
Abstract
Purpose:
This study aimed to: (1) describe the domains and levels of unmet needs of young adult survivors of childhood acute lymphoblastic leukemia (cALL) with comorbidities, and (2) to explore the factors associated with higher levels of unmet needs. Unmet need was considered as supportive care needs not met.
Methods:
The most vulnerable cALL survivors from the PETALE study cohort completed the Short-Form Survivor Unmet Needs Survey, the Brief Pain Inventory and the 15D instrument of health-related quality of life. Demographic and clinical information, including comorbidities, were obtained from medical records or self-reporting. The participants' needs and contributing factors to their needs were evaluated using nonparametric tests.
Results:
Of the 72 participants, 9 (13%) reported moderate/high levels of overall unmet needs. “Worry about earning money” (56%) and “Dealing with feeling tired” (51%) were the most frequent unmet needs (all levels combined). The factors associated significantly with any domain of unmet needs were: having a comorbidity, reporting altered functional health status, high ALL risk status, pain, age (<26 years), and having previously received psychological support.
Conclusion:
A minority of young adult survivors of cALL with comorbidities interviewed reported moderate/high levels of unmet needs. However, financial concerns and emotional health and relationship are the two domains of greatest need. Survivors with altered health condition are most at risk of experiencing moderate/high levels of unmet needs. If confirmed in larger samples, interventions should target modifiable contributors of unmet needs such as physical health and comfort, fatigue, and emotional health.
Introduction
Childhood acute lymphoblastic leukemia (cALL) accounts for nearly one-third of childhood cancers, representing at least 50,000 new cases diagnosed per year worldwide.1,2 Currently, the 5-year survival rate of these patients exceeds 90% in developed countries, where current innovative protocol-driven treatments are available to children.3–5 cALL is one of the most curable cancers. 6 Hence, much current research has focused on late adverse effects resulting in comorbidities, and on survivors' quality of life, to prevent these complications.
Cohort studies of cALL survivors7,8 have ascertained many late adverse effects in this population due to treatment toxicity and radiation exposure.7,9 Survivors frequently have cardiac (e.g., hypertension), metabolic (e.g., diabetes, hypertension), bone (e.g., osteonecrosis), neurocognitive (e.g., attention, memory), and psychosocial complications (e.g., anxiety, depression).7–18 Survivors' health-related quality of life can also be greatly impacted, as highlighted in recent systematic reviews.19,20
These complications may be partially preventable. Indeed, there is reason to believe that nutrition education interventions may favorably impact cardiometabolic comorbidities.21–24 Physical activity can lead to general improvement in the metabolism of patients and to alleviating the adverse effects of treatments, and improve patients' quality of life.25–28 Psychosocial interventions targeting insomnia, psychological distress, and family functioning can also improve patients' quality of life.29–34 However, these interventions are not systematically tailored for this population, and are often not based on a systematic collection of patients' and survivors' needs.
To optimize the specificity of patient care and to achieve patient-centered care,35,36 patients should be interviewed or included in discussions for refining intervention strategies for their difficulties and needs.29,33,37 The assessment of unmet supportive care needs, also termed unmet needs, can help address the gap between survivors' concerns and the level of assistance provided, which is central to formulating a supportive care strategy.38,39 Supportive care is defined as a person-centered approach to “the provision of the necessary services for those living with or affected by cancer to meet their informational, spiritual, emotional, social, or physical needs during diagnosis, treatment, or follow-up phases, including issues of health promotion and prevention, survivorship, palliation, and bereavement”.40 (p. 374)
Unmet needs have been classified into 11 primary domains: physical, psychosocial/emotional, family-related, social, interpersonal/intimacy, practical, daily living, spiritual/existential, health system/information, patient–clinician communication, and cognitive.40,41 Collecting information on these survivors' needs may be key to offering appropriate targeted services in clinics.38,42 Importantly, we still have very limited knowledge on the needs of the vulnerable population of cALL survivors.43,44
Thus, our objectives were: (1) to describe the domains and levels of unmet needs in cALL young adult survivors presenting cardiac, metabolic, neurocognitive, psychological, or bone comorbidities, and (2) to explore whether these needs were explained by health status, demographics, or clinical history.
