
Abstract
Purpose:
With an increasing focus on developing survivorship services tailored for adolescent and young adult (AYA) cancer survivors, incorporation of viewpoints from both survivors and health care professionals (HCPs) is important. This study aims to explore the perceptions of current and prospective survivorship services from both groups in Singapore to propose service design and delivery strategies.
Methods:
Focus group discussions with 23 AYA cancer survivors between the ages of 16 and 39 years at diagnosis and 18 HCPs were conducted in National Cancer Centre Singapore (NCCS) and Singapore Cancer Society (SCS). All focus group discussions were transcribed verbatim. Deductive thematic analysis was performed according to the components of a design thinking model: empathizing with AYA survivors, defining care gaps, proposing services, and implementation strategies.
Results:
AYA survivors preferred age-specific services that are aligned with their personal goals. Current survivorship care failed to address the needs of survivors' dependents (caregivers and children) and to consider the utility of each service temporally. Prospective services should clarify disease disclosure obligation in job search and introduce a care navigator. Key implementation strategies included (1) training HCPs on communication techniques with AYA, (2) selecting engagement platforms that complement survivors' information-seeking behavior, (3) improving outreach to survivors through appropriate branding and publicity, and (4) consolidating services from multiple providers.
Conclusions:
The design of survivorship care services for AYA survivors should be systematic in its conceptualization process and employ implementation strategies. The coordination of the wide spectrum of services warrants a concerted effort by cancer centers, community partners, and the government.
Introduction
In 2018, 6.8%
A growing body of literature has elucidated AYA cancer survivors' diverse needs.9,13–17 There are increased global efforts to build AYA-specific cancer survivorship programs that address these developmental needs holistically.18–20 However, the current provision of survivorship care services remained inconsistent and unorganized in the Asia-Pacific region, including high-resource countries like Singapore where services are segregated by cancer types without age specificity.21–25 As AYA cancer survivors experience a higher psychosocial distress and morbidity burden compared with their cancer-free peers, this segregation would result in services that do not comprehensively and adequately address the unique age-related challenges AYA face. 26 Thus, a change is needed for better management of AYA survivors' needs to improve their quality of life.27,28 In particular, this occurrence underscores the need for a concrete framework to guide the design of beneficial and engaging services in the Asian context.
Existing studies on survivorship service design are limited in two ways. First, the discussion of such services is usually framed in the context of addressing gaps in care needs or serving as examples for contextualizing the principles of survivorship follow-up care provision.29–34 Thus, current recommendations for a systematic survivorship service construction lack granularity and specificity. Second, only a few studies have incorporated the perspectives of health care professionals (HCPs) who play a paramount role in designing and initiating such survivorship services in tertiary and community settings. To address these gaps, this study explores the perceptions of current and prospective survivorship services from dual viewpoints of AYA cancer survivors and HCPs. This study aims to identify desirable AYA survivorship services with the corresponding design and delivery strategies to improve service implementation in Singapore.
Methods
This study analyzed focus group data from a larger qualitative study examining AYA-specific survivorship care needs and the corresponding desirable survivorship care services. Ethical approval was obtained from the SingHealth Institutional Review Board and written informed consent was obtained from all study participants.
Study participants
Figure 1 summarizes the participant enrolment process. Survivors of AYA cancers receiving care from National Cancer Centre Singapore (NCCS) were identified through convenience sampling during two periods: July to October 2017 and July to October 2018. Recruitment was performed in-person or through email. Survivors were eligible if they met the following criteria: 16–40 years old at time of recruitment, 6 months to 4 years from diagnosis, and currently in remission. Survivors were excluded if they were diagnosed with severe concurrent comorbidities like HIV infection, uncontrolled diabetes, or neuropsychiatric disorders that could confound their responses.
