
Abstract
Hypogammaglobulinemia is a poorly described complication of chemotherapy in adolescents and young adults (AYAs, 15–39 years) with acute lymphoblastic leukemia (ALL). The majority of AYAs treated on a Berlin–Frankfurt–Munster-based ALL regimen experienced hypogammaglobulinemia (65.0% [13/20]). Febrile neutropenia episodes (throughout the treatment course) and infectious events during maintenance occurred more frequently in hypogammaglobulinemic patients compared with patients with normal immunoglobulin G levels (n = 7) (median 1.0 vs. 0.0, p = 0.02; 7.0 vs. 3.0, p = 0.02, respectively). Hypogammaglobulinemia did not impact overall or event-free survival. Further studies are needed to elucidate the etiology of hypogammaglobulinemia and to establish criteria for immunoglobulin replacement in these patients.
Introduction
Acute lymphoblastic leukemia (ALL) affects 1 of 100,000 adolescents and young adults (AYAs; 15–39 years). 1 Compared with younger patients, AYA ALL patients have inferior outcomes, with 3-year event-free survival rates (EFS) of ∼60%. 2 The use of intensive, pediatric-based chemotherapy protocols has improved survival, particularly in older adolescents. 3 Increased frequency of severe infections may contribute to the reduced survival observed in AYA patients compared with younger patients. 3 However, risk factors, other than neutropenia, 4 that predict infection during treatment are unknown.
Intensive chemotherapy regimens often cause attenuated humoral and cellular responses. 5 Chemotherapy- and immunotherapy-induced hypogammaglobulinemia have been previously described in pediatric ALL patients,5–10 and in adults with other malignancies.11,12 Hypogammaglobulinemia is defined as a serum immunoglobulin G (IgG) level <2 standard deviations below the age-matched mean.13–15 Holmes et al. found a higher number of febrile episodes in pediatric ALL patients who had at least one IgG level checked (IgG levels <500 mg/dL in 39/63 of these patients) compared with patients who did not have IgG levels checked (5.26 vs. 3.78 episodes/1000 subject-days). 16 However, El-Chennawi et al. found no correlation between IgG levels and the frequency of infectious events during maintenance in ALL patients 3–18 years of age. 9
The incidence and implications of hypogammaglobulinemia in AYA patients receiving intensive chemotherapy for ALL is unknown. We investigated whether hypogammaglobulinemia is associated with an increased number of infections and inferior outcomes in AYA patients receiving chemotherapy per Berlin–Frankfurt–Munster-based Children's Oncology Group (COG) high-risk ALL protocols.17,18
Patients and Methods
Patients
We reviewed electronic medical records of AYA patients diagnosed with B or T cell ALL, between 2008 and 2019, at Riley Hospital for Children in Indianapolis, Indiana. Patients who were <15 years of age at diagnosis, had progressive or refractory disease, received an allogenic stem cell transplant or CAR T cell therapy, or have Down syndrome were excluded. Most patients received induction, consolidation, one or two interim maintenance, and one delayed intensification phases followed by maintenance per established high-risk COG protocols.17,18 Three patients received hyperfractionated cyclophosphamide, vincristine, doxorubicin, and prednisolone (n = 2) or cyclophosphamide, doxorubicin, vincristine, prednisone (n = 1) induction instead of standard induction,12,19 and four patients received St. Jude Rotating Pairs modified maintenance therapy until standard chemotherapy could be tolerated (n = 2) or until the end of treatment (n = 2). 20
Patients were categorized into three groups: (1) those with hypogammaglobulinemia, (2) those without hypogammaglobulinemia, and (3) an unknown group. Hypogammaglobulinemia was defined as having a serum IgG level >2 standard deviations below the age-matched mean (i.e., <639 mg/dL)13,14 at any time during the treatment course. Patients “without hypogammaglobulinemia” were those with IgG level(s) >639 mg/dL. Patients who did not have IgG levels checked were designated as the “unknown group.” IgG levels were obtained per treating oncologist preference, and on suspicion that frequent and/or severe infections may be related to hypogammaglobulinemia. The number of intravenous immunoglobulin (IVIG) doses each patient received were recorded.
