
Abstract
Purpose:
Adult survivors of childhood cancer (ASCCs) are at high risk for cardiovascular disease from chemotherapy- and radiation therapy-related cardiotoxicity. Physical activity (PA) can reduce this risk, but the majority of ASCCs do not engage in sufficient PA. The purpose of this study was to identify barriers, facilitators, and resources for PA among ASCCs using the ecological model of physical activity (EMPA) as a theoretical framework.
Methods:
A concept elicitation survey was distributed independently to ASCCs (diagnosed with cancer before the age of 18, and currently 18–39 years old) and parents/legal guardians of an ASCC. The survey consisted of open-ended questions asking about barriers, facilitators, and resources for PA. Content analysis of open-ended questions categorized responses into levels of the EMPA and identified key themes.
Results:
Seventeen ASCCs and eight parents of ASCCs completed the survey. The majority of barriers, facilitators, and resources reported were at the individual and microsystem level of the EMPA. Six themes emerged, suggesting that ASCC's PA was related to proximity/access, social support, equipment, time/schedule, finances, and health-related barriers.
Conclusion:
This is the first study to examine barriers, facilitators, and resources of PA among ASCCs using the EMPA. Findings from this study provide a multilevel perspective on the influences of PA among ASCCs, and can be used for future, in-depth qualitative studies and quantitative survey development, and as a foundational step toward supportive efforts in increasing PA among ASCCs.
Introduction
In 2020
Physical activity (PA) is a lifestyle factor that may prevent or attenuate many of the long-term health problems that ASCCs experience, including cardiovascular disease. 12 Based on this evidence, the American Cancer Society recommends ASCCs engage in regular PA, including 150 minutes per week of moderate PA, 75 minutes per week of vigorous PA, or some combination thereof. 13 However, ASCCs are less likely to meet recommended PA guidelines compared to their healthy siblings, 14 and the general population.15–17 Previous studies have suggested that in addition to common barriers experienced by the general population, 18 ASCCs face additional barriers to PA related to physical limitations incurred by cancer-related surgery, or treatment-related cardiotoxicity.16,19 Thus, to increase PA among ASCCs, a more specific and comprehensive understanding of barriers and facilitators to PA are needed.
A social ecological framework, designed to evaluate individual, sociocultural, and environmental determinants of PA, is well aligned to identify barriers and facilitators for PA. Spence and Lee developed the ecological model of physical activity (EMPA) as a comprehensive model for understanding PA. 20 The EMPA posits that in addition to addressing individual factors (e.g., medical and demographic characteristics, self-efficacy, beliefs, and attitudes), it is necessary to consider factors encompassed by the microsystem, mesosystem, exosystem, and macrosystem. 20
The microsystem consists of the immediate environment surrounding and the individual (e.g., locations in which someone lives, plays, works, and spends time). The mesosystem includes linkages and connections among microenvironments (e.g., transportation between home and recreation center). The exosystem refers to a pathway by which PA can be influenced by a microenvironment that does not include the individual (e.g., information delivered to a parent in their work setting, impacting child's PA). The macrosystem is the physical and social environments that encompass the microlevel, mesolevel, and exolevel environments (e.g., policy and socioeconomic status). It has been suggested that each level of the EMPA interacts dynamically to influence PA for the individual. 20
In 2013 review, Gillam and Schwebel utilized an ecological framework to explain child and adolescent survivors' PA. Findings concurred with the conceptual model, suggesting that multiple factors work together to encourage or discourage PA among survivors of child/adolescent cancer. 21 However, it is unclear whether the PA correlates identified in this study would remain consistent as child and adolescent survivors transition into adulthood. Thus, the aim of this study was to conduct an exploratory study to identify barriers, facilitators, and resources for PA among ASCCs, utilizing the EMPA framework.
Methods
A qualitative concept elicitation survey was developed and administered to ASCCs, and parents of ASCCs to gather information about barriers and facilitators of PA. Following approval from Colorado State University's institutional review board for the protection of human subjects (IRB no. 18-8349H), the survey was distributed by Qualtrics, a secure, web-based survey platform (Qualtrics, Provo, UT). Upon clicking the survey link, potential participants were taken to an informed consent page. After consenting, participants gained access to the survey. Results were aggregated and summarized for analysis.
