
Abstract
Purpose:
Breast cancer is the most common cancer diagnosed among adolescent and young adult (AYA) females worldwide, but epidemiological patterns unique to this group are often obscured when results are combined with older patients. This study investigates breast cancer incidence and survival among AYA females, including differences by broad stage at diagnosis.
Methods:
A retrospective, population-based cohort study was conducted using de-identified data for females in Queensland, Australia, aged 15–39 diagnosed with a first primary breast cancer between 1997 and 2014 with follow-up to December 31, 2016. Incidence rate trends were examined with Joinpoint analysis. Cause-specific survival was calculated for key characteristics, and 5-year adjusted hazard ratios (HRs) were estimated from a multivariable flexible parametric model.
Results:
The study cohort comprised 2337 patients, of whom two-thirds (n = 1565, 67%) were diagnosed with advanced disease (tumor diameter >20 mm, lymph node involvement or presence of distant metastases at diagnosis). Incidence rates of localized tumors decreased by 1.9% per year (95% confidence interval [CI] −3.5% to −0.4%) over the study period, whereas the trend for advanced breast cancers remained stable. Five-year cause-specific survival increased from 85% to 92% for 2011–2014 compared to 1997–2001 (adjusted HR = 0.43, 95% CI = 0.29–0.65). Patients who were Indigenous from disadvantaged areas or diagnosed with advanced stage experienced significantly worse survival.
Conclusion:
The high proportion of younger females diagnosed with advanced breast cancer should be the focus of future campaigns to improve awareness and earlier detection. While survival has increased over time, further work is required to ensure that this progress is experienced equitably by all patients.
Introduction
Breast cancer is the most common cancer diagnosed among adolescent and young adult (AYA) females (ages 15–39) globally. 1 There were an estimated 244,000 incident cases worldwide during 2018, 1 representing almost a third (31%) of all cancers diagnosed within this demographic group and 12% of female breast cancer diagnoses across all age groups.
There is mounting biological evidence to suggest that breast cancer among younger females is a distinct disease. Breast tumors in the AYA age group tend to be larger at diagnosis, less well-differentiated, and more likely to be hormone-receptor negative compared to older women.2,3 Younger age has been identified as an independent predictor of poorer prognosis even after accounting for tumor characteristics, 4 with AYA patients being more likely to experience local recurrence following treatment or to develop distant metastases.5–7
As with many cancers, breast cancer is generally more difficult to diagnose at an earlier age. Routine screening is generally not recommended for females younger than 40 years of age (except for those considered to be at high risk) because breast cancer is comparatively uncommon in this age group and mammography is less effective due to the breast tissue in younger females usually being denser.8,9 Consequently, AYA females tend to present with symptomatic disease at a more advanced stage than older women. 10
There are also some differences in the etiology of breast cancers diagnosed among younger versus older women. For example, while a higher body mass index among premenopausal women tends to be protective against breast cancer, the converse is true postmenopausally.11,12 Similarly, nulliparity lowers the risk of breast cancer in younger women, but carries an increased risk later in life.12,13 Family history is strongly associated with early onset breast cancer, although only a small proportion of AYA breast cancers are associated with known genetic or hereditary factors. 4 Additional issues more specific to the AYA group include an increased risk associated with recent use of oral contraceptives 14 and childhood therapeutic chest radiation. 15
Given the differences that exist in the biology and etiology of AYA breast cancer, it is reasonable to assume that epidemiological patterns may also be distinctive within this age group. However, data relating to AYA patients are often obscured when information is reported for female breast cancer across all ages combined. The aim of this study was therefore to investigate incidence trends and survival for AYA female breast cancer in Queensland, Australia, with a focus on reporting results by broad stage at diagnosis.
Methods
Data
Unit record data for the study were sourced from the population-based Queensland Cancer Register (QCR) and supplied in accordance with the Public Health Act (2005). 16 Specific ethics approval was not required as all identifying information was removed from the data extract. Details in the data extract included demographic variables (sex, age, Indigenous status, and locality of residence), tumor information (body site, morphology, tumor diameter, and lymph node involvement), date of diagnosis, and date and cause of death (where applicable). Mortality status in the QCR is kept up to date through regular matching with both the Queensland Registry of Births, Deaths, and Marriages and the National Death Index of Australia.