Methods
This analysis was part of the PETALE study, a multidisciplinary research project conducted at Sainte-Justine University Health Center (SJUHC, Montreal, Canada). The PETALE study aimed to comprehensively characterize late adverse effects and to identify the associated predictive biomarkers of long-term treatment-related complications in cALL survivors. The study was divided into two phases of recruitment, with the second phase recalling survivors who presented extreme phenotypes (late effects) in the first screening phase. 45 For the present study, we focused on participants included in Phase II, who are the most vulnerable survivors of the cohort (details provided below) and conducted a cross-sectional analysis of the survey performed on this subgroup of cALL survivors.
Participants
In Phase I, cALL survivors diagnosed between 1987 and 2010 before the age of 19 years, treated according to Dana-Farber Cancer Institute/ALL Consortium protocols 87-01 to 05-01, 46 ≥5 years from diagnosis with no recurrence, who spoke French or English, and were able to complete self-rated questionnaires were invited to take part in the study. Patients who received a hematopoietic stem cell transplant or who experienced recurrence were excluded.
Participants eligible for Phase II study were cALL young adult survivors with extreme phenotypes in at least one of the following domains: cardiopulmonary, metabolic, bone, psychosocial, or neurocognitive. We only included survivors ≥19 years of age. For example, if their measures of anxiety, depression, or distress taken during Phase I exceeded the cut-points for clinical levels, they were invited to complete the Phase II investigations. Consequently, the Phase II sample is composed of the most vulnerable participants of the PETALE study. The full details on the study design and inclusion criteria for Phase II are available in Marcoux et al. 45
Procedure
Participants and their parents (if appropriate) were met between April 2014 and December 2016. The participants who agreed to take part in the study came to the hospital for a day of testing. The tests included complete biological measures, physical health examination, and psychosocial questionnaires. The questionnaires were completed at the hospital or at home, with a mail-back envelope to be sent within 3 weeks.
The Ethics Review Committee of SJUHC approved the study protocol (#2013-479, 3607) and it was conducted in accordance with the Declaration of Helsink. Written informed consent was obtained from all participants.
Measures
Demographic and clinical variables
Participant age, sex, ethnicity, marital status, family structure, educational background, and professional status were self-reported. Time since diagnosis, overall clinical history, including treatments, and information about whether they had received psychological support were collected from the patients' medical files.
Comorbidities
For all Phase II participants, we also collected comorbidities clinically. The clinical director of the long-term follow-up clinic rated these as present or absent based on the medical files and clinical exams available at the assessment point using the Common Terminology Criteria for Adverse Events (CTCAE) version 4.03. 47 No rating was available for psychological morbidity, as no systematic assessment of psychosocial distress was performed at the institution at the time of data collection. A morbidity in one domain was considered present if the domain required in-depth investigation or treatment. Examples of morbidities are: mineral density deficits or osteoporosis (bone), valvular abnormalities or ventricular arrhythmia (cardiac), attention or concentration deficits (neurocognitive), hyperlipidemia, or type 2 diabetes (metabolic). This rating was made available for further analysis in the case report form.
Unmet needs
The participants' unmet needs were assessed using the Short-Form Survivor Unmet Needs Survey (SF-SUNS). 48 We adapted the questionnaire into French following standard translation procedures. 49 The 30-item questionnaire assesses four unmet need domains divided into four factors: (1) information (3 items; α = 0.67), (2) financial concerns (8 items; α = 0.84), (3) access and continuity of care (6 items; α = 0.90), and (4) emotional health and relationship (13 items; α = 0.93). Each domain is scored 0–4, with higher scores indicating high levels of unmet needs. Scores of 0 were classified as no unmet needs, 0–1 as low unmet needs, 1–2 as low-to-moderate unmet needs, and 3–4 as high unmet needs. 50
Functional health status
The French version of the 15D instrument of health-related quality of life (http://15d-instrument.net/15d/) 51 was used to measure functional health status at study Phase I (1.25 ± 0.60 years before Phase II) across 15 domains (α = 0.82): mobility, vision, hearing, breathing, sleeping, eating, speech, excretion, usual activities, mental function, discomfort and symptoms, depression, distress, vitality, and sexual activity. A single index score is obtained, ranging from 0 (being dead) to 1 (no problem in any dimension).
