
Abstract
Purpose:
The number of adolescent and young adult (AYA) survivors of childhood cancer is increasing, and the impacts of therapy on their daily lives are not well understood. Adaptive functions are required for age-appropriate interactions and day to day functioning, but are reduced in AYA survivors. Work in other pediatric populations suggests that additional neurocognitive skills may influence adaptive function and, thus, quality of life and personal attainment of AYA cancer survivors.
Methods:
Retrospective medical records review examined neurocognitive data from 139 AYA survivors. Hierarchical linear regression examined age at diagnosis, use of central nervous system (CNS) radiation, verbal intelligence, processing speed, and executive function as predictors of adaptive functioning domains.
Results:
AYA survivors exhibited weaknesses in all domains of adaptive functioning compared to normative reference values (Cohen's d = 0.660–0.864), as well as in processing speed (Cohen's d = 0.791) and metacognitive executive functioning (Cohen's d = 0.817). Processing speed and executive function provided substantial improvements in prediction of adaptive functioning beyond that of age at diagnosis and use of CNS-directed radiation therapy. Taken together these variables explained 37.1% of variability in adaptive conceptual skills, 26.1% in adaptive social skills, and 27.1% of adaptive practical skills.
Conclusions:
Intelligence, processing speed, and executive function significantly contribute to adaptive function scores in AYA cancer survivors and impact domains that are important to self-sufficiency and quality of life. Attention to neurocognitive function in all AYA cancer survivors is recommended in addition to referral for neuropsychological evaluation and tailoring interventions to address executive and adaptive functioning.
Introduction
The annual incidence of cancers in children, adolescents, and young adults below age 39 years has increased to 75.7 per 100,000 persons. 1 Fortunately, survivorship rates for these patients have been increasing, and the 5-year survival rate for children, adolescents, and young adults (AYAs) diagnosed with cancer has increased to 83%–85%, 1 which means that the number of AYA survivors of cancer is increasing and will continue to do so. The improved survivorship is attributed to multiple factors, including an increase in the intensity of therapies. Unfortunately, the therapies required to treat cancer can create lifelong neurocognitive effects that significantly impact quality of life, cognitive functioning, and overall personal achievement.2–4
Survivors of childhood cancers exhibit significant differences in academic and neurocognitive functioning, with deficits in multiple cognitive domains, including numerical processing, executive function, and adaptive function, compared to those without a history of cancer.5–8 Children who receive central nervous system (CNS) directed chemotherapy or radiation therapy later exhibit dose-dependent cognitive toxicities from therapy. 5 Because of the unique developmental expectations facing AYAs, treatment-related cognitive impairments create significant challenges for development of age-appropriate skills and self-sufficiency that are hallmarks of this developmental stage. Neurocognitive impacts of therapy have been reported as the second most concerning self-identified symptom after treatment by AYAs, 3 and these cognitive effects create tremendous challenges to the transition back to work or school post-therapy. 9 As a result, AYAs have survivorship and psychosocial supportive needs that are unique from other age groups. 10
Adaptive function skills include a person's ability to care for themselves, navigate effectively within home and community settings, and interact with others at an age-appropriate level; these skills reflect how well a person functions independently and may be negatively impacted by chemotherapy and radiation therapy.5,8,11 Changes in adaptive function have been shown to reflect a dose-dependent effect of craniospinal radiation therapy in cancer survivors.8,12 AYA survivors treated with chemotherapy show diminished cognitive and educational attainment compared to those without a history of cancer. 13 Young adult survivors of childhood cancer and those with worse neurocognitive impairment are also less likely to live independently compared to healthy siblings. 14
Executive functions are proposed contributors to adaptive skills given the need to initiate timely actions and regulate responses in real-world settings and are common areas of weakness in survivors of childhood cancers.15–18 Executive functions are processes that are required to control one's own behavior and emotions and include attention regulation, inhibitory control, working memory, and cognitive control and flexibility. Executive function has been identified as a predictor of adaptive function in children with a variety of noncancer populations,20–22 but less work has examined this association in AYA survivors of childhood cancer. As survival rates increase, there is a need to better understand what life will look like after cancer treatment in AYAs as their executive and adaptive demands increase. Furthermore, few studies exist that clarify how known areas of neurocognitive risk (e.g., reasoning ability, processing speed, and executive function) relate to functional adaptive outcomes in AYA survivors.
The purpose of the present study is to describe the adaptive function of AYA survivors and examine prediction of adaptive function from clinical demographic variables (age at diagnosis, type of diagnosis, and use of CNS-directed radiation therapy) and cognitive function (verbal intelligence and executive function).