Infectious events were defined as follows: (1) any positive blood culture, Clostridium difficile polymerase chain reaction (PCR), plasma viral PCR, or plasma or tissue fungal culture or test; (2) any presumed infection, based on clinical signs or symptoms, such as a(n) upper respiratory infection (URI), lower respiratory infection, or otitis media; and (3) any episode of febrile neutropenia (FN) defined as fever (temperature ≥100.4F) and neutropenia (absolute neutrophil count [ANC] of 500 k/mm3 or less), 4 without a confirmed infection.
Delays in receiving therapy were calculated as the number of days between the date chemotherapy was due and the date chemotherapy was administered. The number of hospital admission days, pediatric intensive care unit (PICU) days, and days requiring ventilator or pressor support were noted for each patient.
Complete blood counts and ANC and absolute lymphocyte count (ALC) were recorded at two time points: (1) at diagnosis and (2) on the date of the lowest documented IgG level before IVIG treatment (for patients with hypogammaglobulinemia) or the date of first IgG level obtained (for patients without hypogammaglobulinemia). Standard cytogenetics and next-generation sequencing (NGS) data were recorded for each patient.
Statistics
Demographic and clinical characteristics were summarized by frequency and percentage for categorical variables, and by median and range or mean ± standard deviation for continuous variables. The groups of patients with and without hypogammaglobulinemia were compared using chi-square tests (or Fisher's exact test, where appropriate) or Wilcoxon two-sample test (or analysis of variance) for categorical and continuous variables, respectively.
Overall survival (OS) and EFS were calculated using Kaplan–Meier methods. OS was calculated from date of diagnosis to date of death. Patients who did not die were censored at their last follow-up visit. EFS was calculated from date of diagnosis to date of recurrence or diagnosis of secondary malignancy. If a patient did not relapse or develop a secondary malignancy, they were censored at date of death or date of last follow-up. A log-rank test was used to compare OS and EFS between patients with and without hypogammaglobulinemia. Statistical significance was set at p = 0.05. SAS version 9.4 (SAS, Institute, Cary, NC) was used for analyses.
Results
Sixty-four patient electronic medical records were reviewed. Fifty-two patients (15–24 years at diagnosis) were included in the analysis (Fig. 1). Demographic characteristics are summarized in Table 1. The majority were male patients (37/52, 71.2%), non-Hispanic white (42/52, 80.8%), and had B cell ALL (39/52, 75.0%). NGS was performed on 7 (17.9%) of the 39 patients with B cell ALL, and Philadelphia chromosome-like (Ph-like) lesions were identified in 4 (57.1%) of these 7 patients, 1 of whom received a Janus kinase inhibitor during treatment. There were also two patients (3.8%) with Philadelphia chromosome-positive (Ph+) ALL, who both received tyrosine kinase inhibitors (Table 1).
