
Abstract
This cross sectional pilot study assesses the feasibility of conducting online research into cognitive mechanisms in adolescent and young adult cancer populations. Twenty-one participants, aged 18–39 years, answered questionnaires about mental defeat, rumination, cancer worry, anxiety, and experience participating in such research. Seven participants scored in the clinical range for anxiety. Cancer-related worry was common. Rumination and mental defeat were positively associated with anxiety. The participants reported the length and type of questions to be appropriate and not distressing. Findings may inform future research into cognitive mechanisms, which could aid the development of psychosocial interventions for young cancer patients.
Introduction
Adolescence and young adulthood are periods of rapid development and identity formation.1,2 Significant trauma and stressors, such as life-threatening illness can disrupt achievement of normative milestones and result in psychiatric disorders or heightened psychological distress. 3 As the number of adolescent and young adult (AYA) cancer survivors grows globally 4 research efforts are shifting toward understanding adaptation to life after cancer. Most of the research in psycho-oncology to date has focused on the effects of demographic and clinical factors on outcomes, with little mention of factors that could be relevant to psychosocial adaptation and which could be modifiable with training, such as cognitive mechanisms. 5
Descriptive studies report that over 50% of young survivors worry about late effects of cancer, and about half of all survivors report always having cancer at the back of their minds.6,7 Recent longitudinal work further supported that cancer-related worry remains a significant concern among AYA survivors, 8 and makes some of them reluctant to seek care, 6 which could carry long-term health implications. Greater identification with being a cancer survivor was also associated with higher depressive symptomatology. 9
Cancer illness presents a context marked by disruption of normal routine as well as by high levels of uncertainty, and as such increases the risk of maladaptive coping. 10 Examples of maladaptive cognitive styles are mental defeat and rumination. Defined as the perceived loss of all autonomy, 11 mental defeat predicts the development and maintenance of posttraumatic stress disorder, depression, anxiety, and suicidality. 12 Rumination is a cognitive process, which involves dwelling on past events. It is a self-focused, repetitive, and passive way of coping and a robust predictor of psychopathology. 13 Cancer illness and treatment might put individuals at risk for experiencing mental defeat and rumination, which could in turn contribute to psychological distress in AYA cancer patients and survivors. Because anxiety is an understudied, yet, a significant mental health concern in a subset of AYA population; 14 in this study, we focus on anxiety as the primary outcome of interest.
To the best of our knowledge, no study has yet evaluated associations between mental defeat, rumination, cancer-related worry, cancer identity, and anxiety in an online survey in AYA patients and survivors. This exploratory pilot study has two aims: (1) to assess the feasibility of online research into cognitive mechanisms and (2) to provide preliminary insights into which modifiable factors play a role in psychological adaptation in AYA cancer populations, which will aid future study development.
Methods
This cross sectional pilot study was conducted to inform the development of a large-scale, longitudinal online study. The Medical Sciences Interdivisional Research Ethics Committee at the University of Oxford granted approval (R61437/RE002).
The study was designed using Qualtrics, a secure online survey software provided by the university department. The anonymous survey link was open for 4 months and circulated via social media and patient advocacy groups. The survey was open to anyone across North America and Europe who were able to complete the questionnaires in English. Participants were AYA cancer patients or survivors diagnosed with any form of malignant cancer after 10 years of age and between 18 and 39 years at the time of the study. Participants were provided with brief information about the study aims and procedures and provided online consent.
Measures
Demographic and medical information
Participants were asked to self-report their age, gender, ethnicity, relationship status, and level of education. They also self-reported information about their cancer (type, age at diagnosis, type of treatment, and time since treatment completion).
Feasibility
Feasibility was assessed with five questions. Participants were asked to rate appropriateness of the length of the survey, the number of questions asked, and the type of questions. Participants were asked to rate how burdensome and distressing they found the research. They answered on a scale from 0 (least appropriate, burdensome or distressing) to 100 (most appropriate, very burdensome, or distressing). We also assessed how many people failed to complete or abandoned the survey after having consented to participate.