Stage at diagnosis was broadly classified as either localized or advanced, similar to previous breast cancer studies in Queensland.17,18 The TNM (tumor size, nodal involvement, and presence of metastases) system 19 is typically used to classify cancer stage in adults. Information on tumor diameter and lymph node involvement has been routinely collected by the QCR since 1997, but data on metastatic status are absent (apart from cases where the metastases were used as the basis of diagnosis). For the purposes of this study, localized breast cancer was defined as a tumor with a maximum diameter ≤20 mm and no evidence of lymph node involvement, similar to TNM stage I (except that the absence of metastases could not be confirmed). Remaining cases with a tumor diameter >20 mm, positive involvement of the lymph nodes, or where diagnosis was on the basis of metastatic disease were grouped into the category of advanced breast cancers, approximating an aggregation of TNM stages II–IV.
Eligible patients were female residents of Queensland aged 15–39 who were diagnosed with a first primary malignant breast cancer (ICD-10-AM 20 site codes C50.0-C50.9) between 1997 and 2014. Tumor morphology was used to group patients into the categories of “Ductal,” “Lobular,” “Mixed Ductal/Lobular,” and “Other,” as defined in Table 1. Those with missing data for stage, Indigenous status, or locality of residence were excluded.
Classification of the Study Cohort into Tumor Morphology Groups
NOS, not otherwise specified.
Remoteness of residence, based on the patient's usual address at the time of diagnosis, was categorized according to the Australian Standard Geographical Classification Remoteness Structure. 21 Area-based socioeconomic status was grouped into quintiles using the Index of Relative Socioeconomic Disadvantage. 22
Analysis
Differences in the distribution of key patient and tumor characteristics by stage at diagnosis were assessed using either the chi-square test (categorical variables) or the nonparametric test for trend across ordered groups (ordinal variables).
Incidence rates were directly age-standardized using the World Health Organization (WHO) World Standard Population. 23 Joinpoint regression 24 was then applied to calculate trends, with results presented in terms of the annual percentage change (APC). The Joinpoint procedure fits one or more linear trend line segments to the observed data, taking into account any changes in magnitude or direction over time. Models were specified with a maximum of two Joinpoints in combination with a minimum of 5 years between Joinpoints or from a Joinpoint to either end of the data series. Two-sided t-tests were used to determine the statistical significance of the APCs. The regression mean functions of the trend lines by stage at diagnosis were also tested for parallelism. 25
Estimates of 5-year cause-specific survival were produced using the cohort method, 26 with follow-up on mortality available to December 31, 2016. Survival was censored in the following situations (whichever occurred first): at the date of death for those who died from a cause other than breast cancer; at the end date for patients with <5 years of follow-up who were still alive; or 5 years from the date of diagnosis. Cause-specific survival was reported rather than relative survival due to the unavailability of accurate population life tables stratified by some of the variables of interest, such as Indigenous status and locality of residence. Little difference would be expected between estimates of cause-specific and relative survival, given the low underlying probability of death within the AYA age group.
A multivariable flexible parametric model 27 was then applied to assess differences in survival up to 5 years after diagnosis, with results expressed in terms of adjusted hazard ratios (HRs). The model was adjusted for age group, period of diagnosis, Indigenous status, place of residence, area-based socioeconomic status, morphology group, and stage at diagnosis. Two-way interactions between these covariates were also considered for inclusion, but none was found to be statistically significant (all interactions p > 0.05).
Selected analyses were repeated for the 40–59 and 60 and over age groups to provide benchmark comparisons. All computations were conducted using Stata/SE version 15.1 for Windows (StataCorp, LLC, College Station, TX). Point estimates were presented along with 95% confidence intervals (95% CIs) and/or p-values as appropriate.
Results
Incidence
From a total of 2552 Queensland AYA females who were diagnosed with breast cancer between 1997 and 2014, breast cancer stage was not assigned for 200 (7.8%), and a further 15 (0.6%) were excluded due to missing data on Indigenous status or locality of residence. Those who were excluded were more likely to be younger compared to the remaining 2337 (91.6%) eligible patients (ptrend < 0.001); however, there was no relationship between exclusion and year of diagnosis (ptrend = 0.88, results not shown).
Table 2 presents the key details for the study cohort stratified by stage at diagnosis. Overall median age at diagnosis was 36; <9% were younger than 30 years of age at diagnosis, and there was no change in this age mix over time (p = 0.65). Indigenous Australians comprised 2% of the study cohort. Ductal carcinoma was by far the most common morphology group, accounting for 85% of all cases.
