
Abstract
Purpose:
This mixed methods study sought to assess adolescent and young adult (AYA) adherence to three cancer treatment recommendations (medications, diet, physical activity), and determine the individual, family, and health system factors associated with suboptimal adherence.
Methods:
In Stage 1, 72 AYA-caregiver dyads completed a validated adherence interview and surveys about individual and family functioning. Matched providers (n = 34 who reported on 61 AYAs) completed global adherence ratings through survey. In Stage 2, a subset (n = 31) completed qualitative interviews.
Results:
Medication adherence was higher (M = 94.8%) than diet (M = 73.9%) and physical activity (M = 55.4%), although ≥50% demonstrated “Imperfect Adherence” for each subtask. Univariately, AYAs who missed a medication had more depressive symptoms, worse health-related quality of life (HRQOL), and more medication barriers; their families had more financial stress, worse family functioning, and lower self-efficacy. The odds of adhering to medications were lower with worse HRQOL (odds ratio [OR] = 1.08; 95% confidence interval [CI], 1.02–1.15) and family functioning (OR = 0.18; 95% CI, 0.04–0.91). The odds of adhering to physical activity and diet were lower with worse family functioning (OR = 0.09; 95% CI, 0.01–0.91) and more barriers (OR = 0.24, CI: 0.10–0.61), respectively. Qualitative themes further supported multilevel influences on AYA adherence.
Conclusions:
Adherence challenges were identified across medications, diet, and physical activity. Multilevel contextual factors were associated with suboptimal adherence, including poorer HRQOL and family functioning. Findings support the need to improve clinical adherence assessment and develop contextually tailored interventions.
Introduction
While the historical cancer survival gap among adolescents and young adults (AYAs; ages 15–39) is closing, subgroups continue to demonstrate poorer outcomes.1–3 Stagnated survival and relapse rates among AYAs with particular cancers (e.g., acute lymphoblastic leukemia) and from certain sociodemographic backgrounds have been partially attributed to treatment nonadherence—a modifiable health behavior.4,5 Medication adherence rates are lower in AYAs than younger children (27%–60% across studies).5,6 When few doses of oral chemotherapy are missed (≥5%), this confers a 2.5 greater risk of relapse.7,8 To date, estimates of nonadherence have focused on medications (commonly, 6-mercaptopurine in patients with leukemia), neglecting adherence to other important aspects of care and across cancer diagnoses. 4 AYAs are prescribed multiple home treatments, involving the administration of medications with diverse dosing schedules, specific dietary recommendations (e.g., increase caloric intake), and physical activity regimens (e.g., physical/occupational therapies). Assessing diet and physical activity adherence is important because these health behaviors have been linked to chemotherapy efficacy, symptom management, health-related quality of life (HRQOL), and overall health.9,10
Risk factors for nonadherence in AYA oncology are also dramatically understudied. A few studies found an association between adherence and modifiable (physical symptoms, 11 mood,11,12 motivation,13,14 knowledge, 15 forgetting,16,17) and nonmodifiable individual-level factors (AYA age, ethnic/racial minority status).5,7 Systems-level variables that are intricately linked to adherence in other populations, such as the family environment18,19 and the financial burden of treatment (i.e., financial toxicity),20,21 have been overlooked. Family functioning is a promising target of inquiry. Our prior work demonstrated that family functioning is significantly related to treatment adherence across other pediatric populations. 22 Family-based interventions are also particularly robust for improving adherence. 23 Published studies in this population have other key limitations, including being atheoretical, having small sample sizes, and lacking multiple informants. 24 These limitations may partially explain why the only published AYA oncology adherence-promotion intervention demonstrated limited efficacy. 25
This study sought to address these gaps by adopting a broader, theory-informed conceptualization to: (1) evaluate AYA adherence, adherence barriers, and allocation of treatment responsibilities among family members across three prescribed tasks (medications, diet, physical activity), and (2) test individual, family, and health system factors of nonadherence in accordance with an evidence-based model of disease management. 26 We hypothesized that adherence challenges would span each of the three treatment tasks, and multilevel contextual factors would relate to suboptimal adherence, including AYA (depressive and anxiety symptoms, poor HRQOL and health beliefs), family (poor family functioning and self-efficacy for managing the regimen, AYA responsibility for treatments, financial stress), and health system factors (public insurance, high out-of-pocket medical expenses).