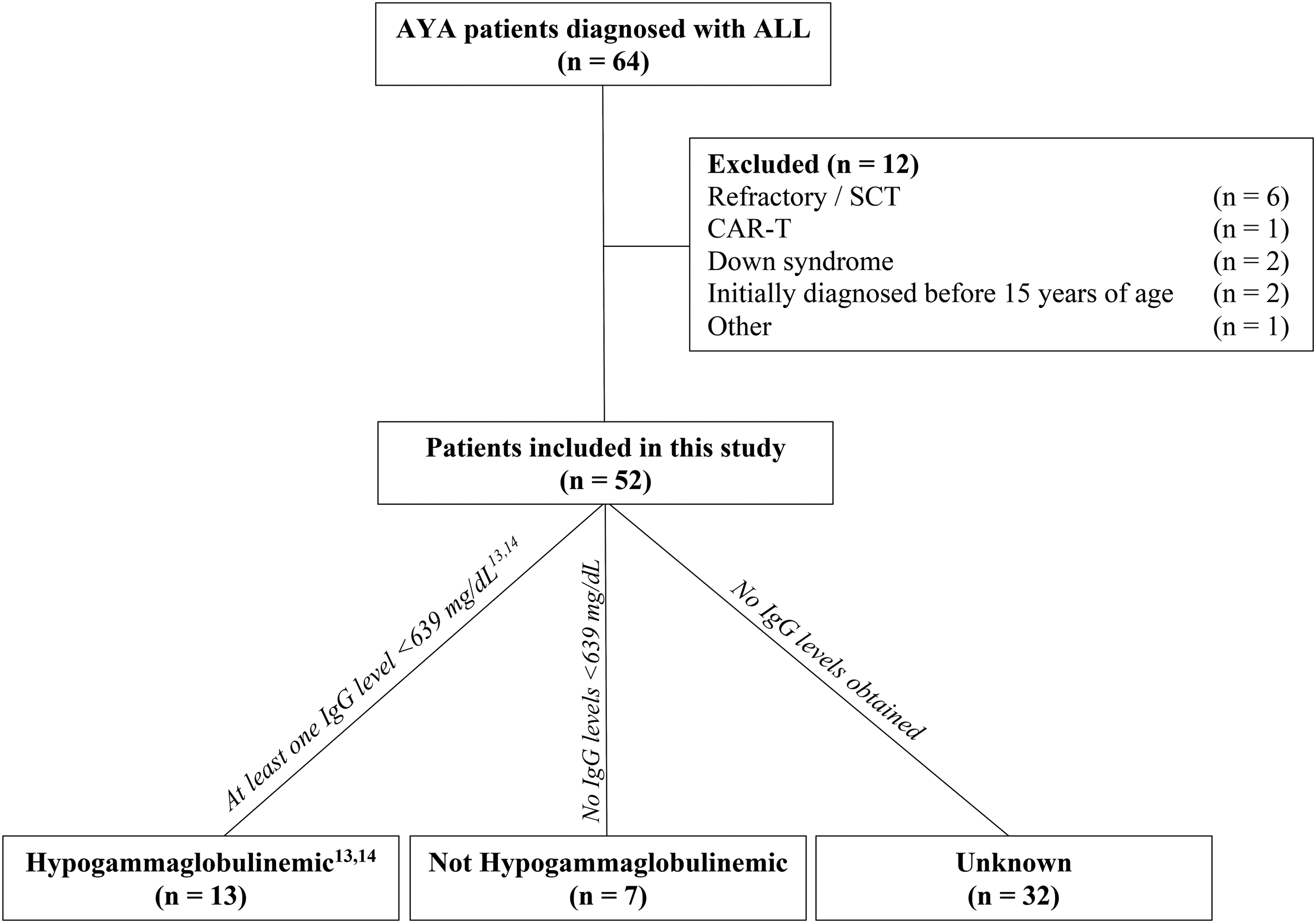
Patient inclusion flowchart. Fifty-two patients met inclusion criteria and were categorized into three groups: hypogammaglobulinemic (n = 13 [25.0%]), not hypogammaglobulinemic (n = 7 [13.5%]), and an unknown group (patients who did not have IgG levels checked, (n = 32 [61.5%]). AYA, adolescents and young adult; CAR-T, chimeric antigen receptor T cell therapy; SCT, stem cell transplant.
Baseline and Clinical Characteristics
Values expressed as n (%), mean ± standard deviation, or median (min, max).
p < 0.05. CBC with differential were obtained for all hypogammaglobulinemic patients at diagnosis and at the time of the lowest IgG level (before the first IVIG treatment, if applicable) (n = 13). Blood counts were available for most patients without hypogammaglobulinemia at diagnosis (n = 5) and at the time of the first IgG level obtained (n = 6). Hypogam, patients with hypogammaglobulinemia; Not hypogam, patients without hypogammaglobulinemia.