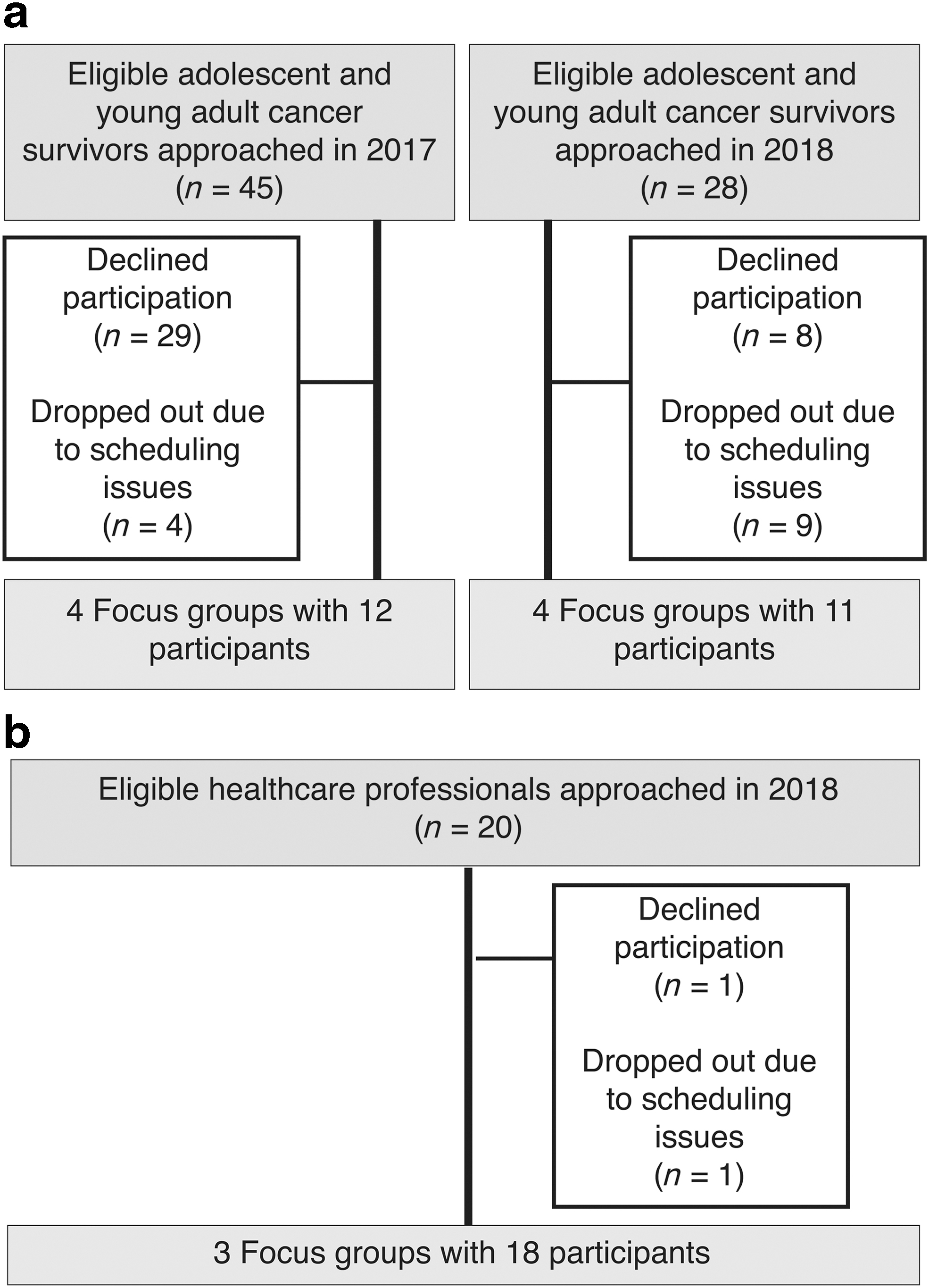
Enrolment process of the study participants who are
HCPs were recruited from Singapore Cancer Society (SCS) and NCCS in July to October 2018 through snowball sampling from study team members (A.C. and B.S.). Potential participants were contacted through email. HCPs with a personal history of cancer were excluded.
Focus group discussions
Eight focus groups involving AYA survivors and three focus groups involving HCPs were conducted on the NCCS and SCS premises between September 2017 and September 2018. Each group consisted of two to six participants, one moderator, and one note taker. Each session lasted 60–90 minutes and was facilitated by trained moderators using a standardized facilitator guide developed to understand the current and prospective AYA survivorship services (Table 1). The moderators (C.J.T. and Y.K.) were research pharmacists with no professional relationships with the participants before the sessions and were not involved with recruitment.
Relevant Portions of the Facilitator Guide Used in Focus Group Discussions
AYA, adolescents and young adults; HCPs, health care professionals; NCC, National Cancer Centre.
Before each session, all participants were asked to complete a demographic survey on their age, gender, and race. AYA survivors were further asked about their age at diagnosis, marital status, education level, employment status, current monthly income, and living arrangements. HCPs were further asked about their professional discipline, primary specialty, practice setting, health care experience, and proportion of time spent caring for AYA cancer survivors. Focus groups began with introductions by all participants before the facilitator inquired about the existing or prospective survivorship care services for AYA cancer survivors. Each participant was reimbursed USD36 in cash vouchers for his/her transport cost and time.
