
Abstract
Purpose:
Testicular cancer (TC) is considered the most commonly diagnosed malignancy in males between 15 and 34 years of age. The objective of this study is to systematically review and meta-analyze studies on fatherhood following treatment for TC.
Methods:
We reviewed studies reporting on fatherhood following TC from Medline and Embase search engines by developing search strategies. Only studies including patients with TC and at least one reproductive variable were considered as part of the analysis. Estimate of heterogeneity was calculated using the I2 statistic. Meta-analyses employing a fixed effects model were also applied as an additional measure of sensitivity.
Results:
A total of 27 studies were included which reported on fatherhood after treatment for TC. A meta-analysis of included studies with subgroup analysis was conducted. Subgroup analysis, for the combined studies, indicated an overall pooled pregnancy rate of 22% (95% confidence intervals [CI]: 0.21–0.23; I2 = 98.1%) for couples who conceived after TC. Of those couples that became pregnant, 11% (95% CI: 0.07–0.16; I2 = 8.5%) experienced a miscarriage. Fatherhood was experienced by 37% (95% CI: 0.35–0.39; I2 = 98.1%) of males following treatment for TC.
Conclusions:
Male cancer patients should be offered discussions, information, and counseling regarding the impact that TC treatment can have on fertility. Furthermore, sperm banking must be recommended to all patients before starting treatment.
Background
Testicular cancer (TC) is considered the most commonly diagnosed malignancy in males between 15 and 34 years of age; however, this malignancy only accounts for 1% of all newly diagnosed male cancers. 1 Patients with this diagnosis have a 95% five-year cancer-specific survival rate. 2
More than 95% of testicular tumors are diagnosed as testicular germ cell tumors (TGCTs). 3 Germ cell tumors (GCT) comprise of ∼98% of TCs. 4 Other GCTs include stromal tumors (2%), such as Leydig cell (∼0.2%) and Sertoli cell tumors (∼0.1). Approximately 55% of TGCTs are considered classic seminomas, 44% are nonseminomas (embryonal carcinomas, teratomas, yolk sac tumors, choriocarcinomas), and 1% are spermatocytic seminomas. 4
The incidence of TC varies by ethnicity, with the highest rates reported in developed countries such as Norway (11.8/100,000) and the lowest in developing countries such as in India (0.5/100,000) and Thailand (0.4/100,000). 5 There is an increased incidence of TGCTs diagnosed in young adult males, with most (84%) diagnosed between the ages of 15 and 44 years. Less than 20%, occur in males ≥45 years of age. The incidence of nonseminoma peaks when a male is ∼25 years of age, while the incidence of seminoma peaks in older males around the age 35 years. 6
Treatment outcomes can have variable effects on spermatogenesis, which is highly correlative to the quality of a patient's sperm before the start of gonadotoxic treatment as well as numerous other factors, including age at diagnosis, tumor type, drug characteristics (including novel drugs), treatment regimen, site of administration of treatment, and length of treatment. 7 Radiotherapy and chemotherapy can either temporarily or permanently impair spermatogenesis,8–11 and retroperitoneal lymph node dissection (RPLND) may be followed by dry ejaculation, in which surgery to sympathetic nerves and ganglia can cause loss of seminal emission into the posterior urethra or true retrograde ejaculation.12,13 The introduction of unilateral and/or nerve-sparing RPLND 14 and surveillance as primary therapy options after orchiectomy 15 are considered appropriate treatment strategies to assist with preserving a patient's fertility. Other possible strategies for preserving fertility include limiting the radiation fields to the para-aortic area, 16 lower doses of both radiation therapy 17 and chemotherapy. 18
Studies report that approximately a quarter of male cancer patients will experience azoospermia following treatment. 19 Three quarters of patient's will present with a decrease in baseline spermatogenesis,11,20 mainly due to existing defects in spermatogenesis, a medical history of cryptorchidism, antisperm antibodies, as well as possible contralateral or intraepithelial germ cell neoplasia and generalized stress associated with illness.19,21 Studies conducted by Stephenson et al. 22 and Matos et al. 23 reported a drop in fertility rates, by half (49%), following treatment with gonadotoxic therapy, with baseline fertility rates at 82% before the start of treatment.
