
Abstract
Purpose:
The Adolescent and Young Adult (AYA) gap describes the drop-off in survivorship improvement among 15–39-year-olds compared with patients with cancer under 15 or over 39. A large body of literature explores why this population experiences lower rates of trial enrollment, an issue of particular importance since this single factor is thought to have the greatest impact on the decrease in survivorship. The purpose of this research is primarily to identify whether or not AYA patients within a large academic center who were treated by a pediatric specialist were more likely to be enrolled in a clinical trial.
Methods:
A retrospective cohort study was conducted by chart review of AYA cancer patients within a large academic institution diagnosed from 2014 to 2016. Information, including physician specialty, sex, cancer subtype, age, and ethnicity were extracted and analyzed in relation to enrollment data from the clinical trials office.
Results:
Patients managed by a pediatric specialist were over 10 times more likely (p < 0.01) than those treated by adult specialists to be enrolled in a clinical trial. When stratified by cancer subtype, pediatric specialist management still predicted trial enrollment in subtypes more common in younger patients, including germ cell and osseous neoplasms, leukemia, and lymphoma. Neither age, sex, nor ethnicity correlated significantly with enrollment.
Conclusion:
These data not only depict the necessity of abandoning traditional age cutoffs when dealing with AYA cancer, but also reveal the need for further study to understand and ultimately rectify the discrepancy between pediatric and adult utilization of clinical trial enrollment.
Introduction
Despite upward trends in U.S. cancer survival over the past few decades, children under 15 and adults over 40 enjoy greater rates of improvement than the 15–39-year-old (Adolescent and Young Adult or AYA) demographic.1,2 In the last quarter of the 20th century, the improvement in survival rate exceeded 1.5% per year in children under 15 and adults over 50, but among 15–24 year-olds, improvement was less than 0.5%; 25–34 year-olds saw no significant improvement at all. 1 Not only do AYA survival rates trail behind that of both children and older adults, but also 15–34-year-old patients experience greater incidence of cancer than that of any other age group aside from the oldest Americans 65 years of age and over. 3 The causes of this “AYA gap” are multifactorial and not yet entirely understood—ranging from an AYA sense of invincibility, leading to delayed presentation to care, to lack of health insurance, to under-researched biological tumor features unique to this age group, to low enrollment in clinical trials.4–7
The lag in survival improvement within the AYA population coincides with a drop-off in clinical trial enrollment for this age group.3,5 While pediatric oncologists consider clinical trials the standard of care, their patients over 14 years of age and those entering young adulthood have significantly lower rates of enrollment in these trials compared with children and adults.1,2,5,8 A recent study of 18 years of comprehensive national cancer survival and clinical trial enrollment data found that increased survival and decreased morbidity correlated with clinical trial enrollment from age at diagnosis 15–39. 2
Due to the varying predominances of tumor types by age, patients in their late teens and 20's with ALL might be managed by pediatric oncologists while a preteen with a carcinoma might receive care from a physician who specializes in medical oncology.1,9 For AYAs with ALL, for example, current NCCN guidelines recommend pediatric backbone-style therapy or clinical trials and the literature indicates that pediatric, as opposed to adult, protocols lead to higher survival rates.1,10 Data suggest that patients with certain sarcomas (rhabdomyosarcoma) and osseous tumors (Ewing sarcoma) also benefit from pediatric protocols. 11
Although more trials may be available to AYAs at large academic centers, the majority of AYA patients are treated at community sites such as those within the National Cancer Institute's Community Oncology Research Program (NCORP). 12 The large tertiary referral center managing patients in this study, University Health, is associated with the city's medical school, UT Health San Antonio. The University Hospital System (UHS), including the medical school, is the lead site for the Texas Pediatric Minority Underserved NCORP, a network that now includes community cancer health networks and serves over half of the state's population. As a first step in a comprehensive evaluation of AYA cancer care across community sites, we set out to describe the AYA cancer population at this lead center by determining the relationship between clinical trial enrollment and oncology provider type (pediatric vs. adult) in addition to age, sex, ethnicity, and cancer diagnosis.