Methods
Theoretical framework
The Pediatric Self-Management Model 26 informs this study and asserts that disease self-management behaviors (e.g., taking medications) occur in context. Adherence may be influenced by nonmodifiable and modifiable individual (e.g., age, depressed mood), family (income, family functioning), and health system factors (insurance, cost).
Study population
Participants were AYAs receiving cancer treatment at a pediatric cancer center, and their matched primary caregivers and oncology providers. Inclusion criteria (AYAs): (1) Between the ages of 14–24 (guided by the National Cancer Institute, 27 but adjusted to represent the younger age of patients at our center who are beginning to assume treatment responsibilities), (2) Receiving cancer treatment (chemotherapy and/or radiation) with curative intent for leukemia/lymphoma, solid tumor, or brain tumor, (3) Diagnosed ≥1 month ago, and (4) English literacy. Inclusion criteria (caregivers): (1) AYA nominates the parent/legal guardian as a primary caregiver involved in oncology care, (2) Resides with the AYA ≥50% of the time (given a focus on family functioning), and (3) English literacy. An exclusion criterion was cognitive impairments that would limit the ability to complete measures. Inclusion criteria (providers): (1) Oncologist, fellow, or advanced practice nurse most familiar with the AYA's current cancer care.
Procedures
In Stage 1, AYA-caregiver dyads were recruited at the hospital or through phone in this Institutional Review Board-approved study and completed informed consent/assent (Fig. 1). Immediately following recruitment, we conducted a structured adherence interview jointly with the dyad (either in person in the outpatient/inpatient setting, or over the phone). Three AYAs opted to complete the interview alone, and we were unable to get in contact with the caregiver to provide their responses. AYAs and caregivers separately completed questionnaires through REDCap. 28 Following the enrollment of the dyad, matched providers were invited to participate through a standardized email. Providers consented through an electronic consent form then completed a REDCap adherence survey.