Lampe et al. 8 reported follow-up sperm counts of TC patients before and then 1 year post-treatment, revealing normal sperm count pre-treatment, with 16% presenting with oligospermic (<20 million sperms/mL) and 20% presenting azoospermic post-chemotherapy. Comparatively, it was also reported that in TC patients who presented with oligospermia before the start of treatment, only 24% had reached a normal sperm count 1 year post-treatment. 8 Additionally, cryptorchidism, where one or both of the testes fail to descend from the abdomen into the scrotum, has been reported to be correlated with both TC and infertility.24,25
Since TC is most commonly diagnosed in males of reproductive age, at the peak of their reproductive potential, undergoing treatment with surgery, chemotherapy, radiotherapy, or a combination of therapies can have irreversible effects on becoming a father. 26 Many studies report that male patients experience a number of clinical and psychosocial concerns in relation to their sexual and psychosexual dysfunction and subfertility or infertility following treatment.27,28 Surgery and radiation to the pelvis or lumbar spine has reportedly been linked to sexual dysfunction, as a result of hormonal deficiency and emotional distress. 29 Kenney et al. 29 reported that 20% of young adult male cancer patients experienced erectile dysfunction subsequent to treatment, and these findings were supported by several other studies revealing that more than half of all survivors presented with ejaculatory dysfunction following treatment.3,30 These consequential reproductive outcomes, in relation to fatherhood, can have a detrimental effect on a patient's physical and psychological wellbeing, maintaining relationships, and quality of life. 31 Hence, discussion and counseling around sexuality, reproductive function, and fertility preservation are important before starting gonadotoxic treatment. 32
Currently, the most common and efficient option for fertility preservation in males is sperm banking through masturbation, and its subsequent use in assisted reproductive technologies (ART), either with the use of in vitro fertilization or intracytoplasmic sperm injection, for those desiring a biological family.7,33–37
Semen quality may be reduced before a patient undergoes treatment with an orchiectomy for TC and sperm count and concentration can further decrease after this procedure.8,13,38–40 The European Society for Medical Oncology (ESMO) recommends patients who receive chemotherapy or radiotherapy following an orchiectomy should be encouraged to undergo sperm banking, as their fertility may be further decreased compared with those patients who undergo treatment with an orchiectomy alone.8,13,38–42 However, fatherhood may still be possible following treatment through natural conception or in vitro fertilization (IVF). 42
The aim of this systematic review and meta-analysis was to investigate and report on fatherhood following treatment for a testicular malignancy in male patients.
Methods
Search strategies
This systematic review of the literature followed the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) Statement (Fig. 1) and PROSPERO (CRD42019136085). Highly sensitive search strategies were designed for the databases MEDLINE (OVID) 1980–July 2019 and EMBASE 1980–July 2019. Searches were conducted using terms such as “testicular neoplasm,” “testicular cancer,” “testicular germ cell cancer,” “seminoma,” “non-seminoma,” “teratoma,” embryonal cancers,” “choriocancers,” “yolk sac tumors,” “reproduction,” “fertility,” “fertilization,” “pregnancy,” and “birth.” Included articles were also checked for additional references. Both searches were limited to “English language” with “male” patients. Four authors (B.G., M.B., X.V., and A.K.) independently screened all citations and abstracts identified by the string search strategy to identify eligible studies. Reference lists, of articles that were screened, were checked to determine whether all pertinent literature was included.

PRISMA flow diagram of the study selection process. PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analyses.
Criteria for inclusion of studies
We first identified articles by examining titles, then abstracts to determine relevance, and then we retrieved the full text of the relevant abstracts for further assessment and review. Accordingly, we identified retrospective studies, population-based studies, cohort studies, randomized-controlled trials, and questionnaire studies (where data were presented on fatherhood that is the number of conceptions and/or subsequent birth outcomes). Among the criteria used in inclusion of studies were; (1) males diagnosed with a TC; (2) studies with adequate information on the method of ascertainment of fatherhood.; (3) studies where information was extracted from peer-reviewed journal articles; (4) medical record reviews or pathological reviews retrieved from participating sites described in the included articles; (5) questionnaires that presented data on reproductive outcomes for couples following TC 43 ; (6) studies published between January 1980 and July 2019; (7) studies that had a sample size greater than or equal to 10 participants; and (8) full-text studies that were published in English.
Studies were excluded: (1) if the study was not published in English and where we were unable to access a copy of the article translated in the English language; (2) qualitative articles that did not include reproductive data for males to be included in the analysis; (3) case studies, as most studies lacked robust quality reproductive data to include in the analysis and to reduce the potential for identifying a patient in this study; and (4) secondary works (e.g., review articles, commentaries, editorials, or dissertations/theses, or conference abstracts that had not yet been published).
