
Abstract
Background:
Evidence on self-care ability and occupational outcomes in Chinese survivors of childhood cancer is clearly lacking. This study aims to identify clinical and behavioral factors associated with poor life functioning in this population.
Methods:
This was a cross-sectional study conducted at an ambulatory clinic of a public hospital in Hong Kong. Licensed occupational therapists administered the Life Functioning Assessment Inventory on survivors diagnosed with cancer <19 years old and ≥5 years post-diagnosis. Survivors' career development self-efficacy, subjective happiness, and motivation were evaluated using structured questionnaires. Clinical information was obtained from medical records. Multivariable linear regression was used to evaluate factors associated with life functioning outcomes, adjusting for clinically relevant variables.
Results:
Eighty survivors were recruited (58.7% male; age at diagnosis: 6.7 [standard deviation (SD) = 4.8] years; age at evaluation: 24.4 [SD = 6.5] years). Compared to survivors of leukemia, survivors of brain tumor performed worse in social functioning (β = −0.79, standard error [SE] = 0.36; p = 0.034). Survivors who had been treated with cranial radiation also had lower worker life functioning than those who had not (β = −0.91, SE = 0.031; p = 0.021). Higher activity motivation was significantly associated with better leisure functioning (β = 0.086, SE = 0.03; p = 0.008), social functioning (β = 0.036, SE = 0.02; p = 0.036), and career development self-efficacy (β = 1.04, SE = 0.26; p < 0.0001).
Conclusion:
Survivors of brain tumors and survivors who were treated with radiation have poorer life functioning, particularly in social and work domains. Future work includes validating the study findings in a larger cohort of survivors in Hong Kong. Addressing modifiable behavioral factors include motivating survivors to engage in meaningful activities that contribute to self-care and participation in society, as well as providing at-risk survivors with ongoing support from community vocational services.
Introduction
Approximately 200
Despite improved treatment outcomes, survivors of childhood cancer are subject to a variety of late effects due to exposure to their cancer therapies.2–5 Treatment for childhood cancer typically involves different types and dose intensities of chemotherapy, radiation, and surgical procedures. Numerous studies have demonstrated that treatment-related late effects are highly prevalent in survivors.2–5 According to one population-based study that enrolled 1713 survivors of childhood cancer, 98.2% of survivors suffer from at least one chronic late effect at a median of 25 years from diagnosis. 5 These late effects include cardiovascular, pulmonary, hepatic, musculoskeletal, endocrine, and neurocognitive disorders, which lead to poorer health-related quality of life. 6 The collective findings of one systematic review suggested potential differences in the prevalence of certain late effects among Asian and non-Asian populations. These may reflect differences in treatment regimens, practice, genetic variations, and socioeconomic disparity. 4 Consequently, the impact of health outcomes on functioning and quality of life in Asian survivors of childhood cancer may be different from published findings in the Western population.
Current research exploring health-related quality of life in Chinese survivors of childhood cancer in Hong Kong has yielded conflicting findings. Li et al. reported that cancer and its treatments had adverse effects on the physical, psychological, and social well-being of Chinese adolescent survivors between 9 and 16 years of age. 7 Another local study found significantly poorer physical functioning in survivors than in sibling controls. No group differences were found in mental, social, and psychological well-being, however, suggesting that survivors adapt well in these aspects. 8
These local studies were deficient in that they did not evaluate the impact of cancer on survivors' life functioning outcomes. Studies conducted with Western populations have demonstrated more educational difficulties, unemployment, lower income, and lower rates of marriage and parenthood in adult survivors of childhood cancer compared with sibling controls and the general population.9–12 In contrast with health-related quality of life, life functioning is described as the perceived level of ability and capacity of an individual in engaging in meaningful activities that contribute to self-care, enjoyment, and participation in society. 13 It emphasizes the ability of survivors to carry out activities of daily living safely and autonomously at home, at work, and in a social setting. Research on self-care ability, as well as the educational and occupational outcomes of survivors in Hong Kong, is clearly lacking.