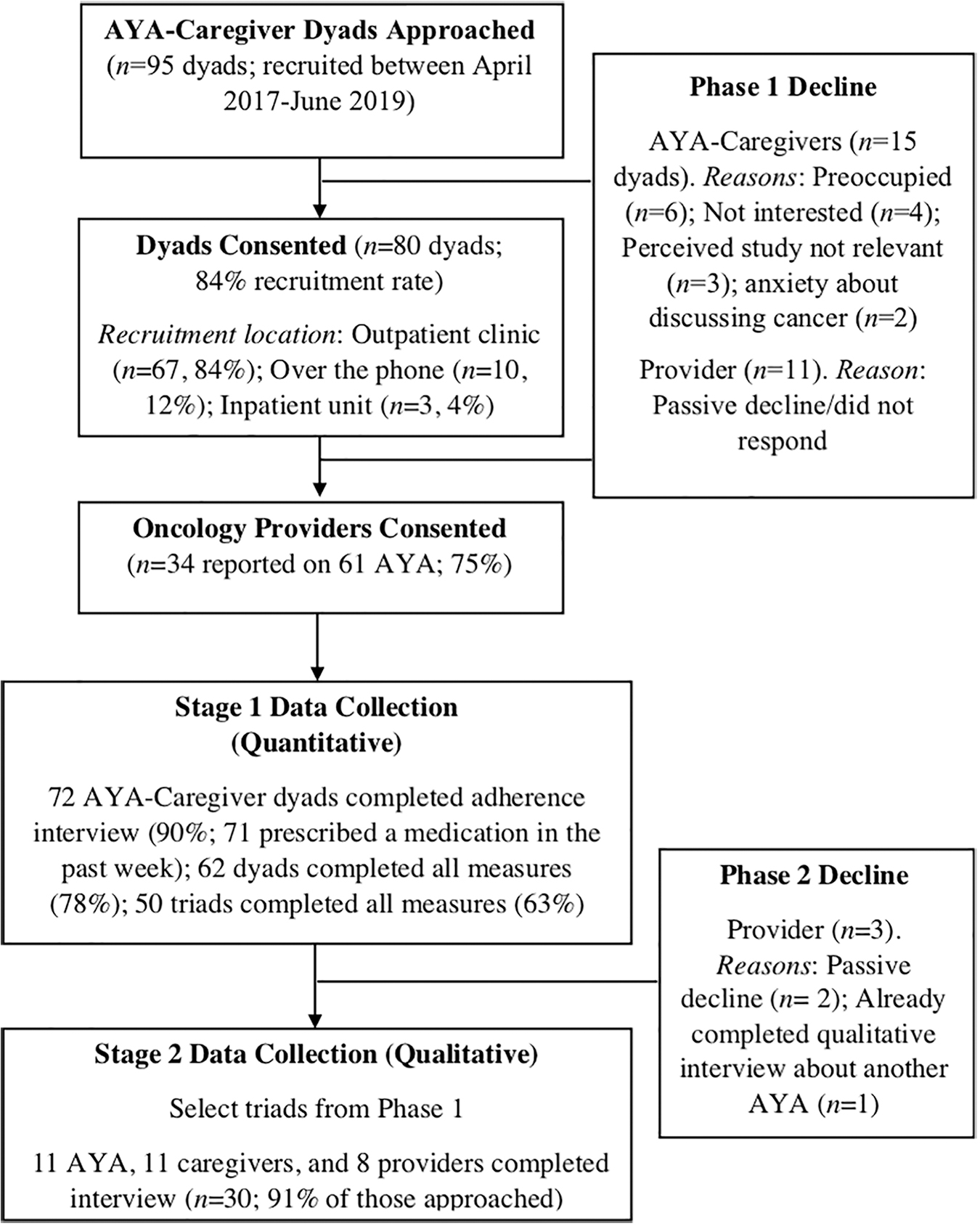
Recruitment and procedures study flow. AYA, adolescent and young adult.
In Stage 2, purposefully sampled triads from Stage 1 completed an individual, in-person interview (in a private outpatient clinic room) to further understand adherence (M = 79 days after enrollment, range 21–155 days). Purposeful, criterion-based sampling was employed to identify a maximally diverse sample in terms of demographics and cancer-specific variables (cancer type, adherence/nonadherence, AYA vs. caregiver responsibility for the regimen). 29 Participants completed qualitative interviews until we reached data redundancy (consistency in the interview information) and saturation (no new themes),30,31 resulting in 31 interviews (typical for qualitative studies). No incentives were provided for participation.
Measures
Demographic, disease, and health system factors
AYAs and caregivers provided data regarding their sex, gender, age, race, and ethnicity. Caregivers reported on annual family income, as well as financial stress through two items from the Comprehensive Score for Financial Toxicity measure 32 (“I feel financially stressed,” “My out-of-pocket medical expenses are more than expected”). Reviews of each AYA's electronic health record (EHR) were conducted to identify diagnosis (leukemia/lymphoma, solid tumor, brain tumor), days since diagnosis, relapse status (yes/no), and primary health insurance (public/private). The Intensity of Treatment Rating 3.033 was completed by a pediatric oncologist (L.S.K.) to categorize treatment intensity (least, moderate, very, or most intense).