Data extraction
The data collection tool was designed by two individuals (A.A., B.G.). Titles, abstracts, and keywords were independently reviewed by four individuals (B.G., M.B., X.V., and A.K.) and the full text for each included study was independently reviewed by four individuals (B.G., M.B., X.V., and A.K.). The full text was retrieved of any reference that gave an indication that it might contain data on at least one reproductive variable in relation to TC.
Data analysis
Descriptive statistics were used to analyze the frequencies, medians, and mean of demographic data (age, study design, tumor type, and stage). Statistical analyses were performed using STATA release 14.2 (Stata Statistical Software; Stata Corporation, College Station, TX).
Meta-analyses
Meta-analyses were conducted using a random effects model to allow for variation in true associations across studies.
44
Estimate of heterogeneity was calculated using the I2 statistic, which is the percentage of total variation in risk estimates attributable to genuine variation rather than sampling error.
45
Meta-analyses employing a fixed effects model were also applied as an additional measure of sensitivity.
46
Generally, heterogeneity is classified into the following three categories: heterogeneity less than 25% (low level of heterogeneity), between 25% and 75% (average level of heterogeneity), and more than 75% (high level of heterogeneity). Forest plots were used to present the combined estimate with 95% confidence intervals (CI). For studies which did not present a standard error (SE), we calculated SE using the formula; SE =
Results
Characteristics of included studies
Initially, 344 publications were searched from databases and other resources. After screening potentially eligible studies, 27 studies13,30,32,33,35,38,39,41,43,47–64 met the inclusion criteria and full texts were subsequently retrieved. The studies included: three retrospective review studies (11.11%)38,54,58; one prospective study (3.7%), 33 seven cohort studies (25.93%),13,49,56,57,60,62,64 four questionnaire studies (14.81%),47,48,50,59 three medical record review studies (11.11%),32,35,51 seven medical review and questionnaire studies (25.93%),30,39,52,53,55,61,63 one cross-sectional study (3.7%), 41 and one registry study (3.7%). 43 Most studies were conducted in Europe (n = 15, 55.56%),13,30,32,38,39,41,43,48,50,56–60,62 followed by The Americas (n = 8, 29.63%),33,49,51–55,63 Australasia (n = 3, 11.11%),47,61,64 and the Middle East (n = 1, 3.70%). 35 Table 1 highlights study characteristic, including TC treatment details, for each of the 27 included studies.13,30,32,33,35,38,39,41,43,47–64
Study Characteristics of the 27 Included Studies a
Brydoy et al., 13 Hartmann et al., 30 , Spermon et al., 32 Agarwal et al., 33 Botchan et al., 35 Huyghe et al., 38 Brydoy et al., 39 Huddart et al., 41 Gunnes et al., 43 Arai et al., 47 Babosa et al., 48 Beck et al., 49 Bohlen et al., 50 Chung et al., 51 Foster et al., 52 Fried et al., 53 Hakim et al., 54 Herr et al., 55 Hultling et al., 56 Lass et al., 57 Magelssen et al., 58 Molnar et al., 59 Ochsenkuhn et al., 60 Ping et al., 61 Rosenlund et al., 62 Sonnenburg et al., 63 Ukita et al. 64
Fatherhood through adoption.
—, not specified; ART, assisted reproductive technologies; RPLND, retroperitoneal lymph node dissection.
The study population consisted of 6439 males.13,30,32,33,35,38,39,41,43,47–64 diagnosed with TC (seminomas = 2156 [33.48%]13,30,32,38,39,41,47–49,53,57–62; nonseminoma = 3861 [59.96%]13,30,32,38,41,43,47–50,54,55,57–63; and unspecified = 422 [6.56%]).
Of those articles that reported on TGCT type and stage for male's diagnosed with a seminoma (n = 16 articles),13,30,32,33,35,38,39,41,43,47–64 24.37% were stage 141,53 followed by 8.83% who presented with stage 2.41,53 No staging was reported for the other 14 (66.8%) studies for this TGCT type.