ALC, absolute lymphocyte count; ALL, acute lymphoblastic leukemia; ANC, absolute neutrophil count; CBC, complete blood count; Hgb, hemoglobin; IgG, immunoglobulin G; IVIG, intravenous immunoglobulin; Ph+, Philadelphia chromosome positive; PICU, pediatric intensive care unit; Plts, platelet count; WBC, white blood cell count.
Thirteen (25.0%) patients had at least one low IgG level documented (hypogammaglobulinemia), whereas seven (13.5%) had normal IgG level(s) throughout treatment (Table 1). Thirty-two (61.5%) patients did not have IgG levels checked (unknown group, Table 1).
The overall incidence of hypogammaglobulinemia was 65.0% (13/20). Patients with hypogammaglobulinemia were older (median age 18.0 vs. 16.0 years, p = 0.03). There were no significant differences between patients with and without hypogammaglobulinemia with regard to sex, race, or diagnosis (p = 0.1–1.0). The median IgG levels in patients with and without hypogammaglobulinemia were 436 and 862 mg/dL, respectively (p = 0.002). Eleven (84.6%) of the hypogammaglobulinemic patients had low IgG levels that persisted in maintenance therapy. Three of the seven patients without hypogammaglobulinemia (42.8%) also had IgG levels obtained during maintenance, which were within normal limits.
Patients who had IgG level testing performed (n = 20) had a greater total number of infectious events compared with patients who did not have IgG level testing performed (n = 29, median 6.0 vs. 4.0, respectively, p = 0.01). The distribution (types) of infectious complications were similar between these two groups (data not shown). Patients with hypogammaglobulinemia experienced more episodes of FN (median 1.0 vs. 0.0, respectively, p = 0.02) and increased total infectious events (median 9.0 vs. 5.0, respectively, p = 0.06) compared with patients without hypogammaglobulinemia (Table 1). In the 33 patients in this study who had all records of infection available from the date of diagnosis to the end of maintenance, 245 infections were recorded, with 54% (132/245) of these infections occurring during maintenance. Fifty-nine infectious events were recorded during maintenance in nine patients with hypogammaglobulinemia, whereas only 13 infectious events were observed in this phase in five nonhypogammaglobulinemic patients (median 7.0 vs. 3.0, respectively; p = 0.02). The number of hospital admission days, PICU stays, days requiring pressor/intubation support, treatment delays, total white blood cell count (WBC), ANC, ALC, hemoglobin levels, and platelet levels were similar between patients with and without hypogammaglobulinemia (Table 1, p = 0.1–0.9).
The frequency of IgG monitoring and the number and dosages of IVIG received by each patient (Fig. 2) varied owing to provider preference. The majority of patients with hypogammaglobulinemia (76.9% [10/13]) received IVIG supplementation (mean of 4.2 ± 7.5 doses), mostly during maintenance therapy (46/51 doses). Doses of 400 mg/kg (n = 5 [50%]) or higher (n = 5 [50%], up to 1000 mg/kg) were administered per provider discretion. However, only two (20%) of these 10 patients received monthly doses (Patients 2 and 5; Fig. 2). One patient (Patient 2; Fig. 2) did not experience any severe infections requiring hospitalization after instituting monthly IVIG infusions. Patient 5 (Fig. 2) was hospitalized for a viral infection and fungal (P. jiroveci) pneumonia toward the end of maintenance therapy. Eight patients received only one or two IVIG doses although hypogammaglobulinemia persisted in six (75%) of these patients (436.8 ± 109.5 mg/dL). Post-IVIG IgG measurements were obtained in eight patients (range = 7–739 days post-IVIG).