To address the abovementioned research gaps, the objectives of this study are to investigate the life functioning of childhood cancer survivors, and to identify clinical, treatment, and personal behavioral factors associated with poor life functioning in this population. Our theoretical model is adapted from the World Health Organization (WHO) (Fig. 1). The International Classification of Functioning, Disability and Health (ICF) conceptual model postulates that an individual's functioning in a specific domain is a complex relationship between health condition and contextual factors. 14 These determinants include both environmental and personal factors. Environmental factors refer to extrinsic variables such as society's attitudes, living environment, and infrastructure that can be either barriers or enablers to the individual's management of their disability. Personal factors comprise features of the individual that may play a role in disability and functioning, but are not part of a health condition or health state; they include individual psychological assets and motivations.
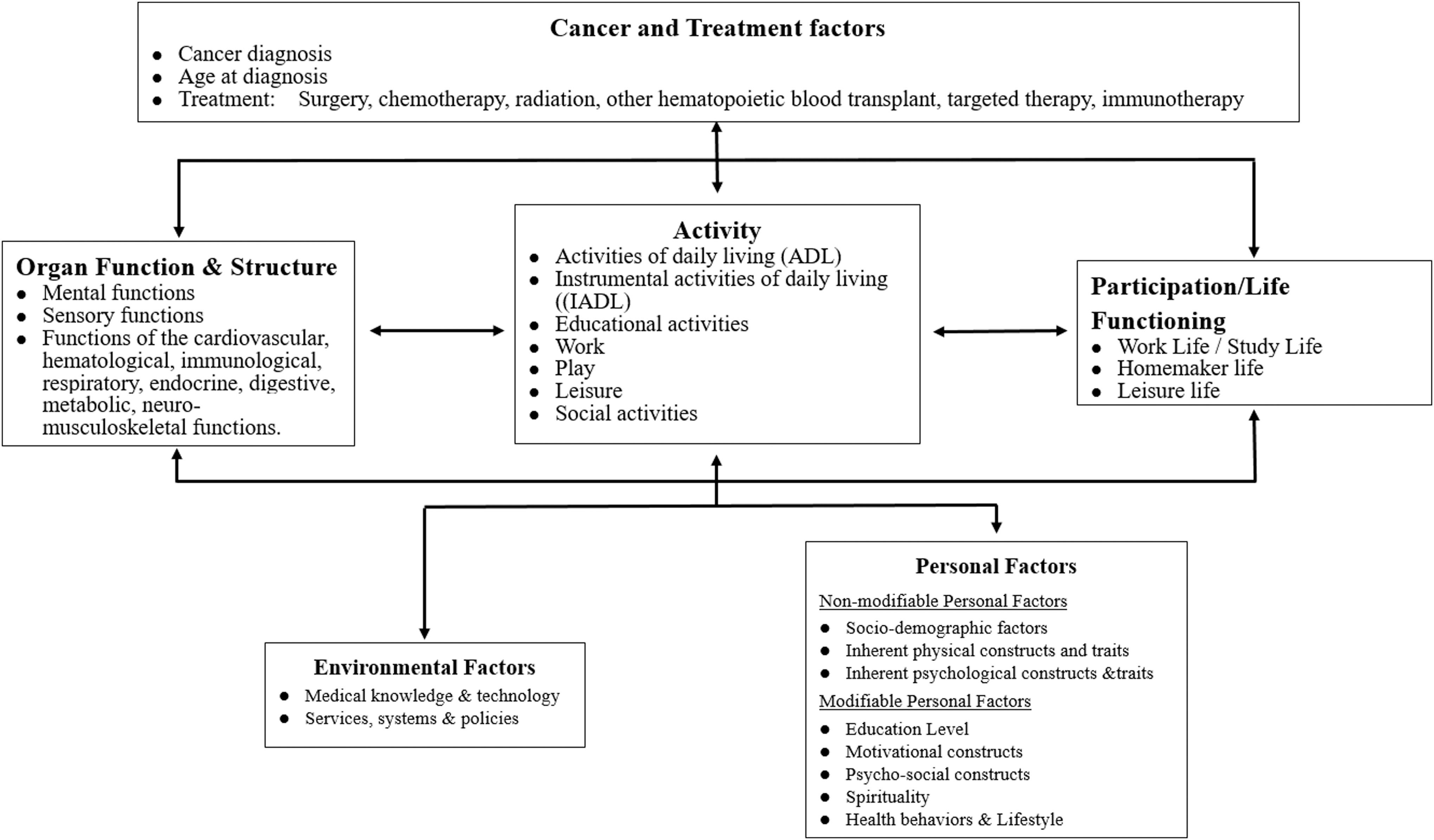
Understanding life functioning in survivors of childhood cancer by adopting WHO International Classification of Functioning, Disability and Health (ICF). According to the WHO International Classification of Functioning, Disability and Health (ICF), disability and functioning are viewed as outcomes of interactions between health conditions (late effects caused by the cancer and treatment) and contextual factors. In this study, we focus on internal personal factors, which include both clinical and demographic variables (sex, age, cancer diagnosis, etc.) and personal modifiable factors (psychological and behavioral functioning, mental health, motivation, etc.) that influence how disability and functioning are experienced by the survivor. Dysfunction involves reported impairments, activity limitations, and participation restrictions, in the domains of work, homemaker, leisure, and social functioning. WHO, World Health Organization.