For those articles that reported on nonseminomas (n = 19 articles),13,30,32,38,41,43,47–50,54,55,57–63 there were 3861 men diagnosed with this TGCT, including: teratomas (n = 26/312, 8.33%),38,48,54,60,62 embryonal (n = 190/478, 39.75%),38,48,50,54,61,62 choriocancers (n = 7/274, 2.55%),38,48 yolk sac (n = 8/380, 2.11%),38,54,61,62 and mixed tumors (n = 152/362, 41.99%).38,60,62 Only six studies reported on stage of TC; stage 1 (369/1330, 27.74%),30,41,49,50,55 stage 2 (64/285, 22.46%),30,49,54 stage 3 (17/98, 17.35%), 30 and stage unknown (32.45%).
Reproductive outcomes, in relation to fatherhood, following treatment for TC
Table 2 highlights reproductive outcomes, in relation to fatherhood, following treatment for a testicular malignancy for the combined studies.13,30,32,33,35,38,39,41,43,47–64
Meta-Analyses in Relation to Fatherhood for Each Reproductive Outcome Following Treatment for Testicular Cancer
—, Insufficient data to perform analysis.
CI, confidence intervals.
The rate of azoospermia, before starting treatment, reported in 11 articles,32,50,52,55–59,61,62,64 was 7.24% (n = 138/1907).32,55–59,61,62,64 Approximately 13.66%13,30,32,33,35,38,39,54,57–59,61,63 of male patient's banked sperm and 52.29% (n = 2834/5420)13,30,32,39,47,55,58,59,61–63 of couples attempted to conceive subsequent to treatment.
Subgroup analysis
There were 6439 males included in the combined articles, with a total of 1192 (22%) (95% CI: 0.21–0.23; I2 = 98.1%)13,30,32,35,38,39,41,43,47,51,52,54,56–62,64 conceptions following treatment for TC (Fig. 2) (median age at diagnosis was 30.7 years and at pregnancy or birth