Distribution of Breast Cancer in Adolescent and Young Adult Females by Broad Stage at Diagnosis and Selected Characteristics, Queensland, 1997–2014
SES, socioeconomic status.
Around twice as many patients were diagnosed with advanced breast cancer than localized breast cancer (33% and 67%, respectively) and the percentage with advanced disease at diagnosis rose significantly (ptrend = 0.002) over the study period, from 63% between 1997 and 2001 to 71% between 2011 and 2014 (Table 2). Indigenous AYA females were more likely to be diagnosed with advanced breast cancer than were non-Indigenous AYA females (82% and 67%, respectively; p = 0.02). A significant trend toward a higher proportion of cases with advanced stage at diagnosis was found as place of residence become more remote (ptrend = 0.036) and for those living in more disadvantaged areas (ptrend = 0.002). Tumors with a mixed morphology of ductal and/or lobular were more likely to be advanced (79%) at the time of diagnosis.
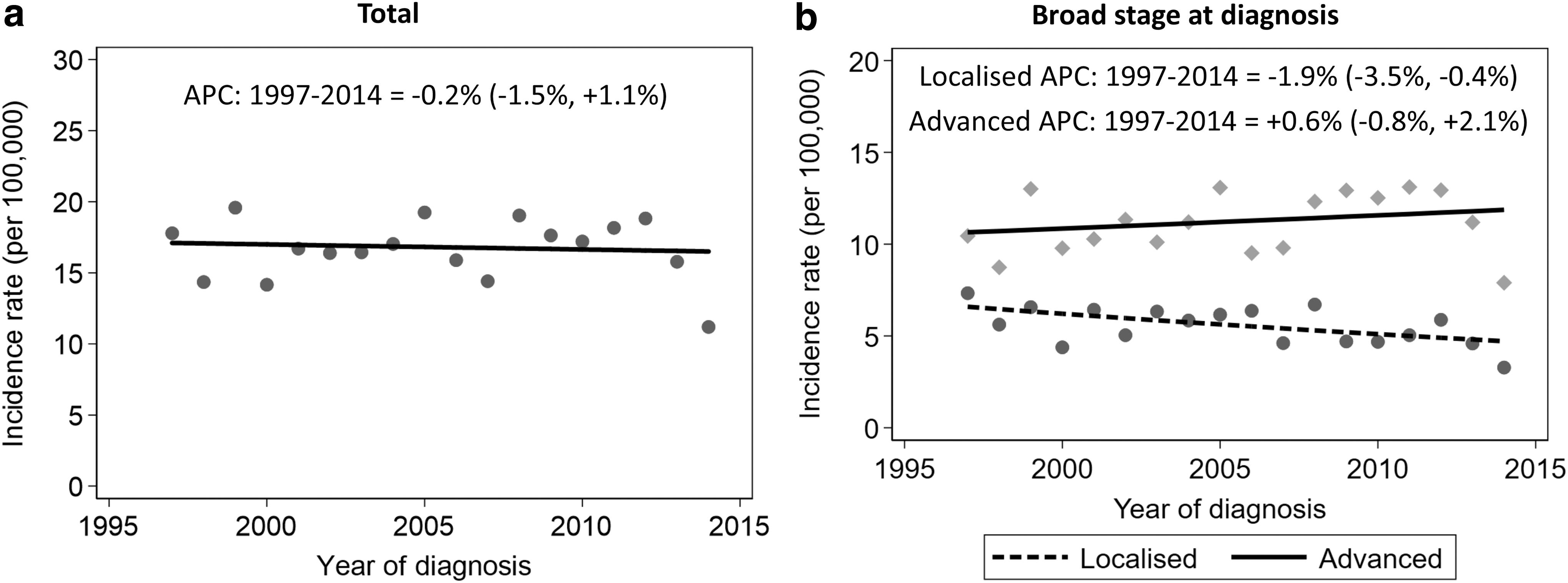
A stable trend in the overall annual incidence rates was observed across the study period (APC = −0.2%, p = 0.74), with an average age-adjusted rate of 16.6 per 100,000 AYA females per year (95% CI = 16.0–17.3) (Fig. 1a). There was a distinct difference (pparallel = 0.005) in incidence rate trends by stage at diagnosis (Fig. 1b), with an ongoing decrease in localized breast cancer (APC = −1.9%, p = 0.02) in contrast to a small (nonsignificant) increase in the incidence of advanced breast cancer (APC = +0.6%, p = 0.37). A divergence in incidence rates for localized versus advanced breast cancers was also observed for patients aged 40–59 (Supplementary Fig. S1), whereas for patients in the older than 60 years age group, the trends were increasing in parallel from 2007 onward (Supplementary Fig. S2).