Centrality of event scale
The centrality of event scale (CES) 15 is a 7-item scale that asks individuals to what extent a stressful or traumatic event affects their sense of being and identity. The scores range from 0 to 28, and higher scores mean that the event serves as a stronger reference point in one's life. It has previously been used in cancer populations. 9
Cancer-related worry
This 6-item scale asks about the degree respondents agree with different worries related to cancer 6 (e.g., fertility, relapse) on a 4-point Likert scale ranging from “strongly disagree” to “strongly agree.” The scale has been developed and validated in a Canadian AYA sample. 6
Mental Defeat Questionnaire
The Mental Defeat Questionnaire (MDQ) 16 is an 11-item questionnaire, which asks about individuals' perceptions of their state during a traumatic event (in this case, cancer illness). Agreement with statements such as I lost any will power, I gave up, and I felt like an object are rated on a 5-point Likert scale from 1 (not at all) to 5 (very strongly). Higher total score indicate higher presence of mental defeat during the stressful or traumatic event (in our case, cancer).
Ruminative response style
The ruminative response style (RRS) 17 -10 is a 10-item scale rated on a 4-point Likert scale from 1 (never) to 4 (always) derived from the original 22-item scale. 18 The questions ask about one's general way of addressing negative emotions such as I think about how alone I feel. The total scores range from 10 to 40, with higher scores indicating higher levels of rumination.
Generalized anxiety disorder
The generalized anxiety disorder (GAD) 19 -7 is a 7-item measure of anxiety symptoms over the previous 2 weeks. Items are scored on a 4-point Likert scale from 0 (not at all) to 3 (nearly every day). A sum score of 7 or above can indicate the presence of clinical anxiety. 20
Analyses
We carried out exploratory analysis to look at associations between anxiety and other variables of interest described above, and also report Spearman's correlations. All analyses, data manipulations, and data visualizations were carried out using R Version 3.4.3. The analysis scripts can be found at https://psyarxiv.com/d3cjy
Results
Participants
Twenty-one AYAs participated in this online pilot study. Demographic and medical information is summarized in Table 1.
Patient Characteristics
Participants failed to report their diagnosis.
n = Number of available responses for each variable. % = Percentage of total sample.
SD, standard deviation.
Feasibility
Out of 23 respondents who consented to participate, 20 (87%) completed the entire survey, and 1 respondent did not complete 2 questionnaires. Participants reported the length, type, and number of questions to be appropriate. Only 1 participant found the survey distressing (80/100), and none found it burdensome.
A direct link to the survey was circulated on Twitter and Facebook. In addition, several patients, health professionals, and cancer charities based in the United Kingdom reposted our advertisement. Most participants were recruited on the day or the day after the advertisement appeared, suggesting that continued social media engagement is required for larger samples and broader reach.
Cancer identity
Thirteen of 20 (65%) participants who completed the CES reported their cancer or cancer-related event as the most stressful or traumatic experience in their life. Among these 13 participants, cancer or cancer-related events formed an important part of their identity. The scores ranged from 10 to 24, with 12 of them scoring 18 or above. Among those who reported cancer or cancer-related events as stressful or traumatic and scored 18 or above on the CES, 4 were under 24 months since treatment completion, and 6 were over 5 years since treatment completion.
Cancer-related worry
All participants responded to the cancer-related worry questionnaire. The scores ranged from 2 to 15, with a mean score of 8.5 (SD = 3.2). Worry about receiving a new cancer diagnosis was the most prevalent (66.7%), and more than half of the participants also worried about experiencing a relapse or experiencing late effects related to their cancer treatment. Figure 1 shows the proportion of participants who worry about a specific aspect of their illness or lived experience.