was 34 years). Table 2 details the number of conceptions, in relation to different cancer treatment options, following cancer therapy. There were 31.8% (n = 214)13,30,32,33,35,38,39,49,51,54,56–64 of couples that became pregnant using ART. There was only 1 article that reported on adoption in 27 (7.24%, n = 27/373) 13 males.
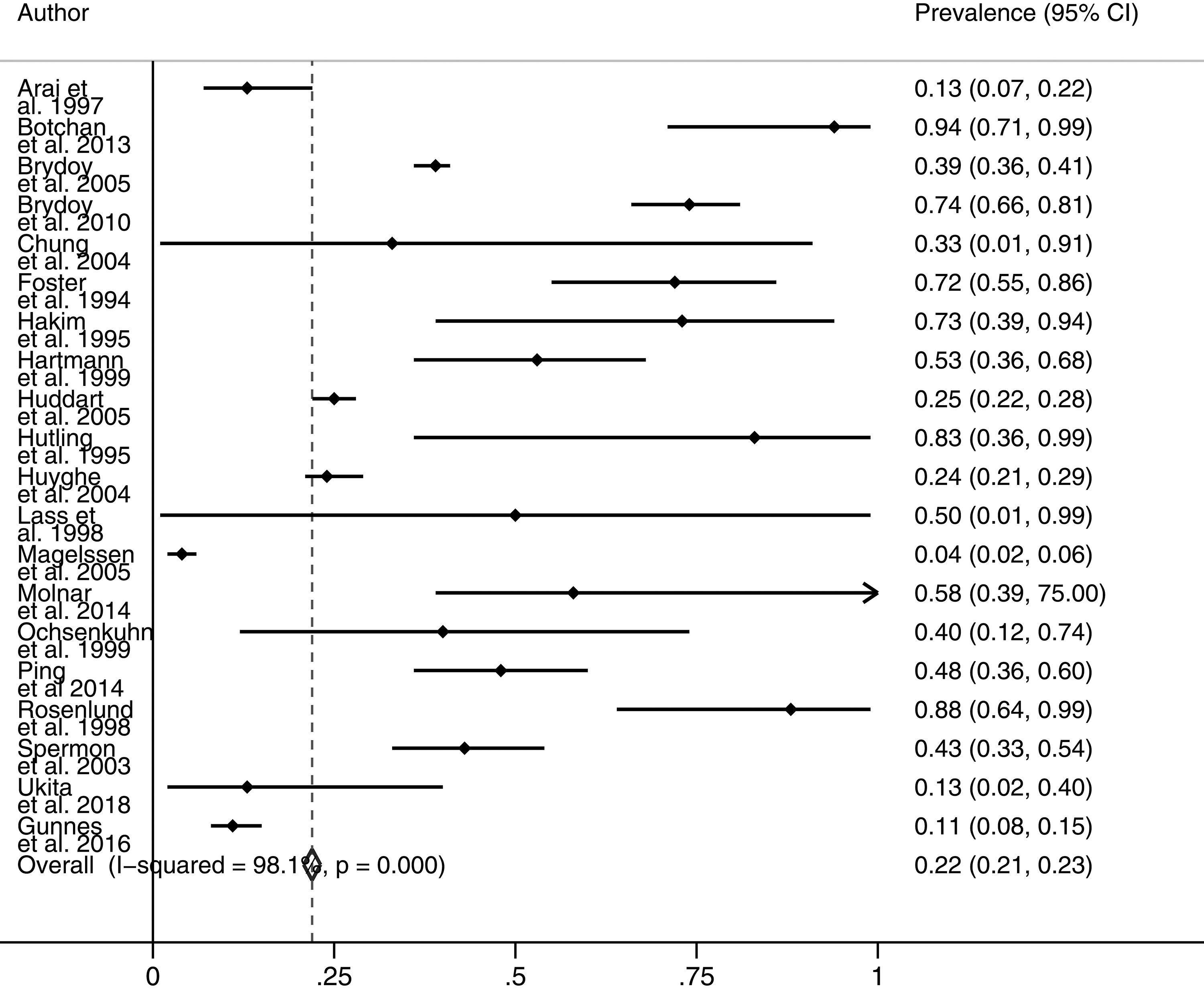
Number of pregnancies sired with a partner following treatment for TC (n = 1319). TC, testicular cancer.
Pooled miscarriage (<14 weeks) and medical terminations for couples were 11% (n = 25) (95% CI: 0.07–0.16; I2 = 8.5%)30,32,48,52,56,60–62,64 and 10% (n = 21) (95% CI: 0.05–0.15; I2 = 57%),48,52,58,59,61 respectively.
Of those couples that successfully conceived, fatherhood (live birth) was experienced by 37% (n = 993) (95% CI: 0.35–0.39; I2 = 98.1%)13,30,32,33,35,39,48–50,52,53–55,58,59,63 of males following TC (Fig. 3).
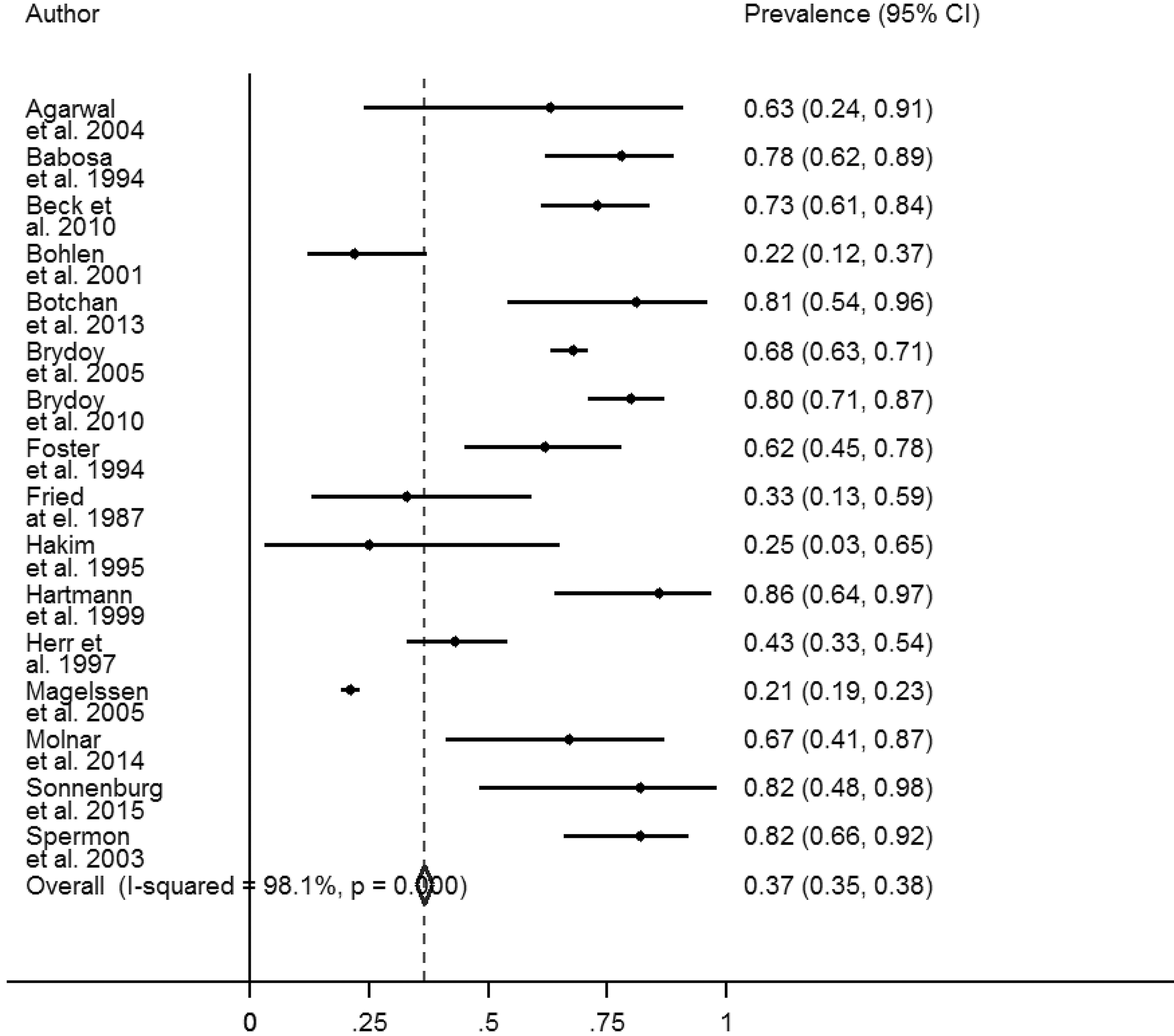
Fatherhood following treatment for TC (n = 993).
There were no data reported on preterm births (<37 weeks), still births, or perinatal deaths included in any of the studies, hence only pregnancy, terminations, miscarriages, and live birth data have been reported.
Treatment with an orchiectomy alone
There were eight studies that reported on fatherhood following treatment with an orchiectomy alone (Table 2). There were 684 (20%) (95% CI: 0.19–0.21; I2 = 98.7%)13,30,32,41,47,57,58,61 males who received this treatment who successfully conceived with their partner. Of those males that experienced a pregnancy with their partner, 753 (32%) (95% CI: 0.31–0.34; I2 = 99.1%)13,30,32,33,55,58 had a live birth. The median age at cancer diagnosis and at birth was 30.3 and 35 years, respectively, for these collective studies.