Participants
ASCCs and parents/legal guardians of an ASCC were eligible for the study. ASCCs were defined as individuals being (1) diagnosed with cancer before 18 years of age and (2) currently 18–39 years old (based on National Institutes of Health [NIH] guidelines for pediatric oncology treatment regimens). 22 Additional eligibility criteria included the following: able to read and write in English, completed active cancer therapy (e.g., chemotherapy and radiation) before the completion of the survey, and did not have an impairment that would hinder ambulation (e.g., wheelchair or crutches). Parents/legal guardians could participate, independent of whether or not their child participated (i.e., not a parent/child dyad), as long as their child met the inclusion criteria. Parents of ASCCs answered questions about their child and their own PA.
Recruitment took place from January to March of 2019. Participants were recruited by purposive sampling, 23 through flyers posted in local clinics and email distribution to adult volunteers of local summer camps for children experiencing cancer, and on social media platforms that target ASCCs (e.g., www.stupidcancer.org).
Survey
Survey questions were developed with input from cancer researchers and practitioners. Before distribution, the survey was pilot tested with one ASCC and one parent of an ASCC. The survey collected demographic information, including age, gender, zip code, and cancer diagnosis information, as well as self-reported PA using the Godin Leisure-Time exercise questionnaire. 24 Participants were classified as “active” if their leisure score index (LSI) score was ≥14 or “insufficiently active” if their LSI was <14. 25
Barriers, facilitators, and resources for PA, respectively, were explored using the following three questions: (1) “Over the last year or so, what factors have made it hard for you/your child to be physically active on a regular basis?” (2) “Over the last year or so, what factors have made it easy for you/your child to be physically active on a regular basis?” (3) “Which resources would you/your child need to participate in PA on a regular basis? (Resources include things like type of activities available, people in your life, access to places to be active, financial resources, etc.)”
Data analysis
Descriptive statistics were calculated for demographic characteristics and self-reported PA. Means, standard deviations (SDs), ranges, and frequencies (n, %) were computed as appropriate, using SPSS statistical software (IBM SPSS, version 25).
Qualitative data were analyzed using content analysis of open-ended responses to the above three questions. To ensure reliability, two researchers (K.F.D. and C.A.C.) independently organized responses to align with each level of the EMPA (individual, microsystem, mesosystem, exosystem, and macrosystem).26,27 This was an iterative process as the coders identified, grouped into themes, and conceptualized patterns salient to the participants within and across the dataset.28,29 For items on which there was disagreement, coders met to discuss final disposition of coding by item and included an additional author (H.J.L.) if agreement could not be reached. 29 All coding decisions were recorded in analytic memos. 29 Responses were coded until data saturation, defined as redundancy of additional data, was reached. Saturation occurred after 17 ASCCs and 8 parents of an ASCC survey were analyzed. 30
Frequencies were computed and tabulated yielding a total number of responses for each level of the EMPA to identify the most commonly reported barriers and facilitators of PA for ASCCs. 31 Responses were first categorized under the appropriate level of the EMPA. Next, responses were grouped into categories, creating themes based on the number of responses in each category. A natural break in the categories then emerged, with six themes each having ≥10 responses, and subsequent categories having ≤4 responses (i.e., there were no responses mentioned between 5 and 9 times).
Results
Participant characteristics are presented in Table 1. A total of 17 ASCCs (n = 13 women) and 8 parents of an ASCC (n = 7 women) completed the survey. All ASCCs received chemotherapy, and a majority (59%) received >1 therapy modality. ASCCs' age at the time of survey completion was 19–39 years (mean = 26.59, SD = 6.60), and their age of diagnosis ranged from 10 months to 17 years (mean = 8.49, SD = 4.94). The average time since therapy completion ranged from 1 to 33 years (mean = 14.35, SD = 9.18). PA levels among ASCCs were approximately evenly split between active (n = 8, 47%) and insufficiently active (n = 7, 53%). Most parents of ASCCs (n = 7, 88%) were physically active.
Participant Characteristics
None of the relapses was due to metastasis.
Total over 100% because n = 14 received >1 therapy.