Incidence rate trends for AYA female breast cancer by
Survival
Median follow-up time per patient was 8.3 years (interquartile range = 4.8–13.2 years), with a maximum attained age of 59. Approximately one in five (n = 464, 20%) patients in the study cohort died before the end of the study period. More than half of these deaths (n = 265, 57%) occurred within 5 years of diagnosis. Breast cancer was responsible for the majority of deaths within the study cohort (n = 434, 94%), with the remaining mortality divided between different cancers (n = 16, 3%) and causes other than cancer (n = 14, 3%).
Five-year cause-specific survival for AYA female breast cancer was 88% (95% CI = 87%–90%). Statistically significant differences in survival were found by year of diagnosis, Indigenous status, socioeconomic status, and stage at diagnosis after multivariable modeling (Table 3 and Fig. 2). Survival improved over time, from 85% for those diagnosed between 1997 and 2001 to 92% for the period 2011 to 2014 (adjusted HR = 0.43; p < 0.001). The improvement in survival was only significant, however, among patients with advanced breast cancer, rising from 79% (95% CI = 74%–82%) between 1997 and 2001 to 88% (95% CI = 84%–92%) between 2011 and 2014 (p < 0.001). Indigenous AYA females had more than double the mortality risk from breast cancer within 5 years of diagnosis compared to non-Indigenous patients (5-year cause-specific survival of 67% and 89%, respectively, adjusted HR = 2.68; p < 0.001) and there was a significant trend toward higher survival rates as area-based socioeconomic disadvantage decreased (84% for most disadvantaged compared to 92% for least disadvantaged, adjusted HR = 1.60; p = 0.03). Patients with advanced disease were at a sixfold higher risk of mortality in relationship to those with localized breast cancer (survival of 84% and 97%, respectively, adjusted HR = 6.20; p < 0.001).

Five-year Kaplan–Meier cause-specific survival curves for breast cancer in AYA females by selected characteristics
Five-Year Cause-Specific Survival and Adjusted Hazard Ratios for Breast Cancer in Adolescent and Young Adult Females by Selected Characteristics, Queensland, 1997–2014
Survival was calculated using the cohort method, with follow-up on mortality status available to December 31, 2016.
95% CI, 95% confidence interval; NA, not applicable; SES, socioeconomic status.
Comparative survival data for the 40–59 and 60 and older age groups are provided in Supplementary Tables S1 and S2, respectively. Five-year cause-specific survival was 93% for the 40–59 age cohort and 91% for those aged 60 and older, both higher than the 88% recorded for AYA patients. Similar to the AYA group, significantly better survival in both middle-aged and older females with breast cancer was found for those diagnosed in more recent time periods, non-Indigenous patients (statistically significant in the 40–59 age group only), those living in the least socioeconomically disadvantaged areas, and patients with localized disease.
Discussion
While some articles have considered the incidence and survival of breast cancer by age group, there is a scarcity of literature looking at epidemiological patterns for AYA patients stratified by stage. Similar to our finding of a stable trend in breast cancer incidence rates for all AYA females combined, data from cancer registries in Asia 28 have shown only small increases since the mid-1980s. A different picture has emerged elsewhere, with ongoing significant annual increases in recent years for pooled information from Europe29,30 and among whites in the United States. 31 It has been postulated that these rising trends could be driven by a combination of changes in diagnostic practices and mounting exposure to risk factors for premenopausal breast cancer within the AYA group.29,30 Given that similar population influences would be expected to operate in Queensland, reasons for the stable incidence rates observed here are unclear.