Materials and Methods
Data source
Data collection began with a retrospective chart review of electronic health records within University Health System of patients diagnosed with any malignancy from January 1, 2014 to December 31, 2016, who were between the ages of 15 and 39 years at the time of diagnosis. UHS is a 716 bed (American Hospital Directory) public hospital and participant in the Medicaid Disproportionate Share Hospital Program that serves Bexar County's ∼2 million people (U.S. Census Bureau). Demographic and treatment data extracted through thorough chart review included: age at diagnosis, cancer type (classified using the standard Surveillance, Epidemiology, and End Results Program within the National Cancer Institute's classifications), primary provider (adult versus pediatric), sex, and ethnicity. Clinical trial enrollment data were acquired through the UHS Cancer Center Clinical Trials Office. Patients were searched by birthday and full name then designated as enrolled or not enrolled.
To determine whether the patient received care from an adult or pediatric specialist, all of the available encounters in the University Hospital medical records system were considered. If the patient received chemotherapy, the primary physician was noted as the individual who signed the orders. If the patient received surgery or radiation, the surgeon or radiologist was listed. If the patient did not receive treatment, records of outpatient encounters were assessed to identify the oncologist who wrote the majority, if not all, of the patient's clinic notes.
Statistical analyses
Data were stored in Microsoft Excel and reviewed to ensure accuracy. Categorical data (sex, ethnicity, SEER diagnostic category, trial enrollment, pedi v. adult physician) were then numerically coded for statistical analysis.
Statistical analyses were acquired through STATA/IC 15.1. One-way frequency tables were used to describe the population. The relationship between the independent variables studied and clinical trial enrollment was characterized by odds ratios comparing enrolled and nonenrolled patients. For example, the odds ratio for pediatric physician management reflects the odds of clinical trial enrollment if an individual was treated by a pediatric physician as opposed to treatment by an adult specialist.
Cancer type was considered a probable confounding factor in this study due to the significant variation in cancer diagnoses with age. Younger AYA patients have a propensity toward certain cancer types, some of which may be more amenable toward clinical trials. Therefore, data were subsequently stratified by this variable to identify whether or not relationships between physician management and enrollment were mediated by age-associated cancer subtypes.
Results
UHS provider type
The breakdown of physician specialty by cancer type follows trends similar to the typical age distributions of the cancer types (Table 1). Cancers more common in pediatrics like osseous and chondromatous neoplasms and leukemias (Fig. 1) had the highest rates of pediatric specialists' managing care with 50% and 52% pediatric oncologists, respectively (Fig. 2). 5 In contrast, only 12% of lymphoma patients were treated by pediatric oncologists, including all of the patients under age 18 and two of the 38 patients in the 20–39-year-old group (Fig. 2).1,5 Among the youngest age bracket, 15–19 year-olds, only patients with lymphoma had a rate of 100% treatment by pediatric specialists while osseous and chondromatous neoplasms and leukemias were close behind at 89% and 83%, respectively (Fig. 3).

Incidence of AYA Cancer Subtypes by Age Group. Number of patients diagnosed with each cancer subtype from 2014 to 2016 stratified by age bracket. Visual representation of data described in Table 1. AYA, adolescent and young adult; CNS, central nervous system.
