interventions. 55 While only two of the studies in this systematic review included eHealth to engage AYA cancer survivors, eHealth was used as a means to change habits and provide information. This may be particularly relevant to interventions for cancer survivors younger than 45 years, who are more likely to use mobile technologies than older cancer survivors. 58
Beyond diet, digitally delivered interventions for other health behaviors such as physical activity, substance use, and medication adherence, as well as psychosocial and symptom management, have been evaluated in AYA cancer survivors.59,60 These interventions tested a variety of digital formats, including websites, mobile applications, and social media. Although participant response was generally positive, intervention effects were not clearly demonstrated. These findings, in combination with our own, propose that there is an ideal balance of frequency of contact, information presented, and delivery method for health behavior interventions. eHealth may be a meaningful way to promote change in dietary behaviors for AYA cancer survivors through individualized tailoring.
Results from our systematic review indicated higher study retention and adherence for studies that included an eHealth component of either SMS or email; however, compliance was lower with daily interactive web-based required components. While the length and intensity of the interventions may have had an influence on participant completion rates, demographics, external commitments, and social support all may have influenced participant adherence, which can impact findings on measured outcomes.
This systematic review is the first comprehensive evaluation of the current state of literature for dietary interventions for AYA cancer survivors. Results suggest that this is an area in need for additional scientific study, and through our narrative synthesis, we developed a conceptual framework of considerations for future dietary interventions for AYA cancer survivors.
One strength of this research was the rigorousness of the risk of bias and study quality assessment of the eligible studies. While the number of studies included in our review was limited, all included studies had at least one positive, predetermined primary outcome in the intervention, and the participants represented the most common AYA cancer diagnoses (e.g., breast, testicular, leukemia, and lymphoma). In addition, the included studies did comprise a characteristic sample of the population and the interventions that were our main foci of interest. Results from this systematic review build on previous evidence in AYA cancer survivors and provides guidance for future development of dietary interventions targeted for AYA cancer survivors.
This systematic review was limited by the current variable definitions of AYA cancer survivors and limited use of the term in literature indexing. To address this, we developed a search strategy, which would capture a broader range of dietary interventions in cancer survivorship, and independently evaluated the included participants in potentially eligible studies to meet one of our three determined criteria of defining AYA cancer survivors. Important to our a priori objectives, the findings suggest that all of the published studies included in this systematic review were feasibility and preliminary efficacy studies, and as such lacked statistical power to observe test effectiveness in relationship to change in metabolic biomarkers. Furthermore, all the studies were of relatively short duration (12 weeks to 12 months), limiting their potential to evaluate the influence of the intervention on late-term metabolic effects of cancer treatment.
Conclusion
Limited studies exist detailing the efficacy of dietary interventions for dietary behavior change, metabolic biomarkers, and quality of life for AYA cancer survivors. Results detailed in this systematic review should be interpreted with caution given the limited number of eligible studies included. Furthermore, of the four included studies, three recruited participants in the upper age range (>35 years) of the spectrum of AYA, indicating a disparity in engaging younger AYA cancer survivors.
There is still clearly a need to address dietary care gaps for AYA cancer survivors, a growing, yet understudied, population. Efforts to comprehensively consider the unique physiological and psychosocial needs of AYA cancer survivors throughout the design and delivery of future targeted dietary interventions are imperative. Future trials may also benefit from individualized tailoring to impact the incidence and severity of late-term metabolic health effects in this at-risk population.
Footnotes
Acknowledgments
Access to electronic databases was available through the University of Arizona Health Sciences Library.
Author Disclosure Statement
Lisa Kopp is an employee of the contract research organization Covance.
Funding Information
The completion of this systematic review received no industry, foundation, or governmental funding.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.