We hypothesize that CNS tumors, younger age at diagnosis, and treatment with chemotherapy or radiation are clinical factors associated with poorer functioning, while better mental well-being, motivation, and subjective happiness are behavioral factors associated with higher functioning in survivors.
Methods
Study design and population
This was a cross-sectional observational study conducted at the Prince of Wales Hospital, which is one of the largest academic and public hospitals in Hong Kong. Approval was obtained from the Joint Chinese University of Hong Kong—New Territories East Cluster Clinical Research Ethics Committee. Survivors of childhood cancer were recruited from the Long-term Follow-up Ambulatory Clinic of the Department of Pediatrics from January to December 2018. Three certified occupational therapists administered a 20-minute survey and structured interview to survivors who (1) were diagnosed with childhood cancer before 19 years old, (2) had completed active treatment, which included surgery, chemotherapy, radiation, and bone marrow transplant, (3) had survived for at least 5 years after diagnosis, and (4) were Mandarin or Cantonese speaking.
Life functioning outcomes
Life functioning assessment was conducted by a licensed occupational therapist using the Life Functioning Assessment Inventory (L-FAI). 15 The scales that were utilized included four important life domains, the (1) Leisure Life Functioning Scale, (2) Social Life Functioning Scale, (3) Homemaker Life Functioning Scale, and (4) Worker Life Functioning Scale. The dimensions of each scale are presented in Supplementary Table S1. Occupational therapists underwent 6 hours of formal training before they were certified to administer the L-FAI. The L-FAI was first developed and validated within Chinese patients with mental health disorders in Hong Kong. During the development phase, the L-FAI was validated within a group of seven healthy volunteers and yielded reasonably good reliability (Cohen's kappa 0.67–0.97) and validity. 15 The score of each scale ranges from 1 to 10. Levels of functioning were defined based on the following cutoff: “very high functioning” (9–10 points), “high functioning” (7–8 points), “average” (5–6 points), “low” (3–4 points), and “very low” (1–2 points). 15
Self-efficacy in career planning was evaluated using the Career Development Self-Efficacy Inventory. 16 It contained 24 items divided into six categories, namely career planning, gender issues, training selection, job hunt preparation, job hunting, and career goal setting. Respondents rated their confidence in completing the mentioned tasks on a 6-point scale ranging from 1 (extremely not confident) to 6 (extremely confident). The total score ranges from 1 to 144. This inventory has been validated in studies collectively involving 6776 senior secondary school students in Hong Kong. All factor loadings of six categories were higher than 0.87 and the internal consistencies of the total scale showed an α coefficient of 0.95. 16
Contextual factors
The participating survivors self-reported demographic information, such as age, gender, education level, and employment status. Other self-reported clinical information included cancer diagnosis, treatment modalities, age at diagnosis, and age at completion of treatment. The clinical information of the respondents was also verified with medical records from the hospital patient record system.