Our finding that two-thirds of female AYA breast cancer patients in Queensland were diagnosed with advanced disease (TNM stage II or higher) closely corresponds with results from the United States for the 25–29 age group. 32 While incidence rates of advanced breast cancer have remained fairly stable over time among AYA females in Queensland, there has been a decrease for localized breast cancer. The proportion of AYA patients with advanced cancer has consequently increased over time. By comparison, trends for localized and regional breast cancer have remained stable among females aged 25–39 between 1976 and 2009 in the United States, but incidence rates of metastatic breast cancer within this group increased by more than 2% per year on average. 33 A study among Norwegian women of all ages with breast cancer reported that changes in coding and classification practices had an impact on stage-specific incidence trends, 34 providing a possible explanation for our findings. Other potential causes for the ongoing divergence in incidence rate trends by stage at diagnosis in Queensland (which were not unique to the AYA age group) are yet to be identified.
Survival for AYA females in Queensland has improved, particularly for those with advanced disease. Care must be taken when interpreting stage-specific changes in survival over time, however, due to issues such as possible stage migration arising from evolving diagnostic techniques. 35 Nonetheless, our overall results appear to compare favorably with data from elsewhere. Five-year relative survival for females aged 15–29 with breast cancer in The Netherlands 36 between 1989 and 2009 was 75% while a study from Japan 37 reported 81% 5-year relative survival among breast cancer patients aged 15–34 for the period 2002–2006. These results were substantially lower than our estimate of around 86%–87% in each of the 15–24, 25–29, and 30–34 age groups in Queensland between 1997 and 2014. Similar to Queensland, both of the other studies described a significant improvement in survival over time.36,37
The survival advantage experienced by Queensland AYA females compared to other published results was also evident within stage categories. For example, Bodmer et al. 38 reported 5-year relative survival for female breast cancer patients in Switzerland aged 20–39 and diagnosed between 1996 and 2009 varied from 94% for localized stage and 83% for regional stage to only 19% for patients who had metastases present at diagnosis. This compares with 97% for localized disease and 84% for advanced disease (comprising regional and metastatic tumors combined) in our study.
Breast cancer survival rates are typically lower for AYA females compared to their older peers, although patterns across key prognostic variables were similar. This survival disparity by age is due, at least in part, to tumors diagnosed at younger ages being more aggressive and hence less responsive to treatment.4,32 Data from the United States 39 have shown that breast cancer patients aged 15–39 with localized or regional disease had significantly higher 5-year mortality compared to older females, whereas the reverse was true for those with distant stage disease.
Two percent of AYA female breast cancer patients were Indigenous, similar to the distribution in the general Australian population of females aged 15–39 at the time of the study. 40 They were, however, more likely to be diagnosed with advanced disease than non-Indigenous females. A recent systematic review 41 found that compared with non-Indigenous women, Indigenous women (of all ages) diagnosed with breast cancer had poorer survival, with this most likely reflecting greater geographical isolation, a higher likelihood of advanced disease, different patterns of care, increased comorbidities, and higher socioeconomic disadvantage. While studies have shown that Indigenous women were more likely to be diagnosed with breast cancer when younger,42,43 information about the specific needs that AYA Indigenous females have when they are diagnosed with breast cancer is lacking. The survival gradient for AYA females by area disadvantage, with higher survival for those in least disadvantaged areas, is also consistent with that reported for women of all ages diagnosed in Queensland. 44
The study had some limitations. Perhaps the most important of these was that we were unable to stratify advanced stage into regional and metastatic disease, similar to the stage definitions used in Surveillance, Epidemiology, and End Results program (SEER) and elsewhere. Although it is unlikely that cancers defined as localized (small tumors without lymph node involvement) had metastasized at the time of diagnosis, we cannot rule out this possibility. The relatively small number of Indigenous patients in the study cohort affected the precision of the corresponding estimates that were reported and precluded the possibility of calculating trend estimates for this group. Information on lifestyle-related risk factors was not available from the Queensland Cancer Registry.
In conclusion, the differing incidence trends by stage presented here illustrate the importance of collecting stage at cancer diagnosis on a population basis as part of routine cancer registration. Stage data are vital to evaluate changes to incidence and survival over time, which in turn may inform targeted cancer control strategies. A major effort is currently underway to improve the collection of data on stage at diagnosis within cancer registries throughout Australia. Furthermore, our results showed that two out of three AYA females in Queensland with breast cancer are diagnosed with advanced disease. This percentage is even higher for patients who are Indigenous and/or who live in more remote or disadvantaged areas. A better understanding of the factors that lead to advanced disease at diagnosis is necessary so that public health programs can then be implemented to aid with prevention and earlier detection.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.