ASCCs and parents provided responses regarding their own PA.
ASCC, adult survivor of childhood cancer; CNS, central nervous system; n/a, not applicable; PA, physical activity; SD, standard deviation.
Barriers, facilitators, and resources for PA
Barriers to PA are reported in Table 2. Twenty-five barriers to PA were reported by ASCCs and 13 barriers to PA (for their child) were reported by parents. For ASCCs, most barriers (n = 17, 68%) were categorized as individual-level factors, and were most commonly health related (n = 9). Other barriers (n = 7, 28%) were categorized as microsystem factors, and were most commonly school or work (n = 4). There were no barriers categorized as mesosystem or exosystem factors, and only n = 1 (4%) categorized as a macrosystem factor, which was finances. For parents, the most commonly cited barriers to PA among their ASCC child (n = 5, 39%) were categorized as individual-level factors, and were most commonly time/schedule (n = 3).
Barriers to Physical Activity a
These are examples of responses to the question “Over the last year or so, what factors have made it hard for you/your child to be physically active on a regular basis?”
EMPA, ecologic model of physical activity.
Facilitators to PA are reported in Table 3. Nineteen facilitators to PA were reported by ASCCs and 12 facilitators to PA (for their child) were reported by parents. For ASCCs, most facilitators (n = 10, 53%) were categorized as microsystem factors, which were most commonly social support (n = 6) and proximity/access (n = 3). Other