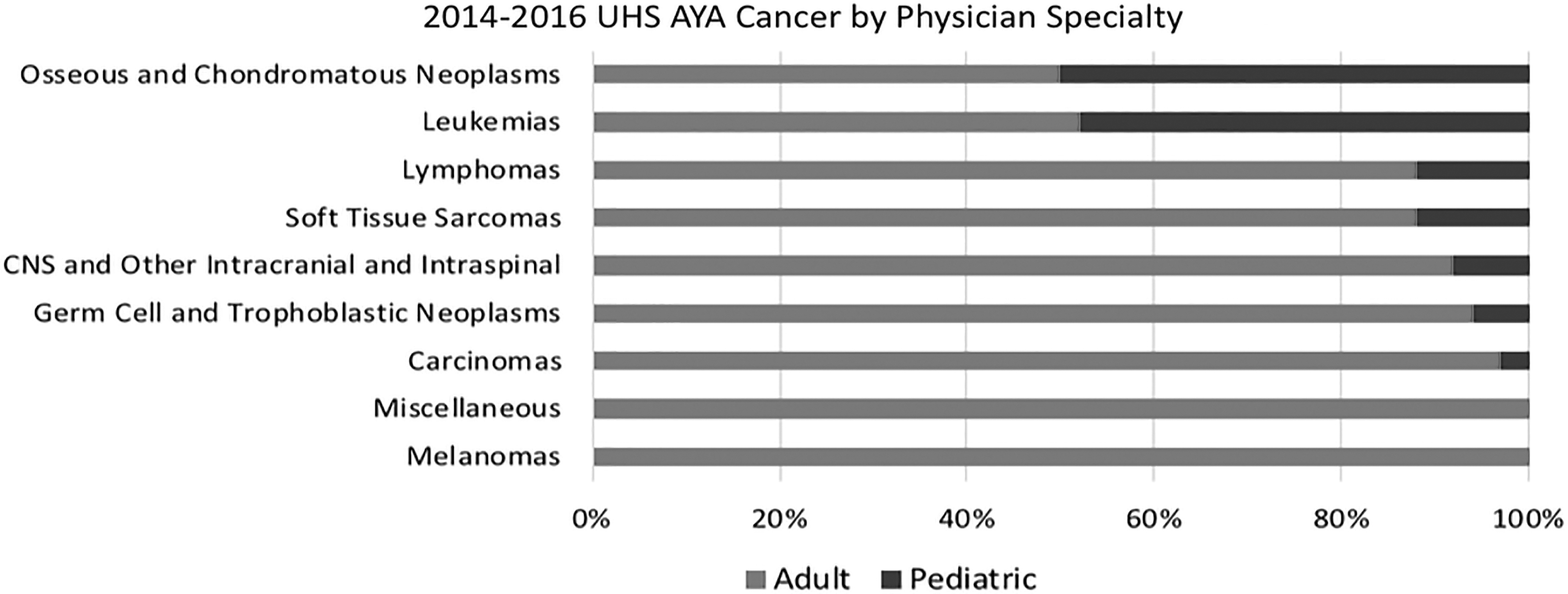
2014–2016 UHS AYA Cancer by Physician Specialty. Percentage of patients managed by pediatric v. adult physicians stratified by cancer subtype. Leukemias and osseous and chondromatous neoplasms both have peak incidences by percentage among the youngest age brackets, which parallels their propensity toward greater percentages of pediatric physician management. UHS, University Hospital System.

Clinical Trial Enrollment by Cancer Diagnosis. Percentage of patients within each cancer subtype enrolled in a clinical trial. Enrollment peaks among patients with leukemias and osseous and chondromatous neoplasms.
Adolescent and Young Adult Cancer Patient Demographics and Diagnoses
Descriptive statistics stratified by age bracket for all AYA patients diagnosed with cancer from 2014 to 2016 managed at UHS.
AYA, adolescent and young adult; UHS, University Hospital System.
Although data were analyzed by cancer subtype and not broken down further into sub-subtypes, it is worth noting that of UHS's 13 new ALL cases, ages ranging 16–35 at diagnosis, 11 saw a pediatric oncologist, whereas two, ages 26 and 35, saw adult physicians. ALL is mentioned in this study because this specific type of leukemia is often referenced in AYA cancer literature as an example of pediatric treatment protocols' superiority in adults with this disease.