Treatment with an orchiectomy followed by chemotherapy
There were 1058 (22%) (95% CI: 0.21–0.23; I2 = 98.9%)13,30,32,38,39,41,47,58,61 males that received combined treatment with an orchiectomy followed by chemotherapy that experienced a pregnancy with their partner. Of those couples that successfully conceived, 34% (n = 816) (95% CI: 0.33–0.36; I2 = 98.8%)13,30,32,33,39,50,58,59,63 resulted in a live birth (median age at cancer diagnosis and at pregnancy or birth were 28.7 and 30.3 years, respectively).
Treatment with an orchiectomy followed by radiotherapy
For those males who had received multimodality treatment with an orchiectomy followed by radiotherapy, similarly low pregnancy rates of around 20% (n = 952) (95% CI: 0.19–0.22; I2 = 98.7%)13,30,32,38,41,47,58,61 were experienced by couples with 32% (n = 731) (95% CI: 0.31–0.34; I2 = 98.9%)13,30,32,33,53,58,59 experiencing a live birth. Median age at diagnosis and at pregnancy or birth was 29.7 and 32 years, respectively.
Treatment with an orchiectomy followed by RPLND
Additionally, males who received combination treatment with an orchiectomy followed by a RPLND, were 21% (n = 841) (95% CI: 0.19–0.22; I2 = 98.3%)13,30,32,38,47,52,54,56,58,60–62 likely to achieve pregnancy with their partner and 34% (n = 837) (95% CI: 0.32–0.36; I2 = 98.6%)13,30,32,49,52,54,–56,58,59 of couples experienced parenthood subsequent to treatment. Median age at diagnosis and at pregnancy or birth was 31.9 and 34.5 years, respectively.