Clinical pain
The French version of the Brief Pain Inventory (BPI)52,53 was used to measure both pain severity (four items; α = 0.87) and pain interference (seven items; α = 0.93). Pain severity was measured at its worst, least, average, and current level. The level of functional interference caused by pain was measured with items assessing general activity, walking, work, mood, sleep, enjoyment of life, and relations with others. Scores of 1–4 were classified as mild pain, 4–7 as moderate pain, and 7–10 as severe pain. 54
Statistical analyses
The Statistical Package for the Social Sciences (SPSS, version 25) was used to conduct statistical analyses. First, we conducted descriptive analyses on the different measures to confirm suitability for parametric tests (data normality and homogeneity when applicable). Then, for Objective 1, we computed means, standard deviations, and frequencies for each factor and item of the SF-SUNS, and described the most frequent needs expressed. For Objective 2, nonparametric tests were performed. Mann–Whitney U tests were used to explore whether unmet needs were linked to comorbidities, demographic and clinical characteristics. Considering possible multimorbidity, we analyzed the links between unmet needs and the number of combined comorbidities with Spearman correlations. We also computed Spearman correlation tests to investigate the associations between unmet needs (SF-SUNS), clinical pain (BPI), and functional health status (15D).
Results
Participants characteristics
A total of 247 eligible cALL survivors were recruited in the PETALE Phase I study. From Phase II, 219 cALL survivors were eligible, among whom 72 young adults (≥19 years) composed the present study sample (flow chart in Appendix Fig. A1). The participants were 19–42 years of age (mean age, 27 ± 6 years), with a majority of self-reported Caucasian ethnicity (96%). The mean time since diagnosis was 17 ± 6 years. Most participants had been treated with cranial radiotherapy (81%; maximum dose was less than or equal to 19 Gy) and approximately one-quarter had received support from a mental health specialist.
Most participants had at least one clinically significant comorbidity (n = 56; 78%) according to the CTCAE rating: either one from among bone, metabolic, or neurocognitive (n = 30; 54%) or a combination of bone, metabolic, neurocognitive, or cardiac complications (n = 26; 46%). As summarized in Figure 1, the cardiac domain was always combined with another domain (metabolic, bone, or neurocognitive). The most frequent morbidity domain alone was metabolic complications (56%). On average, the participants had 1.30 ± 1.00 comorbidity.
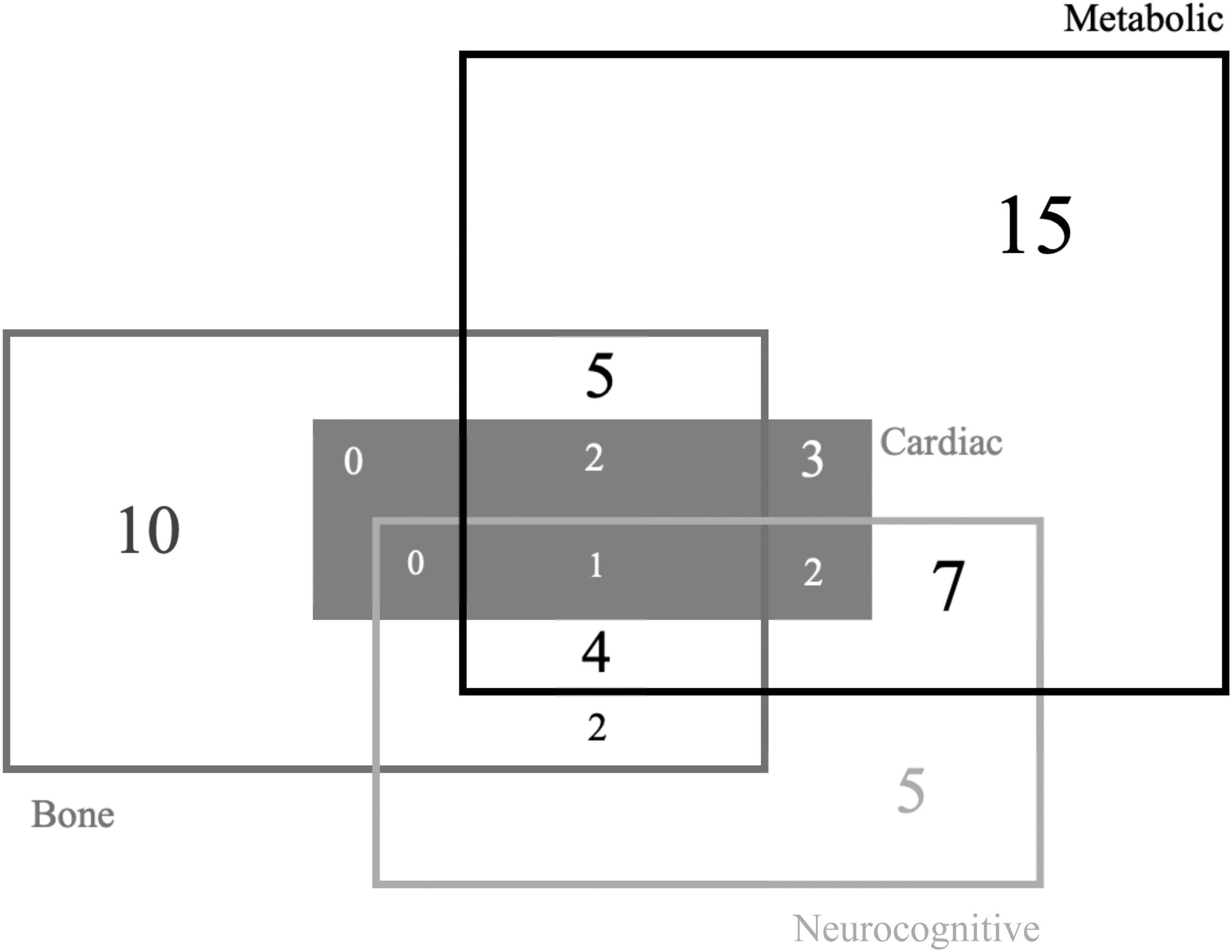
Co-occurrences of clinically rated comorbidities in adults from PETALE Phase II study (n = 56 childhood acute lymphoblastic leukemia survivors from the PETALE study).