Clinical trial enrollment
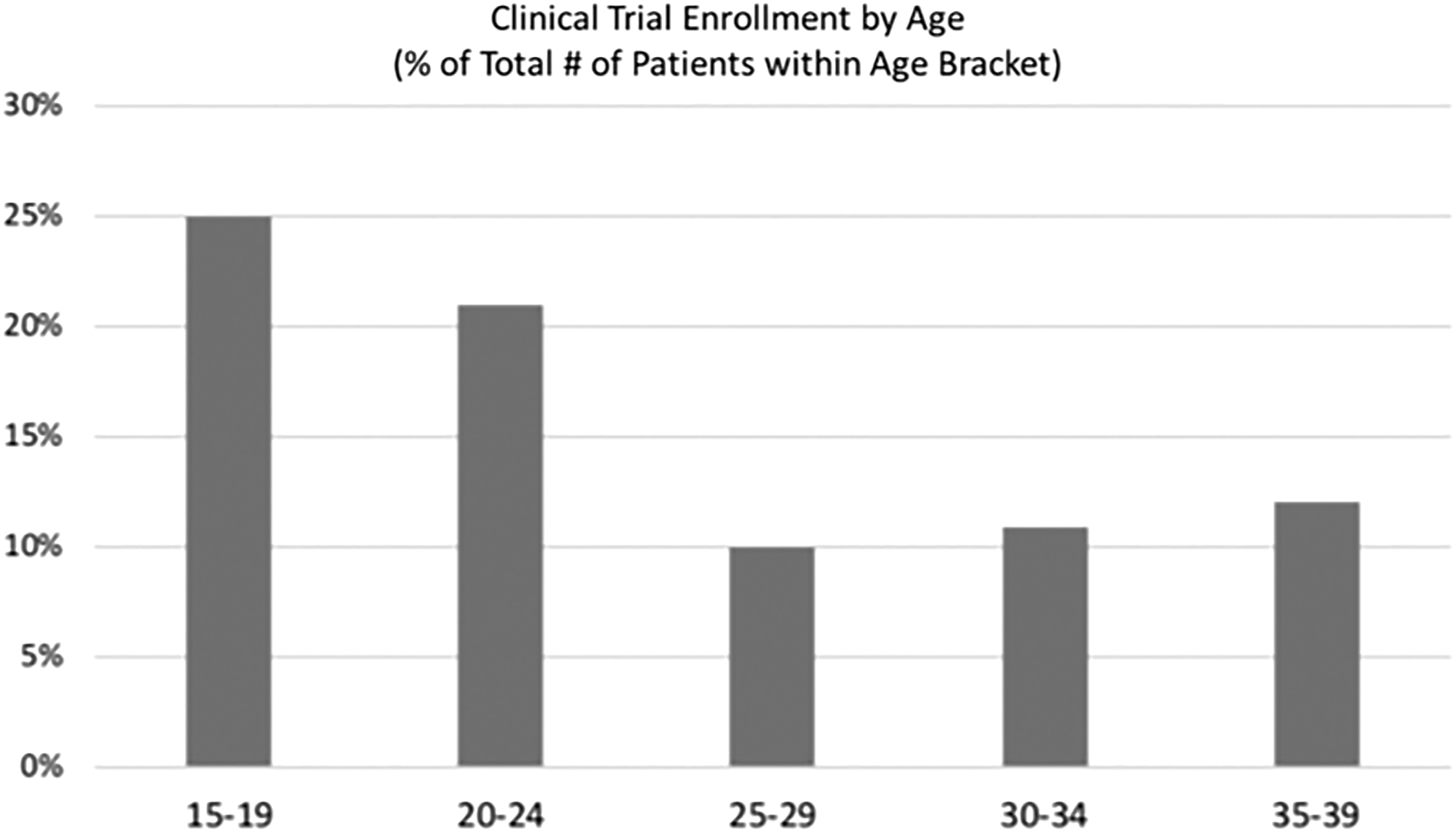
If an AYA patient in this data set was treated by a pediatric specialist, he or she was more than 10 times more likely to be enrolled in a clinical trial (p < 0.01) (Table 2). Additionally, patients who were 15–19 years old at the time of diagnosis were significantly (OR = 2.5, p < 0.01) more likely to be enrolled in a clinical trial (Table 2). Those 20–24 years of age also had a greater odds ratio (OR = 1.7) of enrollment, whereas patients 25–29 years of age at diagnosis were more likely not to be enrolled in a trial (OR = 0.56), but neither finding was statistically significant (p = 0.09 and p = 0.12, respectively) (Table 2). Both the proportions of enrolled individuals and the odds ratios of enrollment increased from the 25–29-year-old bracket to the 30–34 bracket and again into the 35–39 age group (Fig. 4). This increase is, in part, related to the large number of enrollees for breast carcinoma, a disease more prevalent among 30–39 year-olds (Fig. 1).