facilitators were categorized as individual (n = 3, 16%) and exosystem (n = 1, 5%). In addition, several responses (n = 5, 26%) were. “none” or “nothing,” which could not be categorized into a level of the EMPA. For parents (for their child), most facilitators (n = 9, 75%) were categorized as microsystem factors, and included social support as the most common response (n = 3).
Facilitators for Physical Activity a
These are examples of responses to the question “Over the last year or so, what factors have made it easy for you/your child to be physically active on a regular basis?”
Resources for PA are reported in Table 4. Twenty-five resources for PA were reported by ASCCs and 24 resources for PA (for their child) were reported by parents. For ASCCs, most resources (n = 16, 64%) were categorized as microsystem factors, and included proximity/access (n = 6) and equipment (n = 4) as the two most common responses. For parents (for their child), most resources (n = 15, 63%) were categorized as microsystem factors, and included equipment (n = 7) and proximity/access (n = 5) as the most common responses. Examples of barriers, facilitators and resources for PA, according to level of the EMPA are shown in Figure 1. ASCC-reported barriers, facilitators and resources are summarized in Figure 2, and parent-reported barriers, facilitators and resources for PA are summarized in Figure 3.
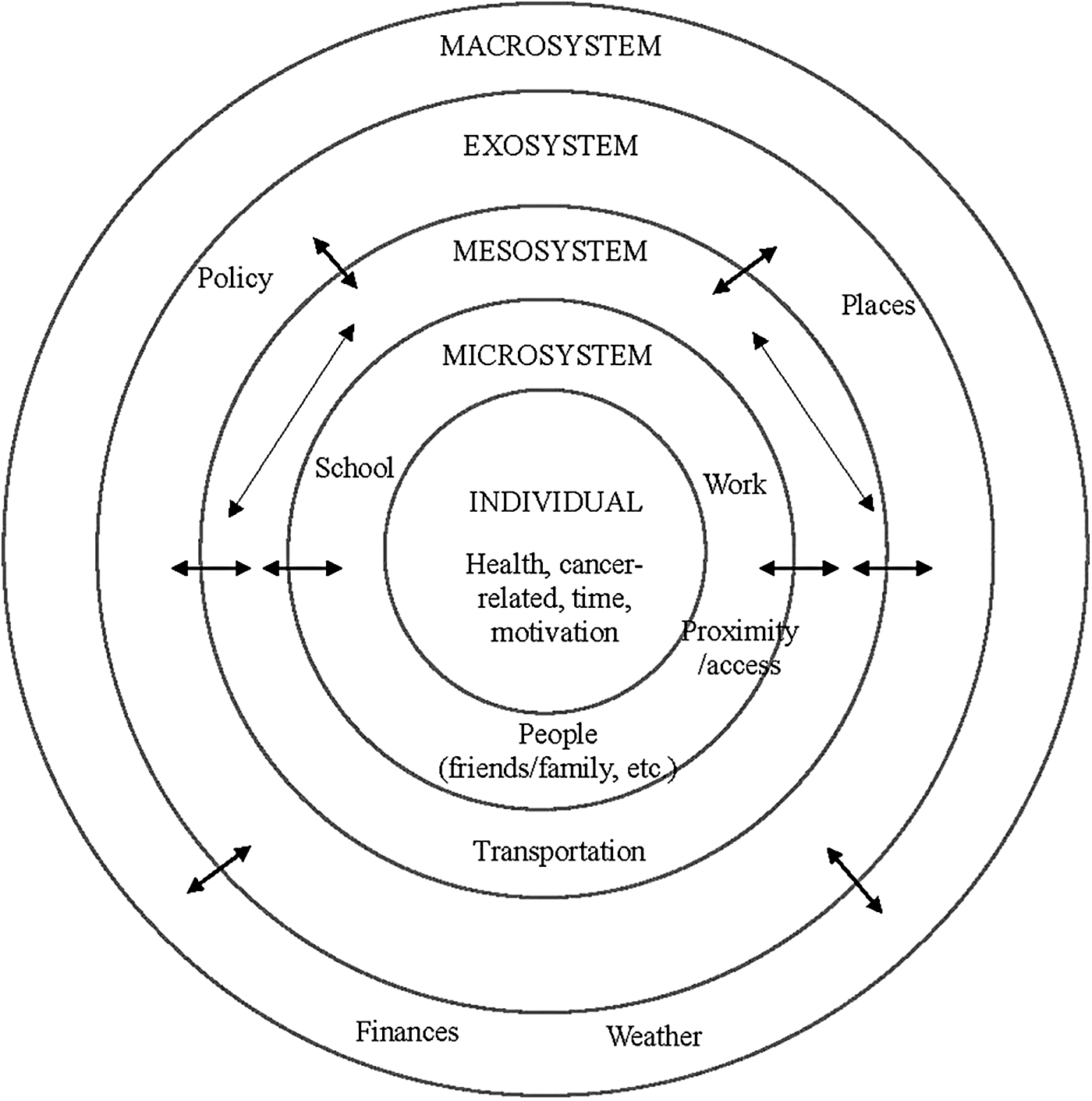
Examples of barriers, facilitators, and resources for PA reported by ASCCs and parents of ASCC, conceptualized in the EMPA. ASCC, adult survivor of childhood cancer; EMPA, ecological model of physical activity; PA, physical activity.