However, participants with neurocognitive complications were younger at diagnosis than participants without such complications (6.31 ± 4.25 years vs. 10.67 ± 4.92 years, U = 274.00, p < 0.01). More specifically, patients who had radiotherapy and presented neurocognitive complications were younger at diagnosis than participants without such complications (6.60 ± 4.37 years vs. 11.44 ± 4.67 years, U = 170.00, p < 0.01). No such statistical differences were observed for metabolic, bone, or cardiac complications according to age at diagnosis (Appendix Table A1). Furthermore, the participants reported only mild levels of pain severity (1.71 ± 1.85 on the 0–10 scale) and pain interference (1.17 ± 1.78 on the 0–10 scale) as measured with the BPI, and very good overall functional health status (0.92 ± 0.08 on the 0–1 scale; 15D instrument).
Table 1 lists the complete details of the participants' characteristics and present the differences between the participants included in PETALE study Phase I and Phase II.
PETALE Study Phase I and II (n = 247 and 72) Participants' Demographic and Clinical Characteristics
Statistical differences between participants phase I and II were computed with Pearson's chi-square test or Fisher's exact test for categorical variables and with Student's t-test for numerical variables.
ALL, acute lymphoblastic leukemia; DFCI, Dana Farber Cancer Institute; SD, standard deviation.
Description of unmet needs
Most of the participants had no unmet needs (19%) or low unmet need levels (68%) (Table 2). The mean levels of unmet needs were also very low (<0.60) for all domains. When present, unmet needs were more frequently reported in the emotional health and relationship domain.
Levels of Unmet Needs Per Domain on the Short-Form Survivor Unmet Needs Survey (n = 72 Childhood Acute Lymphoblastic Leukemia Survivors from the PETALE Study)
However, when investigating the responses for each item (Fig. 2), we observed that >40% of the participants rated five items as an unmet need, and >20% of participants rated 15 items as an unmet need. Thus, some items appeared more representative of unmet needs in the present sample. Participants frequently reported being “Worried about earning money” (item 4; 55.56%) and expressed concerns about “Paying household bills or other payments” (item 6; 43.06%), highlighting financial concerns. Other needs were linked to emotions, such as “Dealing with feeling tired” (item 24; 51.39%), “Dealing with feeling stressed” (item 25; 48.61%) and “Dealing with changes in how my body appears” (item 29; 47.22%). Information, access, and continuity of care were the domains with the fewest unmet needs for all items (reported by <20% of the participants) (Fig. 2).
