
Abstract
We describe three children who developed an osteosarcoma after receiving treatment for acute lymphoblastic leukemia, which included an allogeneic bone marrow transplant (BMT). We discuss the therapeutic options. None of the patients responded to conventional chemotherapy, but one patient given regorafenib showed a temporary response. We conclude that osteosarcoma after BMT has an aggressive course and it is worth further investigating multikinase inhibitors in this setting.
Introduction
Secondary malignancies after treatment for cancer have become a major health issue since therapies have been more successful and patient survival has increased.1,2 Osteosarcoma is the most common primary bone cancer in children and adolescents, and one of the most common secondary malignancies after treatment for solid tumors. It has rarely been reported, however, after treatment for hematological neoplasms: in a series of 152 children with primary acute lymphoblastic leukemia (ALL), only 2.6% developed secondary bone tumors. 3
Osteosarcoma after bone marrow transplant (BMT) is also very rare, but tends to be locally invasive, and often metastatic; and the reported prognosis is poor.4–14
This report describes three children with ALL who underwent BMT and subsequently developed secondary osteosarcoma. The treatment options are discussed.
Case Report
Case 1
A 3-year-old girl was diagnosed with preB-ALL and given chemotherapy according to the Associazione Italiana di Emato-Oncologia Pediatrica (AIEOP) 8803 protocol, which consisted in polychemotherapy associated with cranial irradiation (1800 cGy). A bone marrow relapse occurred 2 years after completing the treatment. The patient was then given second-line chemotherapy and underwent BMT from a mismatched unrelated donor after a conditioning regimen that included thiotepa, cyclophosphamide, and 1200 Gy total body irradiation (TBI). Ten years later (at the age of 15), the patient presented with pain in the left hip. A computed tomography (CT) scan revealed a lesion 12 × 10 cm in size in the left hip bone with a marked periosteal reaction. Biopsy pointed to osteosarcoma with a diffuse chondroblastic component. No metastatic lesions were documented. The search for the p53 mutation was negative.
The patient received chemotherapy with methotrexate, cisplatin, doxorubicin, and ifosfamide according to the Italian ISG/OS-1 osteosarcoma protocol. 15 After six cycles of therapy, a CT scan revealed local and distant (right hip) disease progression. Despite second-line chemotherapy with high-dose ifosfamide and cyclophosphamide/etoposide, further disease progression was documented. The patient was enrolled in a study on radionuclide therapy with samarium. The severe myelosuppression deriving from this therapy ultimately led to the patient's death 15 months after her osteosarcoma was diagnosed.
Case 2
A 12-year-old girl was diagnosed with common ALL and treated according to the AIEOP-BFM 2009 protocol (high-risk group). She received a BMT from her brother after a conditioning regimen that included thiotepa, cyclophosphamide, and TBI (1200 cGy). Three years after the BMT (at the age of 17), she complained of pain and swelling of the left leg. Magnetic resonance imaging (MRI) revealed a hypointense 15-cm-long lesion extending from the epiphysis to the mid-proximal diaphyseal region of the left tibia. A biopsy led to a diagnosis of osteosarcoma. No metastases were found.
Chemotherapy was given according to the Italian ISG/OS-2 sarcoma protocol, but the patient developed severe tubulopathy after the first cycle (high-dose methotrexate). A new CT scan revealed the appearance of multiple lung lesions. Given her low tolerance of chemotherapy, the patient underwent primary tumor resection followed by gemcitabine-docetaxel therapy. Seven months after she had been diagnosed with osteosarcoma, a local relapse with an intracardiac metastasis was documented. The patient died 2 months later. A diagnosis of Li–Fraumeni syndrome was established postmortem.
Case 3
A 10-month-old male child was diagnosed with ALL and given chemotherapy according to the AIEOP ALL protocol for infants. During the maintenance phase, the patient had an isolated central nervous system relapse. Second-line chemotherapy was followed by allogeneic BMT after a conditioning regimen that included thiotepa, cyclophosphamide, antithymocyte globulin, and TBI (1440 cGy). Twelve years after his BMT (at the age of 15), the patient complained of pain and swelling of the right thigh. MRI and CT scan revealed a 16 × 7 cm lesion and multiple pulmonary nodules. The search for the p53 mutation was negative.