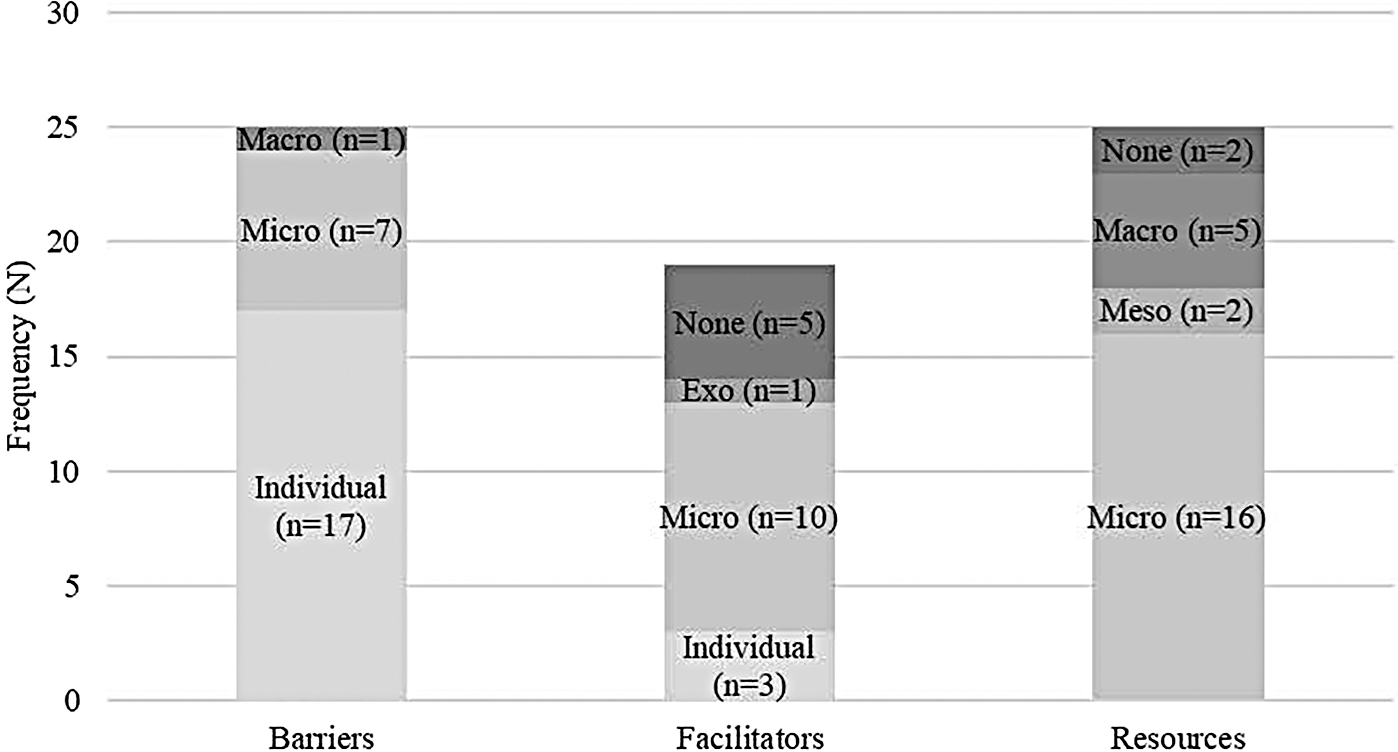
ASCC-reported barriers, facilitators, and resources for PA. aThe different colors in the bars represent levels of the EMPA. b“none” refers to responses of “none, nothing, or n/a,” which could not be categorized into a level of the EMPA.
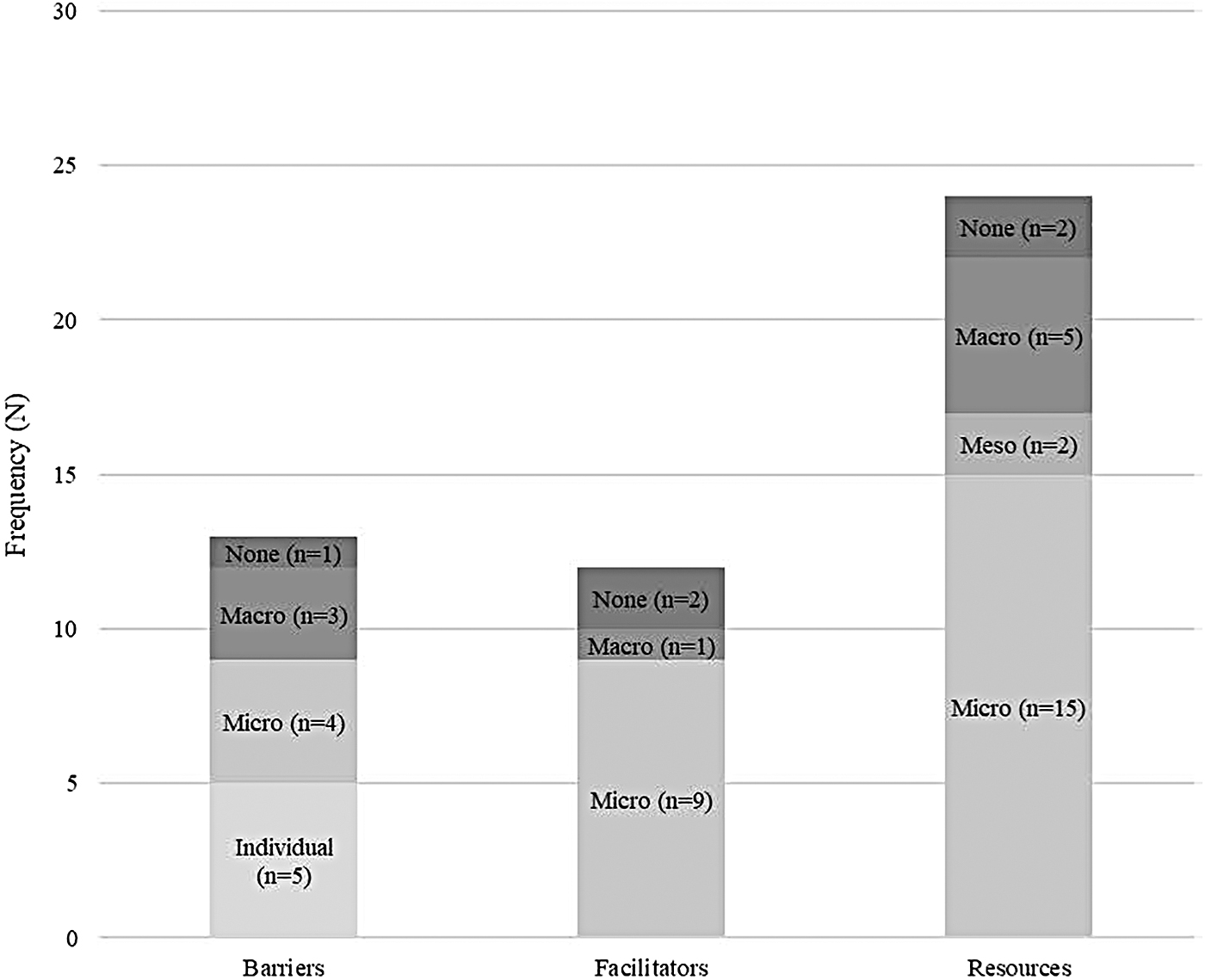
Parent-reported barriers, facilitators, and resources for PA. aThe different colors in the bars represent levels of the EMPA. b“none” refers to responses of “none, nothing, or n/a,” which could not be categorized into a level of the EMPA.
Resources for Physical Activity a
These are examples of responses to the question “Which resources would you/your child need to participate in PA on a regular basis? (resources include things like type of activities available, people in your life, access to places to be active, financial resources, etc.)?”
Themes
Six themes emerged from survey responses from both ASCCs and parents. Of these, three themes were considered microsystem-level factors, two were individual level, and one was in the macrosystem level of the EMPA.
Theme 1: proximity/access
Proximity/access to PA resources, a microsystem factor, was identified as the most common theme. Responses related to proximity/access were reported 20 times as a barrier (n = 3), facilitator (n = 6), and resource (n = 11) for PA. Examples of proximity/access as a barrier to PA were, “physical proximity to area of exercise” (ASCC) and “limited