The survivors' mental well-being was evaluated using the traditional Chinese version of the World Health Organization Five Well-Being Index (WHO-5). The WHO-5 evaluates an individual's psychological well-being over the preceding 2 weeks on a 6-point Likert scale graded from 0 (at no time) to 5 (all of the time). The total raw score ranges from 0 to 25, and is multiplied by 4 to derive the final score that ranges from 0 (worse perceived well-being) to 100 (best perceived well-being). The WHO-5 has been proven to display adequate reliability and validity in the local population, with an internal consistency (Cronbach's α coefficient) of 0.86. 17 It is recognized both as a screening tool for depression and as an outcome measure in clinical trials, and has been applied internationally across a wide range of study fields. 18
Activity motivation was evaluated using the Global Activity Motivation Scale. 19 This scale was developed by University of Massachusetts Boston to measure global motivational orientation in the general population and consists of 13 items to evaluate respondents' motivation in four types of activities: working, formal volunteering, exercising, and taking classes. Respondents were asked to rate the items from 1 to 5 with 1 being “not important” and 5 being “very important.” The total score of the scale ranges from 1 (lowest level of motivation) to 65 (highest level of motivation). The traditional Chinese version of the tool was utilized in this study.
Subjective happiness was evaluated using the Subjective Happiness Scale, which is a global 4-item measure of global self-perceived happiness and has been previously validated in 2732 participants in the United States and Russia. 20 There are two items that ask respondents to identify how happy they were using both absolute ratings, as well as relative to their peers. The other two items offered brief descriptions of happy and unhappy individuals, and require respondents to rate the extent to which each description best fits them. Respondents rate their subjective happiness and satisfaction on a 7-point Likert scale graded from 1 (extremely unhappy. unsatisfied) to 7 (extremely happy/satisfied). The Traditional Chinese version was translated and has been approved by the developers.
Statistical analysis
Descriptive statistics were used to summarize the study outcomes and all of the covariates. Absolute frequency and percentage were presented for the categorical variables, while mean and standard deviation (SD) were presented for continuous variables. The independent t-test and one-way analysis of variance test (for categorical variables) and Pearson's correlation test (for continuous variables) were conducted to compare differences in study outcomes among survivors in different subgroups, in variables that were hypothesized to impact life functioning. These included sex, age at evaluation, age at diagnosis, cancer diagnosis, education, treatment characteristics, and behavioral factors. Multivariable linear regression was used to evaluate clinical/demographic, treatment, and behavioral factors associated with life functioning outcomes. Clinical factors included age at evaluation, age at diagnosis, sex, education level, and diagnosis. Treatment factors included receipt of surgery, radiation, and chemotherapy. Behavioral factors included mental well-being (WHO-5), activity motivation (Global Activity Motivation Scale), and subjective happiness (Subjective Happiness Scale). All of the statistical analyses were performed using SPSS software, version 20. All of the tests involved were two tailed and the results were considered statistically significant at p < 0.05.
Results
Eighty survivors were recruited and analyzed in this study, with a response rate of 93.0% (Supplementary Fig. S1). The demographic and clinical characteristics of the survivors are summarized in Table 1. The majority of the survivors were male (58.8%). The most common diagnosis was leukemia (53.8%), followed by CNS tumors (16.2%). The survivors were diagnosed at a mean age of 6.7 (SD = 4.8) years. The mean age of the survivors at assessment was 24.4 (SD = 6.5), which on average was 16.1 (SD = 6.1) years after completion of their cancer treatment. Most of the survivors had been treated with chemotherapy (92.5%). Over half of the survivors (55%) had completed higher than secondary school education and 10% reported that they were unemployed at the time of assessment.
Demographic, Clinical, and Treatment Characteristics of Survivors (N = 80)
Refers to individuals who reported a full-time or part-time job.
Refers to germ cell tumor, osteosarcoma, soft tissue sarcoma, and lymphoma.
Three survivors of leukemia received hematopoietic stem cell transplantation. Two survivors were treated with total body irradiation, while one survivor received chemotherapy-based conditioning regimen.
CNS, central nervous system; SD, standard deviation.