A biopsy identified an osteosarcoma and treatment was initiated according to the ISG/OS-2 protocol, but after two cycles of chemotherapy there was evidence of local and distant tumor progression, and also of pulmonary embolism. The patient was given high-dose ifosfamide, but the treatment was stopped due to neurological toxicity (drowsiness and asthenia, grade 2 CTCAE). Then palliative radiotherapy to the primary tumor was administered. In the light of recent publications,16,17 compassionate treatment with regorafenib was started at a dose of 100 mg (82 mg/m2) on days 1–21 of each 28-day cycle. The treatment was well tolerated and, after the first cycle, CT showed a reduction in the number and size of the patient's lung metastases (Fig. 1).
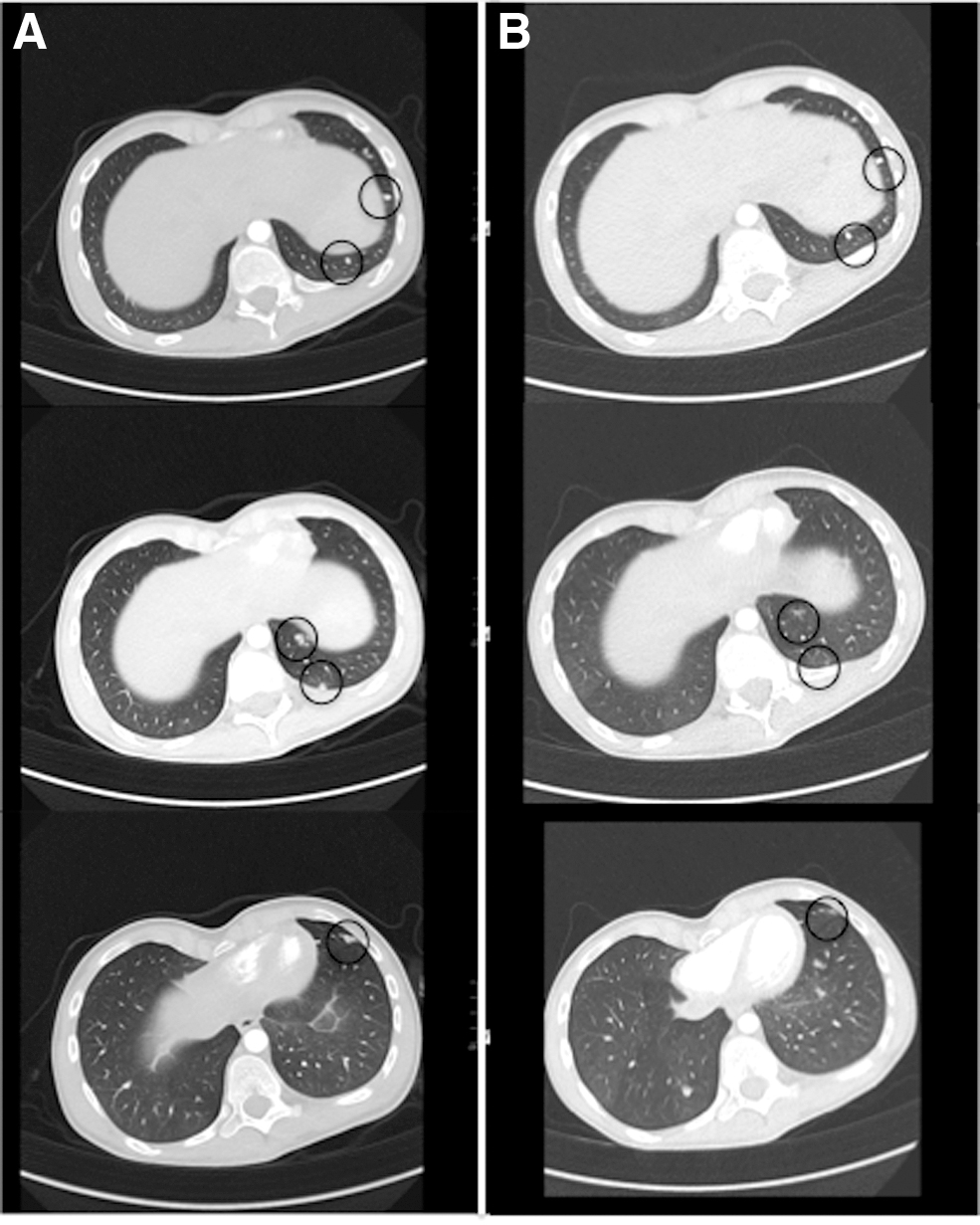
Lung metastases before treatment with regorafenib
There was also a reduction in the size of the leg mass (to which radiotherapy was administered as well), with a complete regression of the associated pain. On reassessment after the second cycle, an asymptomatic left pneumothorax was identified, which was attributed to cavitation of a subpleural lesion; it was drained surgically. After 4 months of regorafenib, the primary tumor remained stable, but a modest increase in the lung metastases and embolic lesion was documented. The patient died 8 months after starting regorafenib.