ice time at the hockey arena [sic]” (ASCC). Examples of proximity/access as facilitators to PA were: “proximity to classes” (ASCC), “proximity to parks, gyms, and so on,” (ASCC), and “quick access to trails” (parent). Examples of proximity/access as a resource for PA were: “accessible activities” (ASCC), “hiking trails” (parent), and “location relatively close to where I live” (ASCC). Responses in this theme were evenly reported among survivors (n = 10) and parents (n = 10).
Theme 2: social support
Social support, a microsystem factor, was the second most common theme, reported 18 times as a facilitator (n = 9) and resource (n = 9) for PA. Social support was not reported as a barrier to PA by any participant. Examples of social support as a facilitator for PA included “my supportive family” (ASCC) and “mom or dad taking her places” (parent). Examples of social support as a resource for PA were, “a trainer understanding my current health state” (ASCC) and “people to help with adaptive equipment” (parent).
Theme 3: equipment
Equipment, a microsystem factor, was the third most common theme, reported 15 times as a facilitator (n = 4) and resource (n = 11) for PA, but not as a barrier for PA. Examples of equipment as a facilitator for PA were, “adaptive equipment” (ASCC) and “having the gear to participate in the activities he wants to be involved in” (parent). Examples of equipment as a resource for PA were, “I find it easier to work out when I'm in a class or have a video one to follow along with” (ASCC) and “backpacking gear” (parent).