AYA factors
We assessed AYA health beliefs through the Health Competence Belief Inventory (HCBI), a validated measure 34 with four subscales: (1) Health Perceptions (α = 0.70), (2) Satisfaction with Health Care (α = 0.57; excluded due to low alpha), (3) Cognitive Competence (α = 0.63), and (4) Autonomy (α = 0.61). AYAs completed the 8-item NIH Patient-Reported Outcomes Measurement Information System (PROMIS) Anxiety Short Form (α’s = 0.91–0.94 for pediatric and adult forms) and the 8-item PROMIS Depressive Symptoms Short Form (α’s = 0.90–0.93); total scores were converted to T-scores, which have demonstrated validity in pediatric cancer samples. 35 HRQOL was measured through the widely used Pediatric Quality of Life Inventory Cancer Module Scales 36 (total score; α’s = 0.86–0.87). Since self-reported adherence may be prone to bias,37,38 AYAs (α = 0.70) and caregivers (α = 0.61) completed the 13-item Marlowe–Crowne Social Desirability Scale—Short Form C. 39
Family factors
AYAs (α = 0.87) and caregivers (α = 0.86) separately completed the 12-item General Functioning subscale of the validated and widely used Family Assessment Device. 40 Caregivers completed The Family Management Measure Condition Management Ability Subscale (12 items), 41 assessing perceived self-efficacy for managing the regimen (α = 0.61).
Medical adherence
The Medical Adherence Measure (MAM) is a valid and reliable structured interview that has been widely used in pediatric solid organ transplant and generalized to other disease groups, and shown excellent convergent validity with health outcomes such as rejection episodes.42,43 Dyads provided information about the number of missed medication doses (for each scheduled medication), and the number of days that the AYA fulfilled diet (e.g., increase caloric intake, supplements) and physical activity recommendations (e.g., physical/occupational therapy exercises, moderate physical activity), over the past week. Dyadic disagreements were rare and resolved through discussion. EHR review was conducted before administering the MAM to determine all prescribed treatments (by reviewing medication lists, clinic notes from oncologists, nutritionists, and physical/occupational therapists). Since diet and physical activity prescriptions were not consistently documented, we also relied on reporter recall. Across each subtask, dyads also reported about perceived adherence barriers, who in the family is most responsible, and then separately responded to a global adherence rating on a 0–10 scale (an overall rating not limited to the past week). Providers completed the global 0–10 adherence rating for each of the prescribed subtasks in an online survey (Supplementary Data). If a subtask was not prescribed, adherence was not assessed. Clinic attendance was also assessed, but excluded since most AYAs had no missed visits (97.2%).
Stage 2
Semistructured interviews were conducted individually by A.M.P. with each stakeholder to compliment quantitative results. The interview guide for AYAs and caregivers included questions about perceptions of adherence demands, adherence/nonadherence to the prescribed regimen, and theory-informed adherence barriers and facilitators. Providers reported on their views of the adherence of their AYA patient and experiences with assessing and treating nonadherence. All interviews were audiorecorded, transcribed, and deidentified.
Data analytic plan
Stage 1 (quantitative)
Based on AYA-caregiver reporting, medication adherence percentages (the proportion of prescribed dosages taken in the past week, multiplied by 100) were calculated for oral chemotherapies (e.g., 6-mercaptopurine), prophylactic antibiotics (e.g., Bactrim), other supportive medications (e.g., Ondansetron), and collapsed across all medications. For diet and physical activity, adherence percentages were the proportion of days that the AYA completed the prescribed regimen in the past week, multiplied by 100. Given ceiling effects and lower n's for some medications/tasks, and consistent with prior studies that identified characteristics associated with suboptimal adherence,17,44 adherence percentages were dichotomized into “Perfect” for each of the three medical tasks (100% adherent) and “Imperfect” (<100%). Intraclass correlations compared global 0–10 adherence ratings between members of the triad. Descriptive statistics and frequencies/percentages were employed to examine adherence, adherence barriers, and allocation of treatment responsibilities.
t-Tests and χ 2 analyses were conducted to compare AYAs with “Perfect Medication Adherence” to those with “Imperfect Medication Adherence” in the past week (across all medications) across predictor variables. A binary logistic stepwise regression tested a multivariate model of significant associates. Given the threshold for significance (α = 0.05) and n = 71 for primary medication adherence analyses, we had 80% power to detect effects greater than an odds ratio of 2.19 and lower than 0.45. 45 Given lower n's, two exploratory logistic regressions tested the same multivariate model for diet and physical activity adherence.