Percentage of Patients Managed by Pediatric Specialist. Percentage of total patients within each cancer subtype managed by a pediatric specialist further stratified by age bracket. Patients with multiple cancer subtypes maintain some percentage of pediatric physician management even into the 25–29 year-olds.
Potential Predictors of Clinical Trial Enrollment
Odds ratio of clinical trial enrollment if a patient is a member of the identified subgroup compared with all of the other subgroups within the corresponding independent variable (bold font). The strongest predictor of enrollment was management by a pediatric physician (OR = 10.8, p < 0.01).
Bold numbers are those statistically significant, given a significance level of 0.05.
There were no patients within this subgroup enrolled in a clinical trial; therefore a p value cannot be calculated and is listed as not applicable (N/A).
After stratification by cancer subtype, patients with leukemia, lymphoma, osseous/chondromatous neoplasms, soft tissue sarcomas, and germ cell tumors were still significantly more likely (p < 0.05) to be enrolled in a clinical trial if they were treated by a pediatric physician (Table 3) (Fig. 5). Pediatric physician treatment of patients with central nervous system (CNS) neoplasms also correlated with higher clinical trial enrollment, but the relationship was not statistically significant. Regarding cancer type alone, only patients with leukemia and osseous/chondromatous neoplasms were significantly more likely (p < 0.01) to be enrolled in a clinical trial (Table 2). Interestingly, a patient with a carcinoma was significantly less likely to be enrolled in a trial (p < 0.05) (Table 2).

Clinical Trial Enrollment by Age. Percentage of patients within each age bracket enrolled in a clinical trial. Enrollment reaches its lowest percentage among 25–29 year-olds while the youngest AYA patients have the highest percentage of enrollment.
Odds of Clinical Trial Enrollment if Treated by a Pediatric Physician: Stratified by Cancer Subtype
Odds ratio of clinical trial enrollment comparing the patients with a particular cancer diagnosis who are treated by a pediatric physician to those with the same diagnosis managed by an adult specialist. Patients treated by a pediatric physician with leukemia, lymphoma, and germ cell and trophoblastic neoplasms had the greatest odds of enrollment (OR = 60, 44, 46, respectively, p < 0.01).
There were no patients within this subgroup enrolled in a clinical trial; therefore a p value cannot be calculated and is listed as not applicable (N/A).
Ethnicity did not significantly predict enrollment. The odds ratio for Hispanic patients was greater than one while that for Caucasians was slightly less than one indicating that, although data are not statistically significant, there was a slight predilection for Hispanic patients to have greater trial enrollment (Table 2). Notably, Bexar County, in which UHS is located, is 60% Hispanic (Bexar census), a proportion similar to the demographic distribution of the current data set in which ∼70% of patients were Hispanic. Otherwise, no individuals of African American, Asian, or Unknown ethnicity were enrolled in trials. Furthermore, although men were more likely to be enrolled in a trial (OR = 1.5), the result was not statistically significant (p = 1.3) (Table 2).