Data analysis
The demographic data were summarized using descriptive statistics. All focus group discussions were audio recorded and transcribed verbatim. Two study team members (C.J.T. and Y.K.) reviewed and coded the transcripts independently according to the major themes outlined in a design thinking model proposed by the Hasso-Plattner Institute of Design. 35 The model consists of five key components to guide service designers: empathizing with the population of interest, defining gaps, ideating, prototyping, and testing of the proposed services. All deductive thematic data analysis was performed in QSR NVivo 12. 36 The thematic structure was then refined through discussions between the two members to resolve all differences and achieve mutual agreement. Data saturation was deemed to have occurred when the focus groups yielded no new themes.
Results
Study participants
Table 2 summarizes the characteristics of the 23 AYA cancer survivors and 18 HCP participants. The median age of survivors was 25 years old and ranged from age 18 to 39 years. All survivors attained a minimal college education, and 65.2% were employed at the point of survey. HCP participants included physicians (33.3%), social medical workers (22.2%), allied health therapists (22.2%), nurses (16.7%), and a patient navigator. Most had >10 years of experience (61.1%) and spent <20% of their time with AYA cancer patients (61.2%).
Characteristics of Study Participants
Coding tree
Table 3 provides quotes from the five major identified themes. The characterization of the AYA group contextualized their engagement with survivorship care services and highlighted gaps in current service provision. Proposals for prospective services were then explored with insights on implementation strategies.
Themes, Subthemes, and Selected Quotes from Focus Group Discussions
TAFEP, Tripartite Alliance for Fair and Progressive Employment Practices; TCM, Traditional Chinese Medicine.
Understanding AYA survivors
The characterization of AYA survivors by HCPs highlighted key traits that influence survivors' engagement with survivorship services. In contrast with other age groups, HCPs observed that AYA survivors were highly resilient, self-motivated, and goal-oriented. Survivors also emphasized that they were inclined to engage in services that were useful in achieving their personal progression goals and interests. Consequently, a sense of autonomy was appealing to survivors who then exercise their freedom of choice to participate in services based on their knowledge of possible alternatives. Survivors also cited differential motivation based on personal characteristics where participation was associated with extroverts or outgoing personalities. Another factor was the survivors' willingness to being reminded of their cancer diagnosis and disease history.
Furthermore, survivors generally prioritized age specificity when services engage multiple survivors concurrently. Based on past experiences of interacting with non-AYA survivors, some AYA survivors reported discomfort because of their minority presence in the setting and their fear of judgment by non-AYA survivors for their diagnosis at a young age. In addition, meaningful interactions were hindered by different priorities and worries associated with the transitional life stages of AYA. For instance, non-AYA survivors' advice on slowing down the pace of life after treatment was not compatible with AYA survivors' drive to return to work. Moreover, different levels of disease understanding also resulted in the exchange of mismatched information between AYA and non-AYA survivors.
Defining AYA survivorship care gaps
AYA survivorship services should consider the multiple roles that AYA play in relation to their family members. Most AYA participants had children as dependents or parents as caregivers. For survivors with children, HCPs emphasized the importance of financial assistance schemes or tuition sessions tailored to the child's needs. For AYA participants with caregivers, they expressed a greater interest in services that could guide their caregivers in the caregiving process. These services should address appropriate diet planning for survivors, provide relevant psychological advice to caregivers, and moderate caregivers' expectations.
Another gap in survivorship care pertained to a lack of consideration of each service's utility temporally. For instance, existing support groups were perceived by both AYA survivors and HCPs as valuable platforms for the informal exchange of experiences to establish empathetic connections and to share coping mechanisms. However, the value perceived by AYA survivors was more pronounced in the acute treatment phase. Although support groups offer a compensatory mechanism for their temporary loss in existing social relationships, their utility diminished in the later survivorship phases. Of note, HCPs reported a drop in survivors' attendance over time, and survivors revealed that sustained participation was challenging because of busy work or schooling schedules.
Proposals for prospective survivorship services
Survivors' awareness of existing survivorship services varied because of their unorganized arrangement and publicity. Participants received services mainly from cancer centers, and all survivors showed poor knowledge of external providers. Nevertheless, key services highlighted for continuation were support groups and allied health services including ad hoc nutritional and financial advice.