Table 2 summarizes life functioning scores in survivors as a cohort, with stratifications for clinically relevant variables. Overall, differences in scores across the four life functioning subscales were observed (p = 0.035); the survivors reported better functioning in the leisure (mean [SD] 7.01 [1.76]) and social (7.50 [1.02]) domains, compared with the homemaker (4.74 [1.19]) and work (5.47 [1.55]) domains. Among the survivors, females performed better in social functioning than male survivors (mean [SD] 7.9 [0.9] vs. 7.2 [0.7]; p = 0.007). Based on the pre-determined definitions, it can be inferred that survivors generally reported average homemaker and worker life functioning, and high leisure and social functioning. The mean [SD] total score for career development self-efficacy is 108.37 [18.76], yielding an average score of 4.51 [0.78], which fell within the definition of “fairly confident” in career planning.
Summary and Univariate Comparison of Life Functioning Outcomes Across Clinically Relevant Subgroups
The total score for each life functioning scale is 10 points. A higher score is indicative of better functioning.
The total score for career development self-efficacy is 144 points. A higher score is indicative of better self-efficacy.
Age at diagnosis was analyzed as a continuous variable. The life functioning scores were presented and stratified by age at diagnosis categories for descriptive purposes.
Higher educational attainment (p < 0.001) and older age at diagnosis (p = 0.022) were significantly associated with better performance in the work domain. Although statistical significance was not achieved, survivors with CNS tumors seemed to report poorer work functioning than survivors diagnosed with leukemia and other solid tumors (mean [SD] 4.91 [1.68] vs. 5.79 [1.53] vs. 5.22 [1.51]; p = 0.15). Survivors who were treated with cranial radiation also reported poorer social (p = 0.035) and work functioning (p = 0.023), as well as lower career development self-efficacy (p = 0.047).
Univariate analysis identified moderate association between career development self-efficacy, with personal behavioral factors motivation (Pearson correlation coefficient [rp] = 0.54; p < 0.0001) and subjective happiness (rp = 0.49; p < 0.0001). Mental health (rp = 0.24; p = 0.043), activity motivation health (rp = 0.48; p < 0.0001), and subjective happiness (rp = 0.43; p < 0.0001) were also correlated with leisure functioning (Supplementary Table S2). These behavioral factors also had significant correlation with social functioning (all p < 0.05), but not worker life and homemaker functioning.
The results of the multivariable modeling are presented in Table 3. After adjusting for sex and age at diagnosis, the survivors with secondary school education or below had poorer work functioning than those who had attained post-secondary education (β = 1.029, standard error [SE] = 0.47; p = 0.033) and tertiary education (β = 0.83, SE = 0.40; p = 0.041). The survivors diagnosed with CNS tumors (β = −0.79, SE = 0.37; p = 0.034) tended to perform worse in terms of social functioning, while the leukemia survivors (β = 0.80, SE = 0.39; p = 0.047) reported better work functioning than the survivors of other solid tumors. The survivors who had been treated with cranial radiation also had lower work functioning than those who had not (β = −1.59, SE = 0.15; p = 0.002).
Multivariable Analysis of Factors Associated with Life Functioning and Career Development Self-Efficacy
Bold denotes statistically significant values (p < 0.05).
A higher score is indicative of better functioning.
SE, standard error.
After adjusting for sex, age at evaluation, and cancer diagnosis, higher activity motivation was significantly associated with better leisure functioning (β = 0.086, SE = 0.03; p = 0.008) and social functioning (β = 0.036, SE = 0.02; p = 0.036). The survivors who reported higher scores on the subjective happiness scale also demonstrated better social functioning (β = 0.067, SE = 0.032; p = 0.045). Subjective happiness (β = 1.12, SE = 0.51; p = 0.035) and activity motivation (β = 1.04, SE = 0.26; p < 0.0001) were also associated with better career development self-efficacy (Fig. 2).