Discussion
Clinical trial enrollment among AYA cancer patients is critical for not only furthering treatment modalities, but also for improving survival.13,14 Since this population continues to suffer from poor clinical trial enrollment compared with that of pediatric and older patients, it is important to identify factors that correlate with increased enrollment. 14 Pediatric physician management was investigated because the overlap between diagnoses more common in the pediatric population and those more prevalent among young adults allows for a more fluid assignment of patients between pediatric and medical oncologists. It is not uncommon for patients 18 years of age and older to be managed by a pediatric specialist if their cancer type is more well known among this specialty.
The UHS data represent a large proportion of cancer patients in the surrounding region. Texas Department of State Health Services divides the state into 11 Public Health Regions and UHS exists with region 8. The National Institute of Health (NIH's) SEER (Surveillance, Epidemiology, and End Results Program) data identified about 3300 new AYA cancer cases in Public Health Region 8 between 2011 and 2015, for an average of about 660 patients a year. These data suggest that UHS alone, which averaged 160 patients a year per this data set, sees ∼25% of all new cancer diagnoses in the surrounding area stretching from the Gulf of Mexico to the western border with Mexico. 15
The single variable boasting the greatest correlation with clinical trial enrollment was treatment by a pediatric physician, as opposed to an adult specialist. The stratification by cancer subtype illuminates the pediatric management-trial enrollment relationship by controlling for the reality that the availability of clinical trials differs by diagnosis. For example, the proportions of trial-enrolled patients with leukemia and osseous/chondromatous neoplasms were several times greater than those for germ cell tumors or lymphomas. Leukemia and osseous/chondromatous neoplasms were also proportionally more common in patients 15–19 years of age who would be more likely to see a pediatric specialist by age alone, even without taking into account whether or not their subtype was more appropriate for pediatric or adult specialist management.
With regard to clinical trial enrollment of traditionally underrepresented ethnic minorities, those of Hispanic ethnicity were actually more likely to be enrolled (although not a statistically significant finding). 16 However, the failure to enroll African American or Asian individuals suggests that not only can UHS work to improve inclusion of those in traditionally underrepresented ethnicities, but also suggests more research is warranted with different demographic distributions than San Antonio's Hispanic and Caucasian-predominant population. Interestingly, although there were more women diagnosed with cancer at UHS over the 3-year period studied, men were slightly more likely (although statistically insignificantly so) to be enrolled in clinical trials.
This study is unique in its limitation to a single location. Although this results in fewer patients included in the analysis (n = 493) compared with larger multi-institutional studies, it controls for patient treatment center. Several studies address discrepancies in clinical trial enrollment between pediatric and adult treatment centers,17,18 correlating pediatric care center with increased enrollment, but physician specialty independent of center has yet to be addressed.
More research is needed to further parse out the specific reasons why patients with and without cancer subtypes unique to the AYA population have greater trial enrollment when treated by a pediatric physician. UHS has newly created inpatient space for AYA patients managed by any specialties, including but not limited to oncology. While an AYA oncology specialty may or may not come to fruition in the near future, by restructuring the inpatient floors to include an AYA unit, a combination of pediatric and medicine specialists can manage patients best suited to their own knowledge and experience. Furthermore, by increasing collaboration between the two specialties, perhaps UHS will see an increase in AYA clinical trial enrollment among those managed by both pediatric and adult specialists, leading to improved outcomes among cancer patients in this age group. The initiative taken by UHS and other hospitals in recognizing the uniqueness of AYA cancer patients will allow for future research into clinical trial enrollment before and after the creation of a specialized location.
Footnotes
Acknowledgments
The authors thank the University of Texas Health School of Public Health San Antonio campus for funding the purchase of STATA statistical software for this project and Melissa Kyzar in the University of Texas Health San Antonio Cancer Center Clinical Trials Office for extracting data on patients' enrollment status.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no funding for this study.