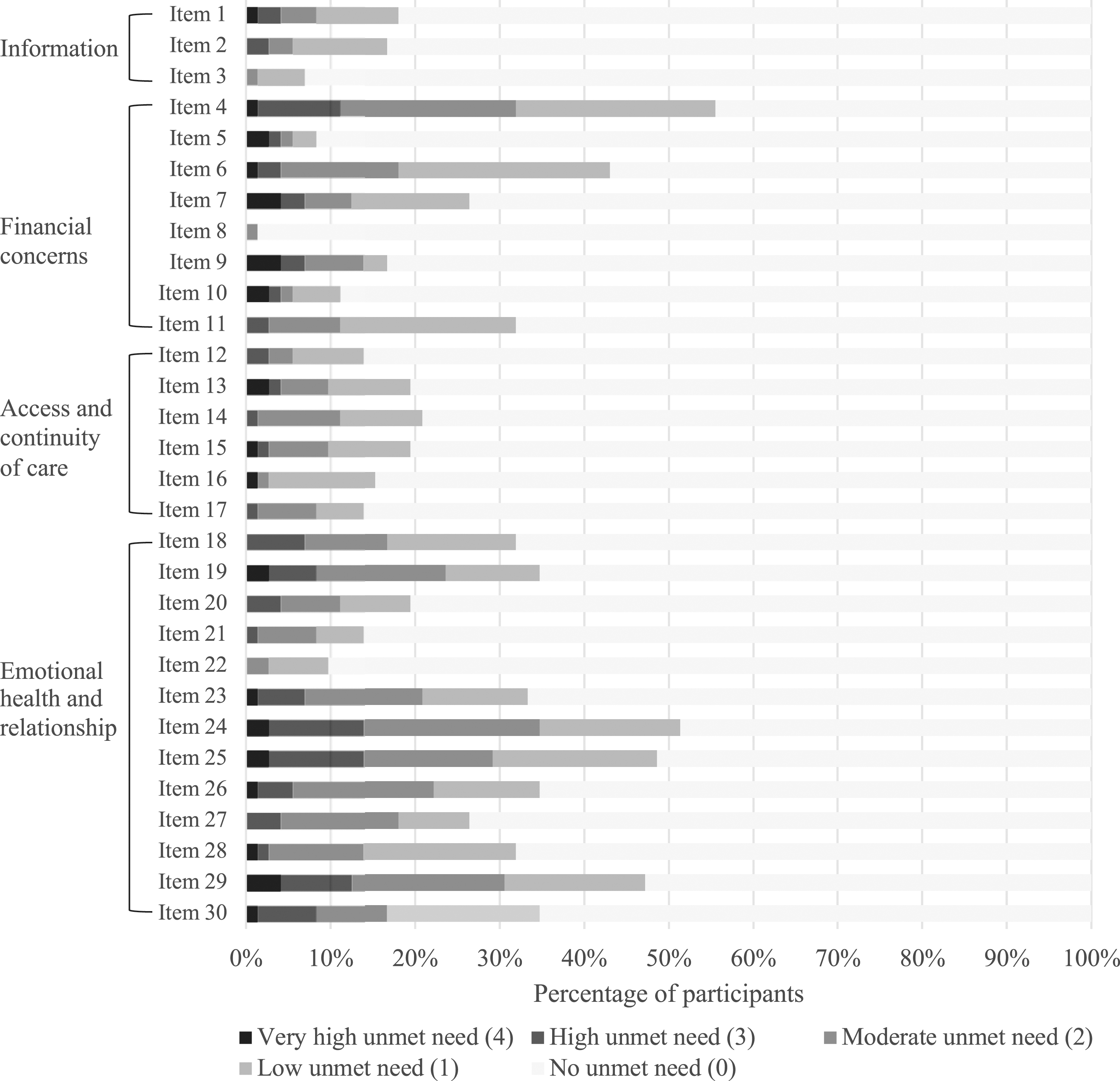
Levels of unmet needs per item on the SF-SUNS (n = 72 cALL survivors from the PETALE study). Items labels' 48 : item #1: Finding information about complementary or alternative therapies; item #2: Dealing with fears about cancer spreading; item #3: Dealing with worry about whether the treatment has worked; item #4: Worry about earning money; item #5: Having to take a pension or disability allowance; item #6: Paying household bills or other payments; item #7: Finding what type of financial assistance is available and how to obtain it; item #8: Finding car parking that I can afford at the hospital or clinic; item #9: Understanding what is covered by my medical insurance or benefits; item #10: Knowing how much time I would need away from work; item #11: Doing work around the house (cooking, cleaning, home repairs etc.); item #12: Having access to cancer services close to my home; item #13: Getting appointments with specialists quickly enough (oncologist, surgeon, etc.); item #14: Getting test results quickly enough; item #15: Having access to care from other health specialists (e.g., dieticians, physiotherapists, occupational therapists); item #16: Making sure I had enough time to ask my doctor or nurse questions; item #17: Getting the health care team to attend promptly to my physical needs; item #18: Telling others how I was feeling emotionally; item #19: Finding someone to talk to who understands and has been through a similar experience; item #20: Dealing with people who expect me to be “back to normal”; item #21: Dealing with people accepting that having cancer has changed me as a person; item #22: Dealing with reduced support from others when treatment has ended; item #23: Dealing with feeling depressed; item #24: Dealing with feeling tired; item #25: Dealing with feeling stressed; item #26: Dealing with feeling lonely; item #27: Dealing with not being able to feel “normal”; item #28: Trying to stay positive; item #29: Coping with having a bad memory or lack of focus; item #30: Dealing with changes in how my body appears. SF-SUNS, Short-Form Survivor Unmet Needs Survey.