Both survivors and HCPs agreed that future employment services should clarify disease disclosure obligations as many deemed the cancer history to be disadvantageous in the job search process. Correspondingly, HCPs proposed general education programs among employers to raise awareness and assist survivors in their job search. Conversely, some survivors did not emphasize the need for designated job search assistance because they perceived it as an active process that is driven by self-capability. Instead, they sought to seek assurance from the government or recognized agencies such as the Tripartite Alliance for Fair and Progressive Employment Practices (TAFEP) that their cancer history would not lead to discrimination by prospective employers.
The creation of a care navigator role was a recurring recommendation by both survivors and HCPs to serve as a continuous contact point in each survivor's journey from diagnosis to survivorship. The navigator would facilitate the consolidation of all possible relevant services such as patient support groups, counseling services, and reliable information services. Furthermore, the navigator should introduce these services concomitantly with existing treatment plans to maximize their utility and incorporation potential. However, the expertise of providing emotional counseling services was not reinforced. One HCP compared the job with that of a transplant coordinator.
Implementation strategies to engage AYA
Both survivors and HCPs concurred that service implementation should consider practical features such as cost, location, and timing. In addition, HCPs advocated for the provision of training or guidance on effective communication techniques with the AYA age group and their unique coping mechanisms. Survivorship service providers should also conscientiously select engagement platforms such as interactive hotlines, physical meetings with HCP or survivors, and the internet to communicate details about survivorship services. Among these possibilities, the internet emerged as a promising and convenient portal that complemented survivors' online information-seeking behavior. Most survivors reported attempts to use the World Wide Web (including Google) to obtain cancer-related information.
Several modes were explored through the internet: noninteractive webpages, messaging, and web forums. The display of information online should be comprehensive and free from the excessive use of jargon or medical terms. Messaging services were considered useful when interactions between survivors are dependent on their respective busy work schedules. Finally, the forum should allow survivors to share and respond interactively to one another's experiences. Both survivors and HCPs proposed a centralized platform to consolidate all modes of information into a single common site or channel. Survivors generally echoed a need for information regulation to ensure its credibility. However, no consensus was reached among survivors over the appropriate authority to assume this responsibility where government, cancer center, and the national cancer society were suggested.
Improving service outreach to AYA
Adequate branding and publicity to promote the constructed services were highlighted to be instrumental in improving its outreach to the AYA group. Survivors perceived the use of social media to promote services favorably. Coupled with publicity efforts, HCPs further elaborated on the importance of branding. Services should embed relevant counseling elements into popular or conventional activities that are appealing to AYA. Expanding on this branding strategy, HCP also introduced a “safe space” concept to describe the creation of a physical or virtual setting where survivors would feel comfortable sharing their concerns and would benefit from a greater immersion in survivorship services. This concept was epitomized in a survivor's narrative where a virtual chat group served as her emotional anchor throughout treatment. For instance, issues that were sensitive and gender-specific, that is, menstruation or physical imagery, were discussed freely with the trust of confidentiality within the group.
The prospect of service integration across multiple providers was explored to optimize outreach to the same pool of AYA survivors. HCPs from cancer advocacy and support organization (SCS) advocated for the centralization of service provision and referrals to avoid duplicity. However, they also acknowledged that this proposal detailing a designated pathway following service referral might limit survivors' choices and hinder their ability to maximize resources from various services. In addition, consolidation would require harmonizing divergent perceptions on the roles of various service providers from HCPs in tertiary cancer centers to other institutions.
Discussion
This qualitative study identified desirable AYA survivorship services and explored delivery strategies from the perspectives of both service recipients and providers in Singapore. The significance of analyzing these two viewpoints is twofold: proposals supported by both stakeholders should be expedited into actualization, and misaligned suggestions highlight areas for future work and clarification. Furthermore, the emerging themes collectively shaped a proposed systematic framework for the design of survivorship services for AYA (Table 4).
Systematic Framework for the Construction of Survivorship Services
Although existing services such as support groups were deemed valuable, their long-term utility and relevance to survivors remained questionable years after treatment. As a service may be useful only for a specific survivorship phase, this temporal phase targeted must be well-defined in the conceptualization stage. The consideration of the temporality factor corroborated with previous work, which framed survivors' concerns in “survivor time.” 37 The survivorship phase is segmented by complex trajectories defining survivors' readjustment to normalcy where they deal with their fear of recurrence and reconcile with their new beliefs. 37 Correspondingly, useful services should collectively be comprehensive for the long-term despite being individually transitory in nature. Thus, service conceptualization should be explicit in its targeted time frame to create constructive programs that assist AYA in developing meaningful goals. Furthermore, to address the differential needs among AYA, the targeted age group within the AYA spectrum should be identified. 38 For instance, literature on the “emerging adulthood” has highlighted a greater unmet need among younger than older AYA. 39 This trend could be partly attributable to the larger impact after formal decisions relating to employment, education, and independent living for those at the younger end of the AYA age spectrum.