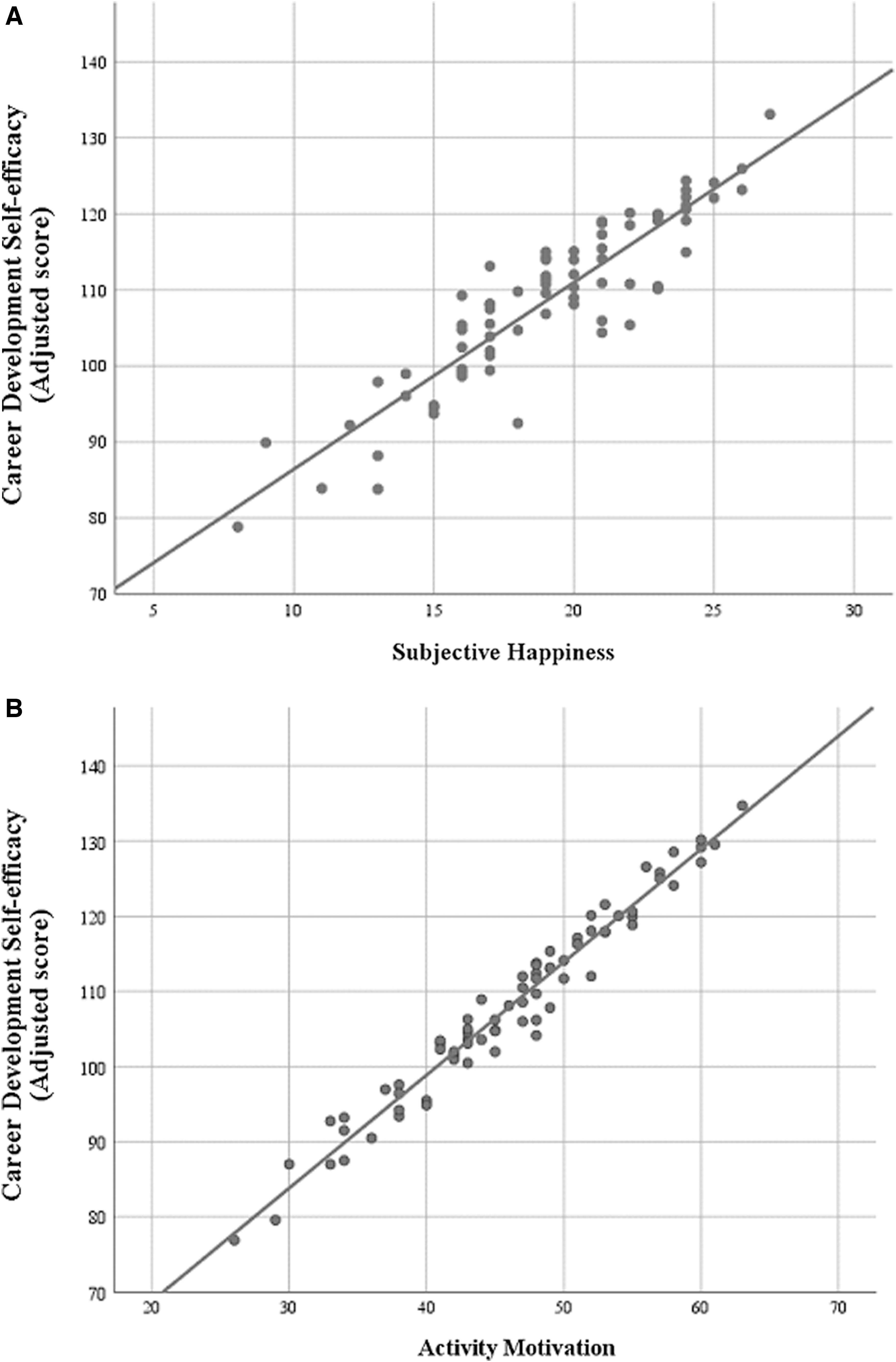
Correlation between personal behavioral factors and career development self-efficacy.