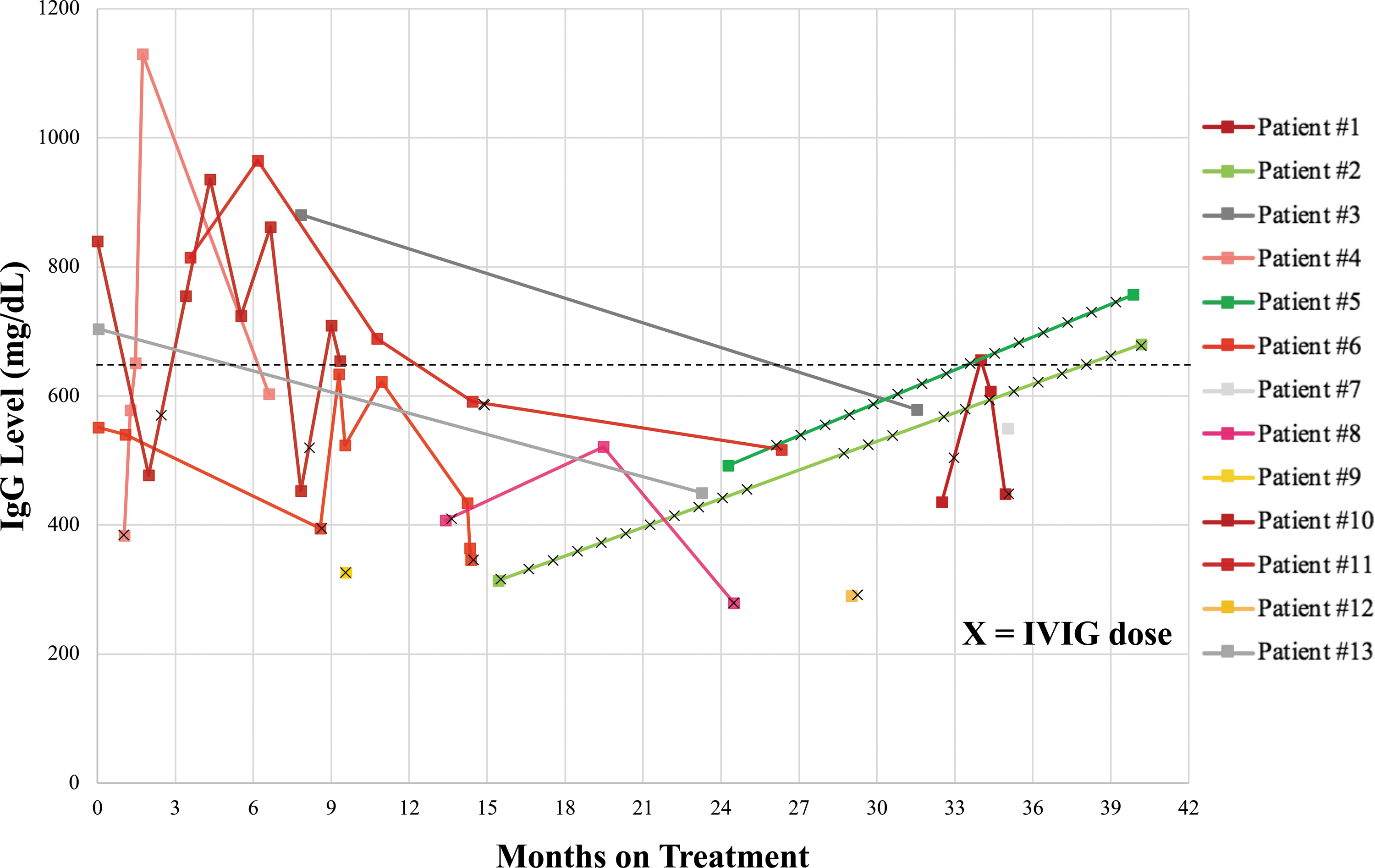
Serum IgG levels in patients during ALL therapy and IVIG replacement over time. IgG levels obtained in 13 hypogammaglobulinemic patients. Each color represents an individual patient. Black Xs represent administered IVIG doses. The dotted, horizontal line represents the lower normal limit of IgG levels (639 mg/dL) in young adults.13,14 Patients 2 and 5 (n = 2) received monthly IVIG. Patients 3, 7, and 13 (n = 3) never received IVIG treatment. Patients 1, 4, 6, 8, 10, and 11 (n = 6) had persistent hypogammaglobulinemia despite IVIG treatment. Patients 9 and 12 (n = 2) did not have IgG levels repeated. Color images available online.