Methods
A retrospective cross-sectional study was conducted at the Kennedy Krieger Institute and Johns Hopkins Children's Center in Baltimore, Maryland. Approval for this study was provided by the institutional review board.
Participant sample
Patient records at the Kennedy Krieger Institute's Department of Neuropsychology were reviewed to identify AYAs aged 14–39 years at the time they underwent clinical neuropsychological testing. These evaluations were completed after clinical referral and included a standard battery of cognitive assessments based on age; scores from the adaptive behavior, intelligence, processing speed, and executive function measures were used for analysis. To provide consistency across the age span, only parent or caregiver ratings were utilized for the adaptive behavior and executive function scales. As such, not all participants had assessments for all measures of interest completed (i.e., when a young adult was not accompanied to the visit by a parent); subsamples with data on each measure of interest are shown in Table 2. Treatment information was confirmed from medical records to verify oncology diagnosis, age at diagnosis, sex, race/ethnicity, and use of CNS-directed radiation therapy.
Adaptive and Neurocognitive Scores Compared to Normative Values
p < 0.001.
p < 0.05.
p < 0.01.
ABAS, Adaptive Behavior Assessment System; IQ, intelligence quotient.
Measures
Adaptive function was measured with the Adaptive Behavior Assessment System (ABAS) second and third editions,23,24 a psychometrically reliable and validated tool for caregiver report of adaptive behaviors and skills for daily life. The measure evaluates nine adaptive skill areas and provides a norm-referenced composite score for three domains (conceptual, social, and practical) and an overall summary adaptive composite. The conceptual domain assesses behaviors required for communicating with others, managing and accomplishing needed tasks, and applying academic skills to daily tasks. The practical domain measures behaviors needed to manage home, classroom, or work settings, care for personal hygiene, and navigate one's community. Social domain behaviors include interacting interpersonally, acting with social responsibility, and engaging appropriately in leisure activities. Higher scores indicate better adaptive function.
Intelligence was assessed with the age-appropriate standardized measure, including the Wechsler Intelligence Scale for Children, fourth and fifth edition, Wechsler Adult Intelligence Scale fourth edition, or the Reynolds' Intellectual Assessment Scale.25–29 These measures estimate overall composite intelligence quotient (IQ), verbal and nonverbal reasoning, and/or processing speed. Given the recognized risk of reduced processing speed in survivors, the verbal reasoning composite (Verbal Comprehension Index; Verbal Ability Index) was used as an estimate of cognitive ability, as the verbal composite does not rely upon speeded responding or graphomotor skills, as does the overall or full-scale score.
Processing speed was assessed with the Processing Speed Index (PSI) from the age-appropriate Wechsler measure. The PSI assesses the participant's efficiency of scanning a page of symbols, processing the information, and providing a graphomotor (e.g., pencil and paper) response. All scores are compared against normative age-specific data; higher scores indicate greater processing efficiency.
Executive function was assessed with parent ratings on the Behavior Rating Inventory of Executive Function (BRIEF), first and second editions.30,31 The BRIEF is a psychometrically sound rating scale designed to assess the application of executive skills in the individual's typical daily environment and yields age-referenced summary behavior regulation and metacognition (e.g., cognitive regulation) composite scores relative to the normative sample. Higher scores indicate greater difficulty with executive function. As with the adaptive ratings, parent ratings rather than self ratings were used to avoid self-report bias or developmental variability in insight.
Diagnosis and treatment information were extracted from medical records. The diagnoses were categorized by disease groups; leukemia/B cell lymphoma, brain tumors, and solid tumors. Solid tumors included patients with a history of Ewing sarcomas (n = 4), rhabdomyosarcoma (n = 2), osteosarcoma (n = 1), Hodgkin lymphoma (n = 2), Langerhans cell histiocytosis (LCH; n = 3), nasopharyngeal carcinoma (n = 2), neuroblastoma (n = 2), desmoplastic round cell tumor (n = 1), nongerm cell testicular tumor (n = 1), and testicular cancers (n = 1) that were treated with systemic, potentially neurotoxic, chemotherapy. Patients with LCH were included in the sample as they also received systemic cytotoxic chemotherapy. All solid tumors (other than brain tumors) were grouped together for analysis as the therapy did not include CNS directed treatments. CNS-directed therapy was defined as any targeted radiation therapy delivered to the brain, including targeted boost of CNS radiation for stem cell transplant conditioning, or intrathecal chemotherapy.