Theme 4: time/schedule
Finding time, or a busy schedule, an individual factor, was reported 14 times as a barrier (n = 12) or facilitator (n = 2) for PA. Examples of time/schedule as barriers to PA were, “I started graduate school” (ASCC) and “busy schedules” (parent). One example of time/schedule as a facilitator for PA was, “I have more time in my schedule without worrying about homework deadlines” (ASCC). In some cases, time/schedule was categorized as a microsystem-level determinant such as “being preoccupied with work” (ASCC) and in others, “my class schedule is super busy” (ASCC) was categorized as an individual-level factor for PA.
Theme 5: finances
Finances, considered a macrosystem factor, was the fifth most common theme, reported 12 times as a barrier (n = 3) and resource (n = 9) for PA. Examples of finances as a barrier to PA were: “financial hardships” (parent) and “limited financial resources” (parent). Examples of finances as a resource for PA were, “finances to afford gym costs” (ASCC) and “money” (parent).
Theme 6: health-related barriers
Health-related barriers to PA, considered an individual factor, was the sixth and final theme (n = 11, all in response to the barriers question). Examples of health-related barriers were, “an exercise-related breathing issue” (ASCC), “fatigue and pain” (ASCC), “sickness and surgeries” (ASCC), and “he is blind” (parent).
Discussion
Using a concept elicitation survey, this study examined barriers, facilitators, and resources for PA reported by ASCCs, and parents of an ASCC. Through content analysis of open-ended questions, responses were categorized into levels of the EMPA and key themes were identified.
The majority of facilitators, barriers, and resources for PA were microsystem factors, further emphasizing the importance of factors that exist in the immediate setting where individuals live, work, and play.20,21,32 For example, proximity/access was the most prominent theme that emerged from survey responses, for both barriers and facilitators to PA. Research with healthy adults indicates that access to resources significantly predicts PA, such that those enrolled in community programs, or who have access to PA facilities show higher PA levels.33–35 These findings suggest that similarly, access may be an important determinant of PA for ASCCs.
Social support, another microsystem factor, emerged as a common theme with regard to facilitating PA, whereas lack of social support was not mentioned as a barrier for PA. This finding is consistent with previous literature that suggests social support is necessary for long-term PA in adult cancer survivors, 36 as well as children, adolescents, and healthy adults.37–41 The qualitative data collected in this study adds to the literature by specifying who in particular (e.g., family and/or friends) are important sources of social support for PA among ASCCs.
Individual factors also emerged as important barriers, facilitators, and resources for PA among ASCCs. Time/schedule limitations were a notable individual barrier for PA, consistent with literature in childhood cancer, other cancer populations, and healthy populations.42–44 Participants also reported health-related barriers to PA, such as fatigue and pain, which are consistent with previous literature among ASCCs. 14 Of the health-related barriers mentioned by survivors, n = 9, 100% were cancer related.
ASCCs and parents of an ASCC reported “finances” as a barrier to PA. Previous literature in adults 45 and adolescents 46 suggests economic or financial limitations may impact PA. To our knowledge, this is the first study to identify finances as an important barrier to PA for ASCCs. Many of the responses related to finances were vague (e.g., “money”), making it difficult to disentangle whether finances were a barrier to PA due to lack of awareness of free resources (e.g., walking outside), or if ASCCs assume that PA requires high-cost memberships and/or equipment.
Finally, several responses to the question, “What factors have made it easy for you/your child to be physically active on a regular basis” were “none, nothing, or n/a.” ASCCs and parents of ASCCs reported “none, nothing, or n/a” a total of 12 times, as a barrier (n = 1), facilitator (n = 7), and resource (n = 4) for PA. ASCCs may be unaware or unsure of what is helping them engage in PA, or it is also possible that since many participants were already physically active, nothing could “make it easier.” Furthermore, parents may have been unsure of how to respond to this question for their adult child. Without further exploration of these responses, it is not clear why participants reported that “nothing” could help them be more physically active.
Strengths and limitations
Strengths of this study include the application of a social ecological framework and reaching saturation in the qualitative data collection. The EMPA helped to identify several themes that may not have emerged had we utilized theoretical models primarily focused on individual determinants of PA (e.g., attitudes, perceived behavioral control, and self-efficacy). Reaching saturation ensured that we have a comprehensive depiction of barriers, facilitators, and resources for PA from the perspectives of both ASCCs and parents of an ASCC.