Five patients (9.6%) relapsed (n = 4) or developed a secondary malignancy (n = 1). There was only one recorded death in a patient with unknown hypogammaglobulinemia status. The 5-year OS probability (100% vs. 100%, p = 1.0) and the 5-year EFS probability (84% vs. 100%, p = 0.3) were similar between patients with and without hypogammaglobulinemia.
Discussion
We report that hypogammaglobulinemia occurs frequently in older AYA patients treated on a pediatric ALL protocol (Table 1). Patients who had IgG levels checked by the treating oncologist, suspecting hypogammaglobulinemia, and were found to be hypogammaglobulinemic experienced an increased frequency of FN episodes and total number of infections compared with patients with normal IgG levels (Table 1). The majority of these infections occurred during the less intensive maintenance therapy and were associated with a persistence of hypogammaglobulinemia in these patients. These results are similar to previous reports in pediatric patients.5–7,21
The increased frequency of FN episodes (Table 1) in hypogammaglobulinemic patients is likely because of an increased susceptibility to infection secondary to severe humoral immune dysfunction. Hypogammaglobulinemia was not associated with a lower ALC and ANC or increased frequency of positive blood cultures (Table 1), suggesting that multiple mechanisms, other than bone marrow suppression, may contribute to hypogammaglobulinemia in these patients. It is plausible that low IgG levels could result from an increased protein loss owing to protein-losing enteropathies, proteinuria, or capillary leak. Future studies incorporating simultaneous serum albumin levels, urine protein levels, and measures of immune reconstitution (IgG, IgA, IgM, T and B cell subsets) 9 may help better define additional mechanisms in play.
Previous pediatric and adult studies have demonstrated that IVIG replacement therapy is safe and reduces the number of microbiologically proven infections and antibiotic use.22–24 However, a study in low-risk, pediatric ALL patients found no significant difference in the frequency of febrile episodes, febrile URIs, and positive blood cultures, during maintenance, in patients who received IVIG versus patients who did not. 16 As our data, and the data of others,16,24 suggest, the decisions to obtain IgG levels and order IVIG replacement are often based on institutional guidelines, or provider preference, and are often arbitrary. Furthermore, IVIG treatment is associated with complications (e.g., fever, headache, and nausea/vomiting) in 3%–4% of pediatric ALL patients receiving immunoglobulin replacement therapy.16,23 IVIG supply is often prone to shortages, and is costly. 25 These factors underscore the urgency to establish specific criteria for IVIG use in AYA ALL patients.
The overall and disease-free survival of our patients was excellent. These outcomes, although better than previously published studies, 2 should be interpreted with caution owing to the small number of patients; a low number of T cell patients; incomplete data on NGS, adverse cytogenetics, minimal residual disease; and provider bias related to checking IgG levels and administering IVIG. Future prospective studies systematically documenting IgG levels in AYA ALL patients throughout the treatment course, and aimed at establishing uniform IVIG administration guidelines, are needed to confirm our findings.
Our study raises the important issue of inadequate screening for hypogammaglobulinemia. Thirty-two of the 52 patients (61.5%) in this study never had serum IgG levels measured while on treatment. Our findings highlight the need for improving awareness among AYA oncologists and underscore the need for prospective studies to delineate the overall impact of hypogammaglobulinemia in an expanded AYA patient cohort.
Conclusion
Hypogammaglobulinemia is a common complication of chemotherapy in AYA patients with ALL. Early detection of hypogammaglobulinemia may allow timely administration of IVIG, aimed at preventing infections. Prospective studies in an expanded cohort of AYA ALL patients are needed to establish specific criteria for IVIG replacement in this patient population.
Footnotes
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This institutional review board-approved project was funded, in part, with support from the Short-Term Training Program in Biomedical Sciences Grant funded, in part by T35 HL 110854 from the National Institutes of Health.