Discussion
This systematic review and meta-analysis provide evidence that low pregnancy and live birth rates for couples are associated with treatment for TC. 32 Additionally, some male cancer patients may still desire fatherhood, but may not be ready to start a family at the time of treatment or alternatively may have already completed having a family. As TC is considered the most common cancer affecting males of reproductive age and with increasing curative rates and survival for TC, patients need to be given an opportunity to consider their fertility in relation to their diagnosis and treatment.
Current clinical guidelines65–70 recommend that newly diagnosed male cancer patients be referred for counseling and discussions regarding infertility as part of comprehensive cancer care in relation to their diagnosis and treatment, including those who may have already fathered children. Hence, the importance of having discussions and counseling around sperm banking before the start of treatment. 63 Several studies have also indicated elevated fertility-related psychological distress in cancer survivors when their fertility is impacted following treatment, 71 hence the importance of timely referrals for fertility discussions.
Approximately 14%13,30,32,33,35,38,39,54,57–59,61,63 of male patients in this study underwent sperm banking and these rates are in line with other studies reporting similarly low rates for sperm banking of cancer patients between 10% and 20%.58,63 Barriers associated with poor uptake for sperm banking may include lack of referral to a reproductive specialist, poor specialist knowledge regarding effects of TC treatment on fertility, cost of sperm banking, and patient/clinician wanting to start treatment urgently. Data presented in this article should therefore be interpreted with caution as not all patients may have desired fatherhood for many personal reasons or may have unsuccessfully attempted to conceive with their partner and these data may not have been captured. Additionally, we did not have data on the number of males who were not offered sperm banking or those who were referred for fertility preservation and decided not to cryopreserve their sperm.
Meta-analyses were performed using pooled data from the combined studies. Finding of this meta-analysis indicated an overall conception rate of 22% (n = 1192) for couples who conceived after TC,13,30,32,35,38,39,41,43,47,51,52,54,56–62,64 although more than half of all couples (52.29%) attempted parenthood following treatment.13,30,32,39,47,55,58,59,61–63 Use of ART for conception was reported in 31.8% couples (with either intracytoplasmic sperm injection-in vitro fertilization [ICSI-IVF] or intrauterine insemination [IUI]).13,30,32,33,35,38,39,49,51,54,56–64
The opportunity for achieving fatherhood has significantly improved over the last 5 years with advancements in fertility preservation techniques and increased awareness of both semen and testicular sperm extraction for cryopreservation. These techniques in combination with ART of IVF or ICSI33,72,73 have helped to improve fertility outcomes for couples.
However, it should be noted that cancer patients may present with infertility concerns unrelated to their cancer diagnosis (such as low sperm production, abnormal sperm function, impotence, diabetes, erection and ejaculation difficulties and blockages that prevent the delivery of sperm, and injuries) before starting treatment. These men are at greatest risk for infertility.
In addition, we performed subanalysis to explore reproductive rates for fatherhood in relation to different TC treatment modalities. It was interesting to observe that most couples had <25% (19–23%) chance of siring a pregnancy with their partner following TC treatment with an orchiectomy alone and/or with chemotherapy, radiotherapy, or a RPLND. The literature reports that infertility has been estimated to occur in about 25% of TC survivors within the first 2–5 years post-treatment.74,75 It has also been reported that reproductive cancer treatments often result in significant fertility reductions, most noticeable in the first few years following treatment.
However, as insufficient information was reported on chemotherapeutic agents as well as dose and site for administration of radiotherapy, in the included studies, we were unable to present fertility outcomes in relation to specific treatment regimens.