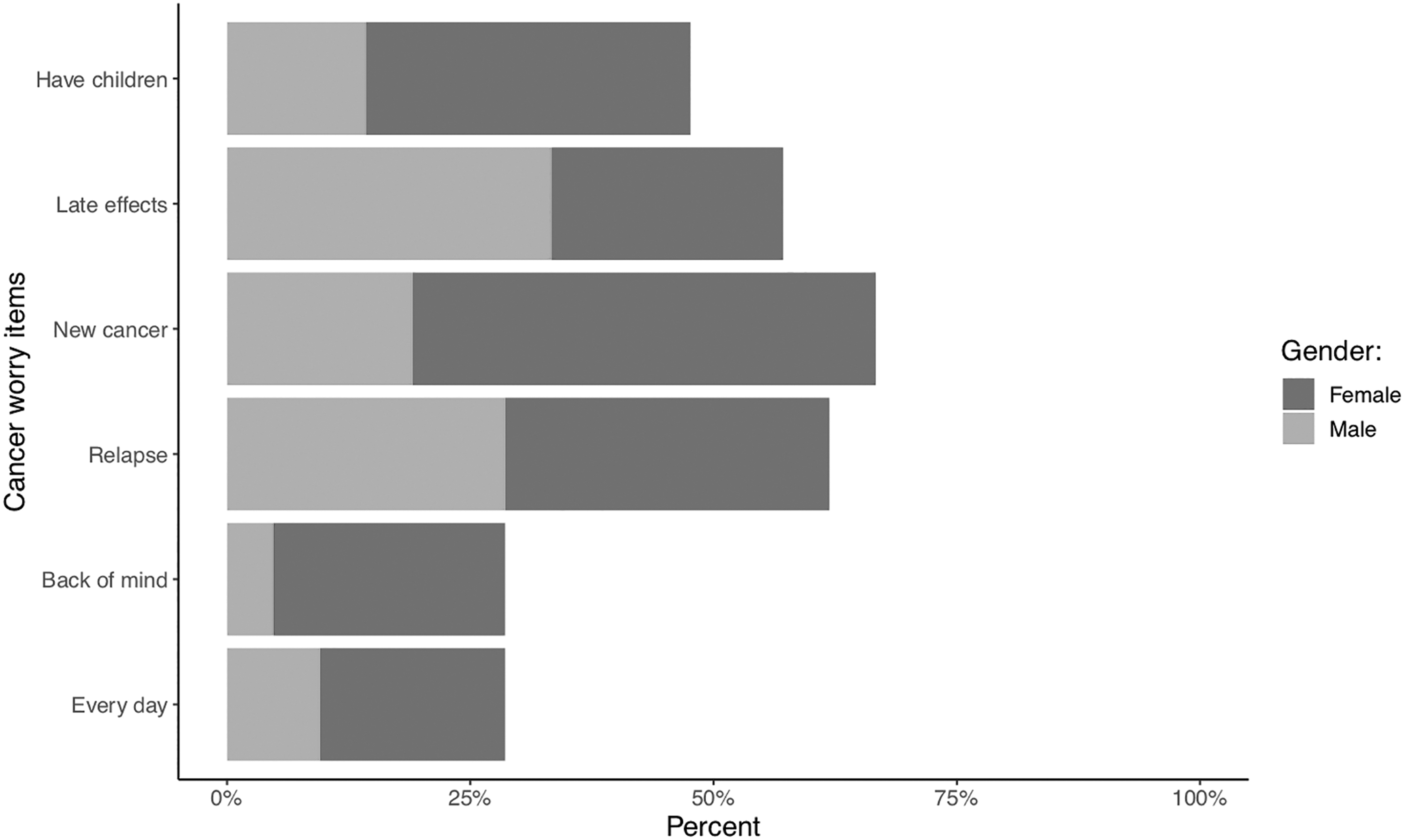
Proportion of participants who worried about an aspect of their illness. Have children = worry about having children in the future; Late effects = worry about experiencing late effects related to treatment; New cancer = worry about receiving a new cancer diagnosis; Relapse = worry about their cancer coming back; Back of mind = cancer being always at the back of their mind; Every day = worry about cancer every day.
Anxiety, Mental Defeat, and rumination
All participants responded to the MDQ and GAD-7 and 20 participants completed the RRS. The scores on the MDQ ranged from 0 to 44, mean = 11.4 (SD = 12.8). The scores on the RRS ranged from 10 to 27, mean = 20 (SD = 6.96), and on the GAD-7 from 0 to 16, mean = 5.9 (SD = 5.55). Using Spearman's correlation, the GAD-7 was positively associated with mental defeat (r = 0.40, p = 0.07), and RRS (r = 0.743, p < 0.001), while there was no association between GAD-7 and cancer worry. To take a closer look at individual data points and associations between these constructs, the data are presented in Figure 2.