When exploring the associations among the domains of unmet needs, we found moderate–strong positive and significant correlations between all domains. The emotional health and relationship domain was strongly associated with both the financial concerns and information domains (r = 0.64, p < 0.01; r = 0.44, p < 0.01, respectively) and was moderately associated with the access and continuity of care domain (r = 0.33, p < 0.01). The access and continuity of care domain was also strongly associated with the financial concerns and information domains (r = 0.47, p < 0.01; r = 0.43, p < 0.01, respectively). We found a strong correlation between the financial concerns and information domains (r = 0.40, p < 0.01).
Contributing factors of unmet needs
Comorbidities
We explored the distribution of unmet needs across the domains of deteriorated health (Appendix Table A2). Participants with neurocognitive issues had higher levels of information (p < 0.05) and emotional health and relationship unmet needs (p < 0.05) than participants without neurocognitive late adverse effects. Participants with bone late adverse effects had higher levels of access and continuity of care (p < 0.05) unmet needs than participants without bone complications. We found no difference for metabolic and cardiac comorbidities.
When examining the number of unmet needs according to the number of comorbidities, we observed that more frequent comorbidities were accompanied by higher levels of unmet needs. This was particularly true for access and continuity of care (r = 0.26, p < 0.05) (Fig. 3).
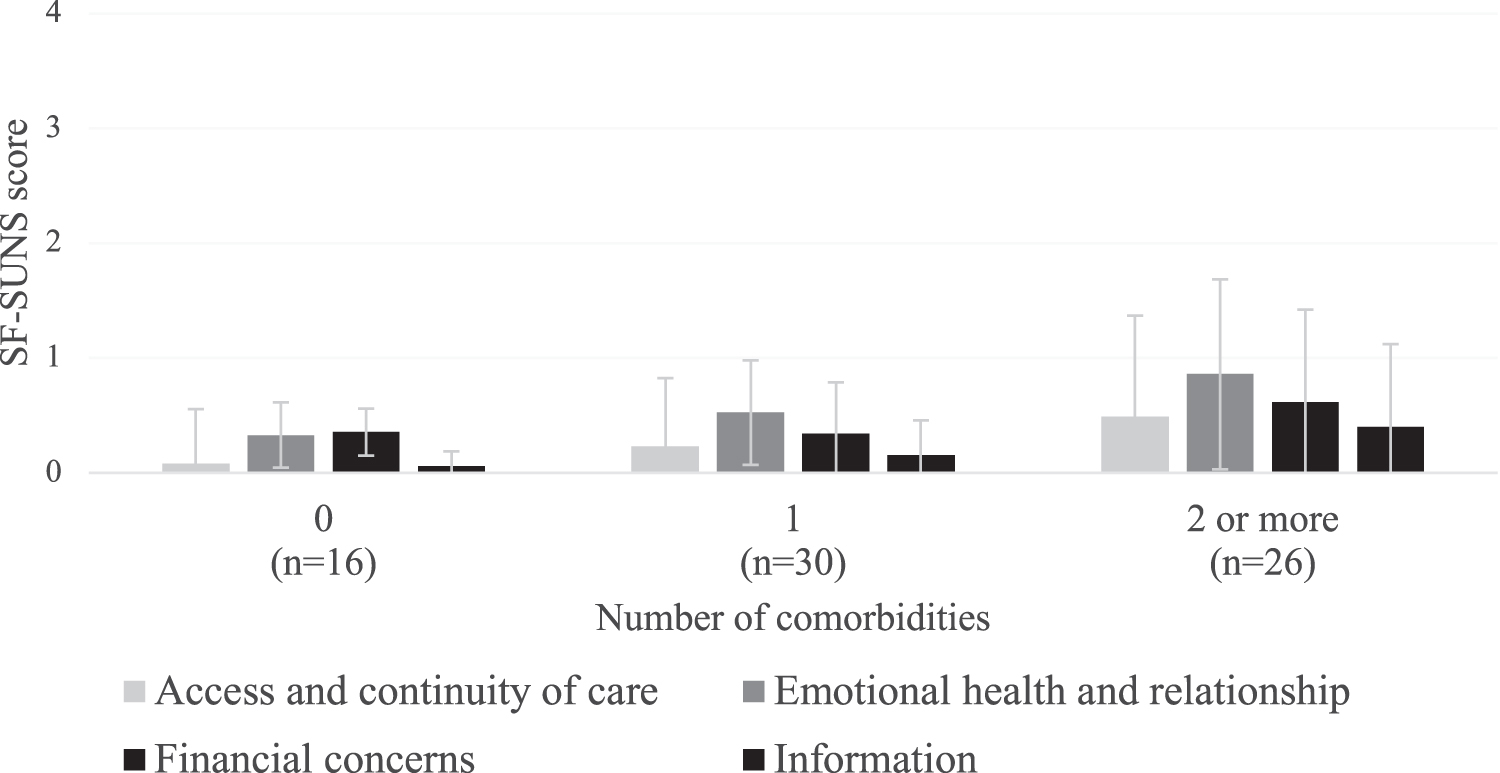
Mean levels of unmet needs according to the number of comorbidities (n = 72 cALL survivors from the PETALE study). Among all the participants, 16 participants had no comorbidity, 30 had one among metabolic, bone, or neurocognitive, 26 had two to four comorbidities (error bars represent the standard deviation of the dataset).
To control for multiple comorbidities, we removed participants presenting mixed profiles (n = 26, Fig. 1), and explored the level of unmet needs across the remaining three groups presenting only one comorbidity, that is, metabolic (n = 15), bone (n = 10), or neurocognitive (n = 5). The results suggested that participants with metabolic complications had fewer unmet needs (all domains) than participants with bone or neurocognitive complications, but these apparent differences did not reach significance in this limited sample (p > 0.05) (Appendix Table A3).
Functional health status and clinical pain
All domains of unmet needs were associated with functional health status and clinical pain (except for the financial concerns domain unrelated with clinical pain). Functional health status measured in Phase I was significantly and negatively associated with unmet needs (all domains). For example, worse functional health status was associated with more information needs and financial concerns (r = −0.32, p < 0.05; r = −0.25, p < 0.05, respectively). Unmet needs were also significantly and positively associated with pain interference (information, access and continuity of care, and emotional health and relationship domains) and pain severity (access and continuity of care, emotional health and relationship domains). Higher pain was associated with more frequent unmet needs. The complete results are available in Appendix Table A4.