Statistical analysis
One-sample t-tests compared mean AYA survivor scores to population normative data across outcomes of interest. Hierarchical linear regression models examined prediction of adaptive composite scores from intelligence (verbal IQ), processing speed, and executive function (behavior regulation and metacognition composites). Given the well-documented impacts that age at diagnosis and use of CNS-directed radiation therapy have on neurocognition,32–34 these variables were included in all models.
Results
Of the 139 participants included in this study, 108 had ABAS scores available for analysis, which is the primary outcome of interest for this study; participants with missing ABAS data were retained to analyze mean IQ, processing speed, and executive function scores. Table 1 displays participant characteristics. The average age at the time of diagnosis was 11.5 years (standard deviation [SD] = 5.7 years). Just over half of the patients were male (n = 59; 57.6%) and identified as white (n = 95; 68.3%). The most frequent diagnoses were brain tumor (n = 77, 55.4%) and leukemia/non-Hodgkin lymphoma (n = 43, 30.9%), with the remaining 19 (13.7%) patients treated for a solid tumor.
Patient Demographics
CNS, central nervous system; n, number; RT, radiation therapy; SD, standard deviation.
General neurocognitive functioning
AYA survivors of childhood cancers as a group scored significantly below normative mean of 100 (SD = 15) across all adaptive function domains and processing speed (Table 2). Although group mean scores fell largely within one standard deviation of the normative mean, the number of AYA survivors who scored >1SD below the mean was higher than expected based on normative data (Fig. 1). Based on a normative distribution, no more than 16% of participants would be expected to score worse than 1SD from the mean, but 35% to 45% of these AYA participants scored worse than normative means in adaptive conceptual, adaptive social, adaptive practical, metacognition, and processing speed domains.
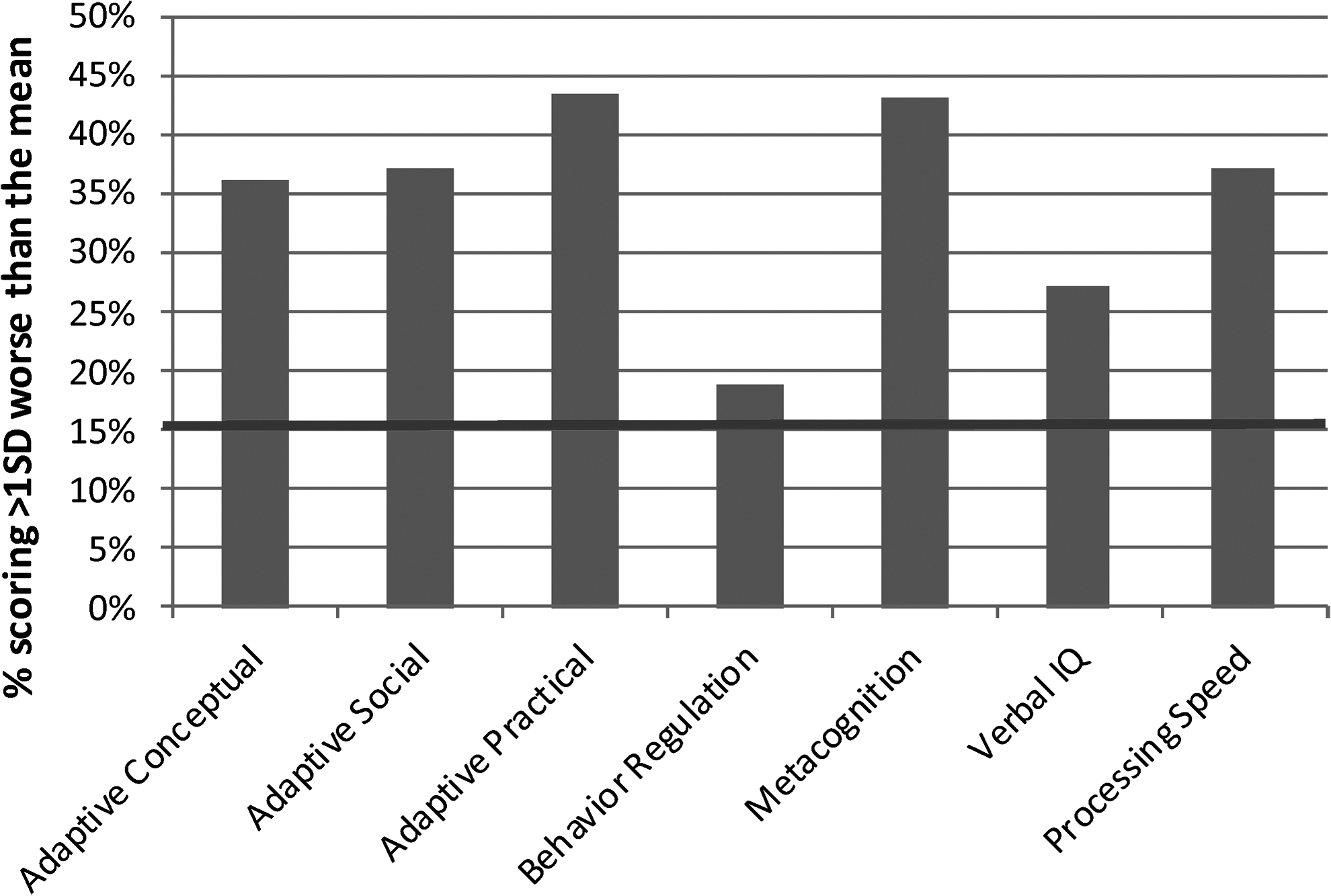
Percent of the sample performing more than 1SD (e.g., >16%) worse than the normative mean for each adaptive and neurocognitive domain. Bold horizontal line indicates the expected 16% ≤ 1SD of the normative mean. SD, standard deviation.
As a group, their verbal IQ scores also differed significantly from the normative mean, but this difference was not present when evaluated based on diagnosis group; it is important to note that all group means fell within five standard score points of the mean (e.g., 0.33SD) and well within the average range. Likewise, mean processing speed scores were significantly below the normative mean of 100 (SD = 15) for AYA survivors as a group (Cohen's d = 0.791), as well as for the brain tumor (d = 0.978) and leukemia (d = 0.680) groups, but not for patients with a history of solid