Discussion
Catastrophic diseases diagnosed in childhood and adolescence are often associated with deterioration in one's functioning and health-related quality of life. Other than the prevention of cancer recurrence and management of treatment-related late effects, survivors' performances at work or at school and social interaction skills are important indicators for recovery. To the best of our knowledge, this is one of the first studies to explore factors associated with life functioning in Chinese survivors of childhood cancer. We found that survivors generally reported good leisure and social functioning, and average homemaker and worker life functioning. Our results concurred with the finding of the existing literature that survivors who were treated with cranial radiation reported poorer work functioning than survivors who did not. Survivors diagnosed at a younger age also reported poorer work functioning. Male survivors demonstrated lower social functioning than female survivors did. Interestingly, we found that behavioral factors such as motivation and subjective happiness were associated with better life functioning and self-efficacy in survivors. This finding may have implications for developing patient-centered rehabilitation interventions to improve self-efficacy and prepare survivors as they transition into adulthood.
A population-based analysis conducted by The Childhood Cancer Survivors Study in the United States reported that 27% of survivors were unemployed, compared with 19% of sibling controls. 9 They also found that survivors who were female, diagnosed at a younger age, or had high-dose cranial radiation had a decreased likelihood of being in full-time professional occupations. 9 The reported unemployment rate in our sample of adult survivors is 10% (male: 8.5%; female: 12.1%), which seems higher than the reported average rate of 3.9% in the general population of Hong Kong between 1981 and 201921; however, the validity of this estimate may be limited by the cross-sectional design, small sample size, and single-center methodology of this study. Hence, statistical hypothesis testing to compare the observed unemployment in our sample with that in the general population was not conducted. The small sample size also did not allow us to conduct meaningful subgroup analyses to identify factors associated with poorer occupational outcomes. Our results nevertheless suggest employment challenges faced by survivors of childhood cancer. Future work will include conducting larger scale studies with more detailed assessment of survivors' career decisions and occupations to identify subgroups of survivors (e.g., those with specific cancer diagnoses and cancer treatment histories), who may require vocational assistance throughout adulthood.
Most survivorship literature has focused on evaluating health outcomes, psychosocial dimensions, and quality of life; few studies have reported on life functioning in long-term survivors of childhood cancer, especially within an Asian population of survivors. The paucity of studies in this area may be due to the lack of validated measures to evaluate the complex nature of “life functioning.” We utilized the L-FAI, which has been developed and validated with the local population. 15 Besides proving to be an acceptable function measure in both clinical and research settings, the multidimensional nature of the L-FAI allows a more accurate representation of performance in different function aspects. This characteristic is especially helpful for health care professionals in evaluating and addressing relevant issues in survivorship planning. For example, we found that compared with leukemia survivors, survivors of CNS and other solid tumors may require more social skills training as they advance into survivorship. This finding provides strong justification for local studies that have adopted innovative strategies, such as music training and integrated adventure-based training, to promote social network support for survivors of CNS tumors in Hong Kong.22,23
Our results also showed that survivors perceived higher functioning in leisure and social activities, compared with meeting the demands of work and homemaking activities. To highlight, survivors who were treated with radiation also had lower worker life functioning than those who did not. Although our study sample was relatively young, the majority were more than 10 years from the completion of treatment. Studies have shown that the cumulative incidence of chronic conditions increases approximately 10 years after diagnosis, particularly in survivors who had been treated with radiation.2,5 We speculate that treatment-related late effects and symptom burden may have limited their roles at work and at home. We speculate that as survivors age and develop treatment-related late effects, their declining health status may affect their life functioning. Our future research will include evaluating the impact of chronic conditions and symptoms on occupational, social, and economic outcomes in survivors.
This study also yielded the novel finding that global measures of activity motivation and subjective happiness are associated with better life functioning and self-efficacy in career development. This implies that motivation, which may potentially be a modifiable personal factor, may improve survivors' role functioning in society. Motivation, often defined as personal interest or desire, is considered one among a number of forces that may increase the likelihood of participation in an activity.19,24 The concept of “motivation” in our study included assessing survivors' levels of interest in learning and utilizing new skills, taking on new experiences, expanding their social network, and engaging in activities that benefit the community (e.g., volunteering). This underscores the need for an innovative care paradigm that empowers survivors during the transition process from active cancer treatment to the survivorship phase. Motivating and empowering survivors require novel strategies such as involving them as peers, mentors, and leaders to provide social and moral support for other patients with cancer.25,26 Other than systematically screening for late effects and providing education on preventive health behavior, a comprehensive survivorship program should empower survivors with the skills to meet the challenges of the workforce and improve their career advancement opportunities. This will require a multidisciplinary team comprising social workers, occupational therapists, developmental psychologists, and rehabilitation specialists to develop effective approaches to transition skills training.