Demographic and clinical factors
We also found that unmet needs were associated with younger age, previous psychological support received, and higher ALL risk status. Financial concerns were more frequent among participants <26 years of age and those who had received psychological support (p < 0.05 and p < 0.01, respectively). Participants who had received psychological support expressed more emotional health and relationship needs (p < 0.05). Participants with high ALL risk status reported access and continuity of care needs more frequently compared with those with standard risk (p < 0.05). No significant association was found with sex, marital status, having children, time since diagnosis and radiotherapy received (Appendix Table A2).
Discussion
This study is the first to investigate the unmet supportive care needs of cALL young adult survivors and their contributing factors. The cALL survivors interviewed expressed few unmet needs. However, the most frequently expressed needs were related to the emotional health and relationship, and financial domains. The factors contributing to unmet needs, depending on the domain, were late adverse effect, altered functional health, pain, having received psychological support in the past, and being younger than 26 years old. Health care professionals could use this information to quickly identify and assist those in need.
Twelve percent of our participants expressed moderate-to-high levels of unmet needs. This result is consistent with the literature, where the levels of unmet needs among survivors of hematologic cancer are generally low.55–58 A study conducted specifically on survivors of pediatric cancers, however, showed high levels of unmet needs. These needs were higher among leukemia cancer survivors compared with survivors of solid tumors. 44 The differences found between our study and other studies can be linked to the country health care system and long-term care available. In Canada, universal health care exists. Our results are thus generalizable to countries with such health care system.
However, even if our participants tended to express few unmet needs, more than 40% of them reported specific needs related to dealing with feeling stressed or tired, dealing with changed body, and worrying about earning money and paying household bills or other payments. Indeed, psychological and information needs have been identified as the most frequent needs among adult cancer survivors, and physical and daily living concerns are the most frequent among adult hematological cancer survivors. 59 Thus, cALL survivors seem to have similar unmet needs to other cancer survivors.