For the possible service types, prospective services should complement AYA cancer survivors' information needs. An online platform was proposed to integrate multiple information sources to assist survivors in systematically navigating through the available services. The internet is suitable for AYA survivors' information-seeking behavior and practical convenience.40–42 Successful examples in Western settings include the Livestrong Foundation's portfolio of interactive internet-based resource products spanning across social media 43 and the AYA Cancer Program at the University of South California. 44 For instance, hyperlinks to fertility counseling services are an extension of information on post-treatment fertility concerns. The ease of access to comprehensive information also creates a strong basis to support autonomous decision-making by survivors. Furthermore, the institution of a regulatory authority is critical in ensuring the credibility of information. Consistent concerns over the reliability of information sources have also been reported in the literature as AYA survivors struggled to find tailored and trustworthy information online.30,41,45
Extrapolating these findings to Asian settings, a similar model of information and service provision can be constructed by leveraging existing infrastructure designed to enhance the public's health information literacy. In a high-resource country like Singapore, the existing HealthHub portal initiated by the Ministry of Health can be expanded to provide AYA-specific information and facilitate access to corresponding services based on their personal health records. 46 Spearheaded by the ministry, additional partnerships with public health institutions and authorities can accommodate varying preferences of regulatory organizations expressed by survivors.
In addition, collaboration opportunities between service providers at a national (or regional) level can be explored to reduce duplicity and maximize outreach to the AYA population. However, two challenges underlie such collaborative efforts: (1) determining the organization body that assumes responsibility of service referrals coordination; and (2) ensuring diversity in the range of service options for survivors. The successful implementation of an AYA Program at Princess Margaret Cancer Center can shed light on how these challenges can be managed. 47 Based in a tertiary setting, the AYA Program provides referrals to survivorship services offered by the center's transdisciplinary team and interfaces with community-based programs.
Cancer centers are in an appropriate position to coordinate service referrals because they appeal to a sense of familiarity among AYA cancer survivors and leverage their positive relationship with HCPs to improve their long-term engagement with the health care system. 48 Recognizing the inherent multidisciplinary nature of care for AYA survivors (e.g., clinical care, psychosocial support, financial counseling, and education), existing services in cancer centers could be maximized for efficient resource utilization. 49 External or community-based service providers could then play a pivotal role in supplementing the service infrastructure in tertiary settings with AYA-specific elements or tailored services to encourage diversity in the range of services.
Overall, the proposed survivorship design framework encapsulates various considerations and is complemented by available resources to facilitate the process. Although this study focused on service design and engagement strategies, an equal emphasis should be placed on a robust evaluation framework to determine the service's feasibility, acceptability, and effectiveness.50–52
This study has several limitations. First, as AYA participants were recruited from their follow-up clinic sessions, our results may not be representative of AYA survivors who were lost to follow-up. This group can potentially provide greater insights into survivorship care services that could improve care continuity within the health care system. The inclusion of survivors in remission also precluded discussion on services targeting palliative issues. Finally, the majority of the participating HCPs only spent <20% of their time providing direct care to AYA survivors, potentially compromising the depth of the perspectives shared. Recognizing that AYA constitutes a small proportion of the cancer population with no dedicated clinics, this phenomenon is expected. Nevertheless, their viewpoints remained valuable because they were able to contrast their encounters with AYA against non-AYA survivors.
Conclusion
The findings of this qualitative study highlight proposals to engage AYA cancer survivors in useful survivorship services through the conceptualization process, implementation features, outreach potential, and evaluation measures. This study also accentuated the need for a concerted effort by various stakeholders including specialty cancer centers, external community partners, and the government. Future work should operationalize the proposed framework to design and evaluate prospective services. In addition, possible care models and partnerships involving community HCPs should be explored and maximized to promote the long-term well-being of AYA survivors.
Footnotes
Disclaimer
The key results from this article have been presented as a poster at the Multinational Association of Supportive Care in Cancer Annual Meeting 2019 in San Francisco.
Author Disclosure Agreement
No competing financial interests exist.
Funding Information
This study was supported by the National Medical Research Council (NMRC/CIRG/1471/2017) and the Singapore Cancer Society Internal Research Grant.