Stage 2 (qualitative)
Directed content analysis techniques were employed to identify and organize relevant themes recurring throughout the individual interviews. 46 Three transcripts from each stakeholder were read by a team of trained coders (A.M.P., K.B.E., B.C.). Based on content analysis, 20 codes emerged and were independently assigned codes to a sample transcript. We then created coding definitions and developed a codebook, which was reviewed and agreed upon by the research team. Two independent coders coded each of the 30 transcripts. Coders compared their codes, resolved any discrepancies to reach agreement, and identified themes.
Results
Medication, diet, and physical activity adherence
Sample characteristics for the 72 AYAs who completed the MAM are presented in Table 1. AYAs were more adherent to medications (M = 94.8%) than diet (M = 73.9%) and physical activity (M = 55.4%) in the past week (Table 2). Participants were prescribed an average of four medications (range 0–11). AYAs were most adherent to oral chemotherapies, followed by prophylactic antibiotics and supportive medications. Less than 50% had “Perfect Adherence” across each of the subtasks. On the global 0–10 adherence rating scale, there was excellent agreement between AYAs and caregivers for medications (intraclass correlation coefficient [ICC] = 0.89), diet (ICC = 0.94), and physical activity (ICC = 0.97), p's < 0.001. There was fair agreement between AYA–provider (ICC = 0.44, p = 0.03), and caregiver–provider (ICC = 0.42, p = 0.02), diet adherence ratings. There was poor agreement between AYA–provider and caregiver–provider medication and physical activity ratings (ICC ranges = 0.01–0.23, p's > 0.05). Providers tended to rate AYAs as more adherent (Table 2). Dyads endorsed forgetting as the most common medication barrier; the most common for both diet and physical activity was not feeling well. Most families nominated caregivers as primarily responsible for medications (n = 52; 73.2%) and diet (n = 34; 60.7%). More AYAs were responsible for physical activity (n = 26; 63.4%).
Demographic and Disease Characteristics for Stages 1 and 2
Stage 1 n's = 72 AYAs, 69 caregivers, 34 providers completed adherence measures; Stage 2 n's = 11 AYAs, 11 caregivers, 8 providers who completed qualitative interview; 62/72 families provided data about family income.
AYA, adolescent and young adult; M, mean; SD, standard deviation.
Adherence and Adherence Barriers (Total n's = 72 Adolescent and Young Adult, 69 Caregivers, 61 Provider Reports)
n's vary across treatment tasks due to different prescriptions and between reporters due to different perceptions of what qualified as an adherence task.
Joint AYA-caregiver report for all but three AYAs who completed the interview alone.
Associates with medication adherence
AYAs who had “Imperfect Medication Adherence” in the past week had more medication barriers, more depressive symptoms, and worse HRQOL (Table 3). Their families had more financial stress, worse family functioning, and worse perceptions of their cancer management abilities. There was a trend for out-of-pocket medical expenses being higher in this group. AYA (vs. caregiver) responsibility was not associated with medication adherence. Using significant univariate associates as predictors, the binary logistic regression model was significant (χ 2 = 20.36, p = 0.002), explaining 25% of the variance, and correctly classifying 73% of participants (Table 4). As HRQOL increased by one, the odds of having “Perfect Medication Adherence” increased by 1.08. As family functioning problems increased by one, the odds of having “Perfect Medication Adherence” decreased by 0.18.
Univariate Comparisons of Perfect Versus Imperfect Medication Adherence
Income of 8 = $80,000–$99,999/year; n = 71/72 participants because one AYA was not prescribed medications that week.
p < 0.05.
p < 0.01.
HCBI, Health Competence Belief Inventory; HRQOL, health-related quality of life.