Given the exploratory nature of this study, several limitations should be mentioned. First, we did not collect demographic information that may have complemented the survey responses. This includes socioeconomic status and race/ethnicity of participants, which can be important for interpreting what is meant by a theme or category of barrier, facilitator, or resource for PA. For example, two responses related to barriers to PA of “limited ice time” and “no ice rink in neighborhood” may both be categorized as a lack of resources. However, with complementary information about family or neighborhood-level income, the context in which these barriers occur may be revealed, indicating there may be multiple ecological influences involved (e.g., no ice rink is the microenvironment, but the low neighborhood socioeconomic status driving the lack of facilities is the macroenvironment).
Second, all except one of the parents who responded to the survey identified as the mother or stepmother of an ASCC. Thus, it is difficult to generalize their perceptions of barriers, facilitators, or resources for PA to fathers or stepfathers of children who are ASCC.
Third, there was potential for selection bias in our sample. The purpose of the study was disclosed during recruitment, and thus, individuals who were physically active or had a fondness for the topic and/or research related to PA may have been more likely to complete this study. Without purposeful concealment or deception of the study purpose, it would be challenging to completely eliminate this bias. However, even with this potential bias, our sample of ASCCs was evenly split between “active” and “inactive,” which provides us with confidence that responses represent both active and inactive ASCCs. Furthermore, even with a sample that is not representative of the population in terms of PA levels (e.g., sample is more active), the nature of the question about facilitators for PA allowed us to gather valuable information related to “what can help ASCCs be more active?” Traditionally, in PA and other behavioral research, we are often inclined to gather information from individuals who are not performing the desired behavior, extrapolate these barriers to others, and search for solutions to overcome the identified barriers. Perhaps there is a need for a paradigm shift, in which we ask, “what can we learn from individuals who are able to successfully engage in PA,” and “how can we extrapolate or modify this information to those who are struggling?”
Fourth, although this study accomplished what it was designed to do (i.e., explore barriers and facilitators to PA among ASCCs, and parents of an ASCC), our study design did not allow for additional probing of provided responses. For example, there were several responses of “none,” “nothing,” or “n/a.” In these instances, additional follow-up questions or probing may have elucidated additional information. Thus, our findings provide important information to assist with designing future studies that utilize more in-depth qualitative methodology (e.g., semistructured interview or focus group) to expand the understanding of social-ecological determinant PA among ASCCs.
Finally, it was unknown if parents and ASCC respondents were related or matched (i.e., a dyad); thus, we were unable to determine if a survivor and their parent provided similar answers, or able to match parent responses (i.e., barriers, facilitators, and resources) to ASCC demographic, medical, or PA information.
Future directions
To build on these findings, future studies should utilize semistructured interviews and/or focus groups to increase the richness of the qualitative data through probing. Questions should ask about themes identified through this study, including cancer-related health barriers, the ASCCs' experience and the impact of childhood cancer on PA habits, and the role of finances among this population. Findings from this study may also be used in quantitative survey development to examine associations between barriers or facilitators and PA. For example, a Likert-scale question could ask, “On a scale of 1 to 7, please rank the importance of the following factors in helping you engage in PA.” Based on our findings, we suggest that cancer-related barriers and finances should be listed as some of those factors.
Conclusion
This study explored barriers, facilitators, and resources for PA among ASCCs, and utilized a social-ecological framework to categorize responses. The majority of barriers were considered microsystem factors, and included proximity/access, social support, and equipment. Financial resources were identified as an important macrosystem-level resource for PA, and cancer-related side effects such as fatigue and pain emerged as barriers to PA. ASCCs are at risk for long-term, treatment-related health consequences such as cardiovascular disease, and thus, it is critical to further our understanding of successful ways to promote PA to help childhood cancer survivors to thrive into adulthood.
Footnotes
Acknowledgment
The authors would like to thank Ashley G Clark, MPHc for her contribution to the qualitative data analysis.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Leach is supported by a career development award from the American Cancer Society (131629-MRSG-18-021-01-CPPB). There were no other funding sources to support this study.