Yet, among the unmet need domains identified in the literature, specific to cancer survivors 60 or not,40,41 an important one has not been explored in our study, i.e., intimacy and sexuality. It appears particularly important to explore this domain among cALL survivors, as recent studies have reported that intimacy and sexuality are strongly impacted.61–63 This is even more obvious at an age when the child, adolescent, or young adult is in the process of building their identity and exploring intimate relationships with others.64,65 In addition, childhood leukemia cancer survivors have fewer higher education and occupational achievements. 66 Future qualitative studies may be particularly relevant for exploring a person's needs in these domains. Moreover, to our knowledge, no study explored unmet needs among other pediatric populations in a similar manner. Further studies should explore unmet needs in other oncologic and nononcologic chronic childhood conditions to explore whether these needs can be condition or age related.
The participants of the present study were specifically selected based on health criteria. In this group, we found that the following factors related to their condition were associated with unmet needs: clinical comorbidities, functional health status, and pain. Participants presenting several comorbidities expressed moderate/high needs for information and access and continuity of care. More specifically, the presence of neurocognitive morbidity was significantly associated with information and emotional health and relationship needs. Likewise, bone morbidities were associated with the need for access and continuity of care. A systematic review of adult cancer survivors found that comorbidities, symptoms, and quality of life were associated with higher levels of unmet needs. 59
In the present study, younger age was also associated with unmet needs. Participants younger than 26 years of age reported more financial concerns than the older, highlighting an issue that may be specific to cALL survivors, as financial concerns are less prevalent in adult survivors of hematological cancers.55–58 This is probably the result of higher financial strain on pediatric cancer survivors resulting from their younger age and the responsibilities that accompany young adulthood.
We should acknowledge several limitations of this study. First, the limited sample size did not allow us to carry out multivariate analyses that would have allowed us to isolate the unique effects of the contributing factors. As Figure 1 illustrates, a detailed description of the participants' clinical context quickly yields small cell numbers. Second, 96% of our participants were Caucasians. Thus, the results are not generalizable to all ethnic groups. Third, although we based our analysis on a recognized questionnaire of unmet needs, our data potentially overlooked some aspects of cALL survivors' unmet needs (e.g., intimacy/sexuality). To ensure appropriate and targeted care, future research should continue exploring cALL survivors' needs in larger samples, using surveys specifically developed for the younger adult population. Researchers should also consider conducting further studies in more varied samples.
In conclusion, in a group of 72 vulnerable cALL survivors, the most frequent unmet needs were related to financial concerns and emotional aspects. The levels of unmet needs were related to the presence of clinical comorbidity, lower functional status, pain, as well as younger age and higher risk status. The results stress the complexity of distinguishing and studying different groups of participants based on their clinical profiles, as multimorbidity is frequent. Future research should expand this line of research by improving profiling methods in larger samples and specifying the needs surveyed in childhood cancer survivors to better describe the needs of young adult survivors, as most tools have been developed for the much older adult populations.
Footnotes
Acknowledgments
The authors would like to thank all the survivors who participated in the study, and the clinical research staff.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Institute of Cancer Research of the Canadian Institutes of Health Research, in collaboration with C17 Council, Canadian Cancer Society, Cancer Research Society, Garron Family Cancer Center at the Hospital for Sick Children, Ontario Institute for Cancer Research, Fonds de Recherche du Québec-Santé Cancer Grant, and Pediatric Oncology Group of Ontario grant number TCF 118694. Editorial assistance in English was financed by the Laboratory of Psychopathology and Health Processes, Université de Paris.
Appendix
Association Between Unmet Needs, Pain, and Functional Status
| Measures | BPI pain severity (n = 68) | BPI pain interference (n = 68) | Functional status 15D (n = 66) |
|---|---|---|---|
| Domains of unmet needs | |||
| Information | 0.22 | 0.41 * | −0.32 * |
| Financial concerns | 0.17 | 0.24 | −0.25 * |
| Access and continuity of care | 0.30 * | 0.43** | −0.34** |
| Emotional health and relationship | 0.24 * | 0.37** | −0.47** |
| Mean (SD) | 1.71 (1.85) | 1.17 (1.78) | 0.92 (0.08) |
| Scope | 0–6.5 | 0–7.29 | 0.68–1 |
p < 0.05; **p < 0.01.
15D, instrument of health-related quality of life; BPI, brief pain inventory.