Logistic Regression for Medication Adherence Over the Past Week
R 2 = 0.25 (McFadden), χ 2 = 20.36, p = 0.002; the overall model correctly classified 73% of participants into perfect versus imperfect adherence categories.
p < 0.05.
p < 0.01.
CI, confidence interval; OR, odds ratio.
Exploratory analyses
The same predictors from the medication adherence logistic regression were tested in two additional models predicting Perfect versus Imperfect Adherence to diet and physical activity over the past week. The model was significant for diet (χ 2 = 16.78, p = 0.01; explaining 26% of the variance and classifying 83% of participants), but not physical activity (χ 2 = 10.82, p = 0.09). When individual predictors were tested, the number of diet barriers was significant, B = −1.41, Wald χ 2 (1) = 9.02, p = 0.003. As the number of barriers increased by one, the odds of having “Perfect Diet Adherence” decreased by 0.24 (95% confidence interval [CI], 0.01–0.91). For physical activity, family functioning was significant, B = −2.45, Wald χ 2 (1) = 4.17, p = 0.04. As family functioning problems increased by one, the odds of having “Perfect Physical Activity Adherence” decreased by 0.09 (95% CI, 0.10–0.61). All other predictors were nonsignificant.
Qualitative results
Stage 2 qualitative interviews supported Stage 1 quantitative findings and added new insights into how each member of the triad emphasized different adherence issues (Table 5). For example, AYAs and caregivers defined multiple adherence demands, including tasks captured by the MAM and additional tasks (e.g., monitoring for fever). Providers were most focused on oral chemotherapy adherence, and discussed adherence assessment challenges. Stakeholders described AYA physical HRQOL as an adherence barrier, however providers discussed this issue broadly, caregivers emphasized the challenges of establishing an adherence routine when symptoms fluctuate, and AYAs discussed their difficulties with swallowing/retaining medications (“Two days after chemo, I can barely drink water, so I can't even swallow pills. So, when I need them most is when I physically can't take them”). AYA psychological HRQOL was another theme, with depressive symptoms described as barrier (“There is nothing really to motivate [adherence], yeah to get rid of cancer. But it is a year away and putting your life on hold. What are you going to do to help me smile again?”).
Qualitative Themes, Definitions, and Perceptions by Informant
Informants described adherence as more manageable when family members effectively organize, communicate about, and share cancer-related responsibilities. Yet, some AYAs and caregivers described negative impacts of a high level of caregiver involvement, such as caregiver stress and disagreements related to AYA's desires for greater independence (“[My mom] reminds me to take my medicine because I forget. I'm worrying about being an average teenager. Of course, I get mad when she tells me to take it.”) Access to care was another theme, with respondents reflecting on how cost, insurance problems, and the complexity of the health system can impact adherence (“The insurance doesn't approve it. It has to come from a mail pharmacy who doesn't have it, and you have to make 12 phone calls and get a prior auth[orization], then, they're just not going to do it”).
Discussion
This study represents the first to evaluate AYA's adherence to multiple home cancer treatment recommendations (medications, diet, physical activity), and elucidate the social/ecological factors that may influence adherence to each task. Strengths of this study include adopting an evidence-based theory of disease self-management, 26 and utilizing multi-informants and mixed methods to triangulate adherence behaviors, barriers, and allocation of treatment responsibilities. While the overall medication adherence rates were high, we found that 50% or more of AYAs demonstrated imperfect adherence across each subtask. This is consistent with prior research that suggests that up to half of AYAs demonstrate suboptimal adherence.5,6 Adherence rates were lower for supportive medications (compared with oral chemotherapies and prophylactic antibiotics), and even lower for diet and physical activity. Qualitative themes were consistent with a need to assess adherence to all home treatments, even if oral chemotherapy is a priority.