tumors (mean = 95.94; d = 0.303). With regard to executive functioning, all AYAs were consistently rated as showing significantly higher scores (indicating greater difficulty) relative to age-referenced norm of 50 (SD = 10) for metacognitive executive skills (Cohen's d = 0.817). There was not a significant difference in behavioral regulation skills (d = 0.064) with the exception of AYAs with a history of leukemia, who also exhibited somewhat more difficulty with behavioral regulation than expected for age (d = 0.399).
Adaptive behavior
Utilizing hierarchical regression analysis, we examined the impact of each hypothesized predictor on adaptive function domain while controlling for treatment-related variables of age at diagnosis and use of CNS-directed radiation therapy, neither of which predicted adaptive outcomes (Table 3). Measures of verbal intelligence, processing speed, and executive function (behavior regulation and metacognition composite scores) were entered into the model individually and sequentially to evaluate their contribution to prediction of adaptive behavior scores (e.g., change in R2, or ΔR 2 ).
Hierarchical Linear Regression on Adaptive Function Scores
Bold indicates p-values < 0.05.
Each variable entered sequentially in separate blocks; β = beta for each block sequentially.
Adaptive conceptual
After controlling for the treatment related variables of age at diagnosis and CNS radiation, verbal IQ scores accounted for a significant proportion of variability in parent-rated conceptual composite scores (ΔR 2 = 0.086, p = 0.005). Over and above the treatment related variables, the addition of processing speed accounted for an additional 5.3% (p = 0.023) of the variance in adaptive conceptual skills. Finally, both the metacognition (ΔR 2 = 0.186, p < 0.001) and behavior regulation (ΔR 2 = 0.039, p = 0.026) composites added significantly to prediction of conceptual adaptive functioning. Even with executive function scores in the model, verbal IQ (β = 0.202, p = 0.028) and processing speed (β = 0.281, p = 0.03) remained unique predictors of AYA's conceptual adaptive skills. Taken together, the model accounted for 37.1% of the variability in adaptive skills.
Adaptive social
After controlling for the treatment related variables, neither verbal IQ nor processing speed accounted for a significant amount of variance in adaptive social functioning (VIQ: ΔR 2 = 0.005, p = 0.510; PSI: ΔR 2 = 0.026, p = 0.128). However, the metacognition composite accounted for an additional 17.3% of the variance (p < 0.001), with behavior regulation also contributing uniquely (ΔR 2 = 0.035, p = 0.049) to social adaptive domain scores. With all predictors in the model, processing speed (β = 0.208, p = 0.039) emerged as an additional unique predictor of social functioning. Taken together, the model explained 26.1% of the variance in social adaptive functioning.