It has been well reported in the literature that chemotherapy regimens and radiotherapy can have deleterious effects on male fertility and endocrine function, particularly on spermatogenesis.76,77 The effects of TC treatment on sperm DNA and chromatin during the recovery process is important as damage to the paternal genome can have devastating effects on the offspring. 76 There are debatable outcomes reported in the literature associated with alterations in sperm DNA. With one study highlighting an increase in DNA damage 6–24 months subsequent to treatment, 78 conversely another study reported no increase in DNA damage. 79
A study by Bujan et al. 76 reported adverse gonadotoxic effects, particularly with the use of chemotherapy and radiotherapy, on spermatogenesis of TC patients, with potential recovery at 2 years post-treatment. The study reported elevated effects of radiotherapy on chromatin changes at 6 months after cancer treatment with an increase in aneuploidy during the 17 months following the use of chemotherapeutic agents, such as bleomycin, etoposide, and cisplatin (BEP), which are used to treat cancer patients. 80 These outcomes have been confirmed in results, highlighted in other studies, following the first 2 years post-treatment.81–85
Ghezzi et al. 77 assessed the impact of having an orchiectomy followed by chemotherapy (BEP treatment, or surveillance alone) on sperm parameters, sperm aneuploidies and DNA fragmentation, sex hormones, and testicular volume in TGCT cancer patients. Patients (n = 212) were followed at various time points (baseline 12- and 24-months post-treatment) to determine the effects of carboplatin (CARB) compared with surveillance and BEP treatments. Findings indicated an increase of sperm aneuploidies after BEP therapy up until 24 months post-treatment and adverse effects on sperm DNA, which continued up until 24 months from end of treatment. The authors also highlighted that one cycle of CARB did not have an effect on sperm aneuploidies, DNA compaction, and DNA fragmentation.
Overall, the estimated medical termination rate was 10%.48,52,58,59,61 Couples may decide to terminate a pregnancy following cancer treatment as they may experience heightened psychological concerns and fears associated with their diagnosis. Additionally, spermatozoa may carry damaged DNA after completion of treatment, hence the concern that cancer survivors may transmit a defective genome to their offspring. 84 Furthermore, cancer patients may also fear disease relapse and how this may affect their ability to parent. 86
Furthermore, we conducted a subanalysis on fatherhood (live birth rates). Less than half of all couples who became pregnant after TC treatment experienced a live birth (37%) (95% CI: 0.35–0.39; I2 = 97.8%).13,30,32,33,35,39,48–56,58,59,63,64 Unfortunately, as only five studies48,52,58,59,61 reported data on medical terminations, we were unable to determine the actual proportion of live births that may have been experienced.
The literature reports that infertility affects ∼20–30% of males and 15% of couples globally. 87 Rates for fatherhood reported in this study are considerably lower compared with males from the general population. Fossa and Kravdal 88 report that males treated for TC experience lower fertility rates of around 30% compared with those males in the general population.
Tang et al. 89 report that male cancer survivors were 23% (standard birth ratios: 0.77, 95% CI: 0.75–0.79) less likely to father an offspring compared with males without cancer in the general population. 89 Furthermore, these authors report that males diagnosed with a childhood cancer (0–12 years) are 38% less likely to give birth (standardized birth ratios [SBRs] 0.62, 95% CI: 0.57–0.67) compared with males diagnosed with cancer in adolescence or adulthood. They also highlight that males diagnosed with cancer in adulthood are 20% less likely to experience parenthood (SBR 0.80, 95% CI: 0.78–0.82) compared with the general population of males without cancer.
Additionally, Syse et al. 90 report similar findings, where male cancer survivors had a 24% (odds ratio 0.76, 95% CI: 0.72–0.79) lower first birth experience compared with the general population when matched by age and education. Similar findings were presented by Green et al. 91 who stated that male survivors were 44% (hazard ratio 0.56, 95% CI: 0.49–0.63) less likely to conceive with their partner compared with siblings who had not undergone cancer treatment.
Limitations
There are several limitations that need to be addressed in presenting reproductive outcomes, in relation to fatherhood, from the combined studies. Data were unavailable in some of the studies in relation to cancer stage, baseline semen analysis (number of sperm, motility, morphology, volume of the ejaculated sample), number of patients that relapsed following initial treatment for TC and only few studies provided time to pregnancy or birth following TC treatment. Also rates for partner infertility were not included in the studies. Additionally, as control groups were not included in each of the studies, we were unable to conduct odds or risk ratios for aged-matched groups (cancer vs. control) in relation to reproductive outcomes for each study. Despite these limitations associated with this study, we still report several interesting findings.
Conclusions
This systematic review and meta-analysis report low pregnancy and birth rates for male TC survivors who desire fatherhood as compared with those males in the general population. We present findings in support of international guidelines that recommend patients be referred for discussions around treatment-related fertility impairment before starting cancer treatment 33 as well as oncofertility psychosocial support.
Footnotes
Author Contributions
B.G. and A.A. were responsible for the conception and design of this study. B.G., A.K., M.B., and X.V. were responsible for screening included studies. B.G., O.A., and H.W. were responsible for the analysis of data. All authors read and approved the final article.
Availability of Data and Materials
All data pertaining to this study are contained and presented in this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.