Individual scores on the GAD scale combined with Mental Defeat, Rumination and Cancer worry. The graphs represent individual scores of anxiety on y-axis against (
Conclusion and Future Directions
This exploratory pilot study was guided by two aims: to assess the feasibility of conducting online research with AYA cancer patients and to explore the relationship between modifiable cognitive mechanisms and anxiety. Our results suggest that online research with AYA cancer populations is feasible; however, recruitment relies on continuous social media engagement by researchers and participating stakeholders. Our results also highlight that cancer or cancer-related events are significant stressors for the majority of young cancer survivors. All AYA cancer patients and survivors worried about at least one aspect of their cancer. Mental defeat during illness and a ruminative coping response emerged as mechanisms worthy of further investigation in longitudinal studies of psychological distress in survivorship.
In our study, 62% of participants reported their illness or cancer-related events to be the most stressful events in their lives. For these participants, cancer formed a significant part of their sense of self and identity. Interestingly, we note that time since treatment did not seem to be associated with the perception of magnitude of cancer or cancer-related events, suggesting that cancer might have a stable and long-lasting effect on one's identity. This aspect is important to consider as previous work suggests that those who identify more as “cancer survivors” also tend to report poorer quality of life and psychological functioning. 9 It is important to note that young people will have varying degrees of exposure to stressful or traumatic events. The trajectory of adaptation to life with and after cancer might be different for those who face multiple adversities (e.g., abuse, death of a parent). Cancer should not be automatically assumed to be a traumatic event and future studies should control for the level of adversity one has experienced prior or during their illness, as well as further explore the role of cancer identity on psychological functioning.
In addition to cancer identity, we assessed cancer-related worry, mental defeat, and rumination as three modifiable factors linked to anxiety. Cancer-related worry has been identified as a contributing factor to loss of AYA patients to follow up, 6 which can compromise health in the long-term. The three most common worries in our sample—relapse, late effects, or new cancer—may well be justified. Given that late-effects are a real threat for AYA cancer survivors, 21 the important question to ask will be at what point do these worries become pathological and overwhelming for the young person. Cancer-related worry should be assessed in longitudinal studies to better understand its direction and association with clinical anxiety in the survivorship phase.
Our exploratory analysis suggests a relationship between mental defeat, rumination, and anxiety. Feeling defeat during the time of illness might enhance perceived stress and the negative experience of cancer, which could lead to poorer psychological adaptation. However, we observed that some individuals who experienced mental defeat also report low level of current anxiety. RRS also indicates that it might play a role in anxiety among AYA. Association between rumination and anxiety has been established previously. 22 It is important to note that mental defeat was assessed retrospectively for the majority of our participants, and our cross sectional pilot study cannot yield information about the direction of effects. It is possible that current psychological distress might in turn influence the answers to both response style questionnaire as well as mental defeat. A longitudinal approach will help in providing a fuller picture of these processes.
There is a consensus in the literature that one's understanding and perception of cancer has a stronger impact on one's psychological adaptation than objective clinical or sociodemographic factors.5,23 Studying cognitive mechanisms such as mental defeat, rumination, or cancer-related worry and their relationship to mental health provides an avenue to developing novel and tailored psychosocial approaches to care, which are currently lacking. 24 Moreover, these mechanisms could be addressed via multiple avenues, from cognitive-behavioral therapy to informing oncological teams on how to best convey the risks of relapse and help attenuate the worries about late-effects.
Limitations
This is a pilot study for which we utilized a convenience sample of self-identified cancer survivors, who were invited to participate via social media. This makes the data prone to self-report bias as well as retrospective bias when participants answered questions about their past experience. The sample size is small, which prevents us from making statistical inferences. Even though the age range at diagnosis is wide, the group reflects the most common cancer types in this age range. 25 The time since treatment completion also varied, which may have resulted in recall bias, when asked about mental defeat during their cancer experience. We included gender in our figures; however, our sample is too small to discuss any gender differences. As it is often noted that women report higher levels of mental distress, 5 gender should be controlled for in a larger study. Nevertheless, the preliminary findings presented here are important in informing the development of future research.
Footnotes
Acknowledgments
The authors thank all the participants who took time and volunteered in our online study. The first author acknowledges the support of Economic and Social Research Council (ESRC) and Ad Futura for her doctoral work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.