Adaptive practical
After controlling for the treatment related variables, verbal IQ accounted for an additional 5.4% of the variance (p = 0.026) in practical adaptive domain scores. With treatment related variables and verbal IQ in the model, processing speed also explained a significant proportion of additional variance (ΔR 2 = 0.077, p = 0.006). Finally, metacognitive executive skills (ΔR 2 = 0.105, p = 0.001), but not behavioral regulation (ΔR 2 = 0.005, p = 0.452), accounted for unique additional variance in practical adaptive functioning. With all predictors in the model, processing speed (β = 0.322, p = 0.002), but not verbal IQ (p = 0.174), remained a significant unique predictor of practical composite scores. Taken together, the model explained 27.1% of the variance in practical adaptive skills.
Discussion
Findings from this cross-sectional study show that AYA survivors of childhood cancers referred for neuropsychological testing exhibit significant weaknesses across cognitive domains. These effects are not limited to patients with a history of brain tumors, leukemia/lymphoma, or CNS-directed therapy; groups commonly considered to be at highest risk. There are important cognitive factors that explain these deficits beyond diagnosis and therapy alone.
Cognitive profile of AYA survivors
Similar to prior studies, our investigation demonstrated that survivors of childhood cancers are at risk for lasting neurocognitive effects.5,6,8,15,35 The AYA survivors in this study exhibited substantive impacts on all domains of adaptive function when examined as an entire group compared to normative data, with moderate to large effect sizes (Cohen's d > 0.660 for all domains). Survivors also had significantly slower processing speed and metacognitive executive dysfunction compared to normative data. It is notable that, on average, these AYAs demonstrated broadly average intelligence, suggesting that the functional weaknesses observed in adaptive and executive function are not solely due to reduced IQ. With regard to executive function, cognitive aspects of self- and task-regulation (e.g., metacognition) were more consistently affected than behavioral and emotional regulation (large vs. small effects, respectively).
Importantly, these differences in neurocognitive functioning were not limited to patients who received CNS-directed therapy. Patients with a history of solid tumors who did not receive intrathecal chemotherapy or CNS radiation therapy also exhibited weaknesses in adaptive function and metacognitive executive functioning. Oncology providers who care for these patients should be aware that the lack of cranial radiation, brain surgery, and CNS-directed therapy does not prevent these patients from developing neurocognitive deficits and should consider the impacts that systemic chemotherapy or a cancer diagnosis alone may have on key domains of functioning. This study suggests that patients who have a history of solid tumors, who have previously not been thought of as high risk, may develop some neurocognitive challenges after cancer therapy. The small sample size and heterogeneity of diagnoses within this group preclude identification of which types of solid tumor diagnoses might present the most risk; however, these data do suggest the importance of ensuring access to neurocognitive screening and/or assessment for these patients.
Predictors of neurocognitive function and adaptive behavior
Intelligence, processing speed, and executive function together explained a substantial amount of variability in adaptive function in AYA survivors of childhood cancers, over and above that explained by age at diagnosis and CNS-directed therapy. Overall, metacognitive executive function was the most consistent and sizable predictor of adaptive functioning across domains. The scales comprising the metacognition composite assess skills of initiation, working memory, planning and organizing (setting goals, establishing steps to reach goals, carrying out tasks), organization of materials, and self-monitoring.30,31 These are critical life skills for meeting daily expectations across settings (e.g., home, classroom, and work environments), and it is clear that the lack of these key skills could limit day to day performance substantially, even in the context of generally age-appropriate IQ. As metacognition was most consistently and significantly correlated with adaptive behaviors, identification and implementation of strategies to mitigate impacts to metacognition during and following cancer therapy may have profound impacts on the daily lives of survivors.
Behavior regulation added to the hierarchical model of conceptual and social adaptive functioning for survivors beyond metacognition, speed, and verbal IQ. Behavior regulation includes the ability to control impulses, easily transition from one activity/situation to another, and appropriately regulate emotional responses.30,31 The ability to regulate one's own behavioral reactions can impact functional adaptive behaviors (e.g., initiating or completing needed tasks even when the individual prefers another activity) and influence an individual's ability to excel in their environment.
Processing speed was significantly associated with adaptive conceptual and adaptive practical functioning for survivors. The inability to quickly ingest, interpret, and use information has a negative impact on the ability to develop adaptive conceptual skills and may impact skills needed to communicate, accomplish tasks, and utilize academic skills efficiently. Likewise, delayed processing speed has some influence on the ability to develop adaptive practical skills for self-sufficiency, self-care, and future-oriented planning tasks.