Discussion
A secondary tumor is the most feared consequence of antineoplastic treatment for a primary malignancy in children. Osteosarcoma is a common secondary malignancy, especially in patients previously treated for retinoblastoma, Ewing's sarcoma, 18 rhabdomyosarcoma, 19 or Hodgkin lymphoma. 20 Children are at higher risk if they carry germline mutations predisposing to cancer such as p53 in the Li–Fraumeni syndrome 21 that we found in one of our patients.
Osteosarcoma after treatment for leukemia is rare. In a population-based cohort study from the Nordic countries, 22 no osteosarcomas were detected among eight second tumors developing in 895 children with ALL. There were also no bone tumors among 43 second malignancies occurring in a population of 9720 children with ALL in a study performed by the Children's Cancer Study Group. 23
Second tumors are an important complication of BMT, but secondary osteosarcoma has rarely been reported in this setting.4–14 The few reports on the outcome of osteosarcoma after ALL and/or BMT suggest that this is an aggressive tumor with a poor prognosis. We found 21 cases of osteosarcoma secondary to allogeneic BMT in the literature.4–14 The median age at diagnosis was 15 years (range 7–26 years). The reason for BMT was ALL in 13 patients, whereas the others were single cases of acute myeloid leukemia, neuroblastoma, chronic granulomatous disease, Blackfan-Diamond anemia, congenital amegakaryocytic thrombocytopenia, myelodysplastic syndrome, and non-Hodgkin lymphoma. Follow-up data were available for 20 patients, and 9 deaths were related to osteosarcoma. Interestingly, a significant proportion of the patients who died had BMT prompted by ALL (7 of 13 patients).
In our experience, osteosarcoma developing after BMT had a very aggressive behavior. All three primary lesions were large, and there were already lung metastases at diagnosis in one case. Our patients were treated with the chemotherapy in use for newly diagnosed osteosarcoma, but response was poor, and further attempts with different regimens failed to improve the situation.
A possible cause of such aggressive behavior is the previous treatment and in particular the administration of TBI. As shown in several studies radio-induced sarcomas 24 are often resistant to conventional chemotherapy, making highly challenging the management of these diseases, also in the pediatric population. 25
In our patients chemotherapy tolerance was also poor, with two patients experiencing renal and neurological toxicity. Their previous treatments, including allogeneic BMT, may have made these children more susceptible to the negative effects of chemotherapy, even if it was administered 3 and 12 years later.
In this context, the response seen in one patient already after one cycle of regorafenib is of interest, even though the benefit was temporary. The activity of regorafenib (a multikinase inhibitor) against refractory or relapsing osteosarcoma had previously been tested in two studies. Duffaud et al. 16 treated 38 patients from 18 to 74 years old, 26 given regorafenib, and 12 a placebo. After 8 weeks of treatment, there was no disease progression in 17 (65%) of those given regorafenib (compared with none in a placebo group). The median progression-free survival (PFS) in the regorafenib group was 16.4 weeks (compared with 4.1 weeks with placebo), with a partial response in 2 patients (8%) and stable disease in 15 (58%).
Similar results were obtained by Davis et al. 17 in 42 patients from 18 to 76 years (median age 37 years), 22 given regorafenib and 20 a placebo. The median PFS was 3.6 in the regorafenib group and 1.7 months in the placebo group, with a PFS at 16 weeks of 44% and 10%, respectively (p = 0.027). A partial response was observed in three patients treated with regorafenib (13.6%).
Regorafenib-related toxicity was not negligible. It prompted temporary suspensions of the treatment in 35% of cases, and dose reductions in 38% of the cases described by Duffaud. In the article published by Davis et al., 17 one patient experienced grade 3 pneumothorax, and one had grade 4 colonic perforation, both attributed to regorafenib.
Despite evidence of activity, regorafenib as monotherapy failed to produce any complete response. Its role in the treatment of osteosarcoma needs to be further explored.
In conclusion, our experience confirms that osteosarcoma after BMT is very difficult to treat. It is often resistant to standard chemotherapy, and toxicity is higher than in osteosarcoma patients with no history of BMT. Our experience suggests that regorafenib may have some activity in cases of secondary osteosarcoma.
Footnotes
Acknowledgments
This study was partially supported by the Alto Adige Peter Pan Association for children with cancer, Bolzano, Italy.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no specific funding for this work.