There is now an evolving area of research seeking to improve care in children with cancer in China. For the last few decades, research efforts have been dedicated to cancer prevention and reducing mortality rates of childhood cancer. Large epidemiological studies have reported that childhood cancer incidence in China has significantly increased by up to 2.8% annually since 2000.27,28 With increased access to contemporary treatment, a growing cancer incidence, and reduced cancer mortality rates, China is expecting an increasing population of survivors in the next few decades. These survivors require long-term follow-up care to address both medical and psychosocial late effects of cancer treatment. Even though post-treatment survivorship care is now a recognized distinct phase of the cancer care continuum in the United States and Europe, providing comprehensive survivorship care seems to be a work in progress in China. Our findings reinforce the urgent need to develop strategies for improving confidence and transition readiness in survivors. Improving functional and psychosocial outcomes in adolescent and young adult survivors who are still in the early phase of their cancer survivorship will translate into a substantial positive impact on society.
The study had certain limitations that should be considered in the interpretation of these results. This single-center study included a relatively small sample size of survivors who were recruited through a convenience sampling approach. Moreover, eligible participants were identified from a long-term follow-up clinic that had an average default rate of 15% to 20%. This is a recognized challenge in survivorship research, as this population is often lost to follow-up from their primary pediatric clinics due to growing independence and mobility as they advance into adulthood. This may have resulted in a higher proportion of leukemia survivors in this study sample (53.8%), compared to the expected proportion of childhood leukemia cases in Hong Kong (30%). 1 These study limitations could have introduced sampling bias and reduced the validity of the findings, which may have yielded overestimates of survivors' life functioning level and self-efficacy. Although the self-reported measures adopted in this study are validated tools, they may possess suboptimal psychometric properties to measure the constructs of interest in the study population. For example, it has been reported that survivors of childhood cancer in Hong Kong tend to adjust fairly well in psychological and mental health aspects 8 ; hence the WHO-5 used to measure mental well-being may not be sensitive enough to identify associations between mental well-being and life functioning in multivariable analysis. As survivors self-reported their life functioning, psychological well-being, and subjective happiness data, the internal validity of the findings should be interpreted cautiously due to potential common source bias. The multiple predictors and covariates analyzed in this study may increase the risk of committing a Type I error. However, functioning itself is a complex phenotype that is likely influenced by intrinsic and extrinsic factors; we would like to emphasize that the clinical, treatment, and behavioral factors of interest were selected based on existing evidence that suggests their plausible association with life functioning. Furthermore, we did not collect information on other important variables that may influence life functioning, such as late effects associated with the cancer treatment, childhood socioeconomic status, and spirituality. Finally, this study also did not include an age-matched healthy comparison control group. However, our results are consistent with the robust literature that identifies treatment factors such as cranial radiation and CNS diagnosis as predictors of poor functioning. Despite these limitations, this study serves as a feasibility study and a model to facilitate larger-scale research to validate the preliminary findings of this study. A multicenter study that involves prospective collection of outcomes data may also better reflect the trajectory of occupational functioning and limitations in Chinese survivors of childhood cancer as they advance from early to long-term survivorship.
Conclusion
Our results show that survivors of childhood cancer in Hong Kong report reduced functioning in meeting demands at work and at home. Survivors of CNS tumors and survivors who were treated with radiation have poorer life functioning, particularly in social and work domains. Future work includes conducting a multicenter study to validate the findings in a larger sample of survivors in Hong Kong. Occupational needs and limitations should also be evaluated prospectively in this population. To maximize survivors' career opportunities and potential, long-term survivorship programs should offer vocational assistance to survivors as they transition into adulthood. High-risk survivors may require additional and ongoing support from community educational or vocational services. Addressing modifiable behavioral factors include motivating survivors to engage in meaningful activities that contribute to self-care, enjoyment, and participation in society.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.