Predictors of diagnosis and radiation with adaptive function
In contrast to prior work,5–8 we did not find that age at diagnosis or CNS radiation correlated with functional outcomes. We did find that all diagnosis groups had lower than expected adaptive function scores independent of CNS radiation. Data utilized in this study were extracted from records of patients who were referred for neuropsychological evaluation, meaning that they likely had some cognitive function concerns that prompted a referral from the parent, patient, or oncology team, which introduces some selection bias and may explain why there is not a notable difference due to radiation therapy.
Nonetheless, these findings suggest that neurocognitive challenges after treatment are not limited to those who received CNS-directed therapy. Rather, children and AYAs with solid tumors, those who do not receive radiation therapy, and patients who do not undergo brain surgery are also at risk for adaptive behavior difficulty after therapy. Furthermore, there may be some impact of the lived experience of having cancer or undergoing cancer treatment as a child that limits the development of executive function and adaptive behavior skills because treatment interrupts typical development and can result in fewer opportunities to take on greater independence.
Limitations
Limitations of this study arise mainly from the retrospective cross-sectional design. First, there are no pretreatment neuropsychological assessments available for comparison, removing the ability to determine degree of change after diagnosis and treatment. However, the literature is rich with descriptions of negative neurocognitive impacts from therapy, which suggests that the uniform deficits across domains seen in this study are likely related to diagnosis and treatment. Second, there is a strong selection bias within this sample because all patients for whom these data were extracted were referred for neuropsychological testing and likely exhibited a degree of neurocognitive difficulties that warranted a need for further evaluation and management and, therefore, may not reflect the entirety of the AYA survivor population.
Future directions
Future research should focus on determining the degree to which these patients experience neurocognitive changes after therapy for childhood cancers, including longitudinal prospective evaluations. There is little evidence yet that specific, noncontextual executive function interventions provide lasting improvements in these skills for survivors of childhood cancer. The use of computerized cognitive interventions and telephone-based coaching for children with a history of brain tumor or leukemia has shown some potential for supporting working memory, processing speed, and cognitive flexibility.36,37 Supporting the use of technology either through web-based intervention programs or online calendars, reminders, and organizational platforms may support development of executive skills or provide a means to mitigate the daily impacts of lower executive skills. 38 Structured interventions with cognitive behavioral therapy, cognitive training, relaxation coaching, stress management, and occupational therapy have also been suggested as potentially beneficial for survivors. 39 Interventions tailored to the challenges imposed by chemotherapy, radiation therapy, and hospitalization that accompany a cancer diagnosis may prove to be more successful in improving neurocognitive functioning than existing standard approaches.
The Children's Oncology Group notes that survivors who have received CNS radiation, brain surgery, or therapy with cytarabine and/or methotrexate (which mainly includes children with brain tumors or leukemia) are at risk for neurocognitive effects from therapy and should be monitored for deficits after treatment. 40 However, these findings suggest that patients who did not receive these therapies may still develop cognitive challenges that can impact daily adaptive outcomes.
Current practices of referring survivors for neuropsychological evaluation based on disease or treatment associated factors may miss patients who require neuropsychological services. Survivors of childhood cancers should undergo routine screening for difficulties in domains of adaptive function after therapy during follow-up with the oncology team 41 so that providers identify the need for referral early in the survivorship phase. Standardizing the lexicon used to define the role of neuropsychology teams in caring for these patients will be important in helping identify survivors most in need of support, and neuropsychologists should be incorporated into the interdisciplinary cancer care team. 42
Conclusion
This study reinforces prior findings that AYAs who have completed treatment for childhood cancer may have neurocognitive deficits that could impact the ability to fully meet expectations for age appropriate functioning. Adaptive function reflects how well a survivor is able to navigate and function independently in adulthood, and we identify some previously unexplored relationships that suggest weaknesses in intelligence, processing speed, and/or executive functioning after therapy, which may substantially limit day to day adaptive outcomes. By improving understanding of how these deficits manifest, and identifying strategies to support AYA survivors, the burden of cancer treatment in children may be eased so that survivors have the opportunity to reach their fullest functional potential.
Footnotes
Acknowledgments
None to disclose, all persons who had contributed meaningful input to this work are listed as authors.
Author Disclosure Statement
Authors have no disclosures to state; there are no conflicts of interest to declare.
Funding Information
No funding was received for this project.