Consistent with the Pediatric Self-Management Model, 26 multilevel contextual factors related to cancer treatment adherence, including characteristics of the AYA (depressive symptoms, HRQOL, the number and type of adherence barriers), family (family functioning, self-efficacy for condition management, financial stress), and health system (out-of-pocket medical expenses, access to care issues). In the logistic regression, HRQOL and family functioning problems emerged as the two strongest predictors, and assessing these factors may help identify patients at risk for suboptimal medication nonadherence. In the absence of efficacious interventions, 6 improving AYA's physical and emotional functioning, and the ways families interact and communicate about adherence demands, may represent important intervention targets. For example, interventions could include a combination of behavioral (e.g., reminders, incentives, symptom management strategies), cognitive (e.g., targeting AYA's adherence attitudes/motivation, depression), and family-based strategies (e.g., family problem solving, communication training). 47 Indeed, multicomponent interventions have demonstrated small-to-moderate effects on adherence in other pediatric populations.23,48 Providing social work support is also important for navigating access issues, and may partially explain why clinic attendance was high in this sample given every patient had a social worker.
Contrary to our study hypothesis and what has been hypothesized in the broader AYA oncology literature, 4 we did not find an association between allocation of treatment responsibilities (AYA vs. caregiver) and adherence. Our approach, using a self-reported measure to assess adherence to each subtask and the corresponding family member responsible for it, revealed that caregivers were predominantly responsible for two of the three subtasks (medications and diet). Qualitative themes highlighted that even when AYAs were responsible for executing the subtask, stakeholders valued “sharing” supervision of these responsibilities, which has been associated with more optimal adherence in other populations. 49
Findings should be interpreted in the context of study limitations. Our relatively small sample identified primarily as middle class, non-Hispanic White. While this demographic is consistent with patients at our center and nationally, patients from minority backgrounds have been shown to have suboptimal cancer treatment adherence. 7 Thus, our study findings may represent a more ideal adherence presentation, and future research should oversample individuals from lower SES and minority groups. Our reliance on self-reported adherence, rather than objective measures such as electronic pill bottles and accelerometers, was not ideal. Self-reported measures possess key advantages (low-cost, minimally burdensome, flexibility to assess heterogeneous regimens and processes, such as allocation of treatment responsibilities), but may inflate adherence due to recency and social desirability biases.37,38 We planned for these limitations by using a validated measure that assessed adherence in a short timeframe and measuring social desirability. Another limitation was questionable reliability of certain questionnaires. Finally, our sample was heterogeneous with regard to cancer type and time since diagnosis (both a study strength and limitation) and cross-sectional findings may not have fully captured adherence challenges that are specific to certain diagnoses/treatment phases.
These findings have several implications. A broader conceptualization of AYA cancer adherence is needed that considers multiple co-occurring treatment tasks that families self-manage from home. Longitudinal research with larger, diverse samples will be critical for determining how adherence to these subtasks cluster within individuals, across time and treatment stage, and impact clinical outcomes. Our dichotomous approach yielded clinically relevant information, but a more fine-grained examination of the magnitude and persistency of adherence challenges is needed. Improving clinical adherence assessment efforts, including conducting more frequent and valid assessments and screening for risk factors, such as HRQOL, is recommended. Families and providers were not always in agreement about what qualified as a diet or physical activity adherence task, highlighting the need to standardize how these recommendations are prescribed and monitored throughout treatment. 50 Mobile health may offer pragmatic methods for more frequently assessing adherence in daily life. 51 In a recent abstract, a Children's Oncology Group adherence intervention that involved education, reminders, and parent supervision improved 6-mercaptopurine adherence for subgroups. 52 It is important to consider approaches for optimizing adherence-promotion interventions for AYAs, including delivering theory-based, contextually tailored interventions, while carefully balancing needs for autonomy and supervision.
Footnotes
Acknowledgments
The authors thank the participating AYA patients and their caregivers and providers, as well as Heather Fellmeth, PhD and Yael Gross for their support with study recruitment.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by a grant from the American Cancer Society (PF-16-166-01-CPPB awarded to Alexandra Psihogios, PhD).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.