
Abstract
Activity trackers have emerged as promising devices used to motivate and/or objectively monitor physical activity (PA) levels. It is unknown how activity trackers have been used in interventions for children and adolescents affected by cancer. This review aimed to investigate the effectiveness of wearable activity trackers to monitor and/or improve PA levels and health outcomes in pediatric oncology. Based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses, we conducted an electronic search of four databases (Cumulative Index to Nursing and Allied Health Literature [CINAHL], Medline, Embase, and SportDiscus) between January 2000 and March 2020. The review included PA interventions that used an activity tracker with children (≤18 years) diagnosed with cancer. We excluded studies including adult participants (>18 at time of study participation) and cross-sectional or case-report studies. Twelve studies examining 517 children and adolescent patients and survivors of pediatric cancer (age range: 4–18 years) were included. Intervention delivery ranged from 2 weeks to 12 months. Two of 12 studies reported increases in PA and 6 showed improvements in health outcomes, including aerobic fitness and negative mood. PA interventions using activity trackers within pediatric oncology are highly diverse in study design, study population, and intervention features. Preliminary data suggest that interventions using wearable activity trackers may have a positive impact on health outcomes in children and adolescents affected by cancer. Future research is needed to establish optimal intervention approaches to using activity trackers to increase PA in children affected by cancer.
Introduction
Cancer is the leading cause of death for children worldwide with ∼300,000 young people 0–19 years of age diagnosed each year. 1 Childhood cancer survival rates have increased in the last 50 years to currently over 80% due to advancements in cancer treatment and improved patient care.2,3 Despite this success, childhood cancer survivors are at risk of developing treatment-related long-term health conditions, including cardiovascular disease, secondary cancers, metabolic syndrome, endocrine dysfunction, neurological deficits, and decline in fitness and muscle strength. 4
Many survivors experience a decline in physical activity (PA) levels coupled with poor dietary practices. 5 These modifiable risk factors for cardiometabolic disease may contribute to a decline in health-related quality of life (HRQOL) over time. 6 The consequence of poor lifestyle behaviors may increase survivors' already elevated risk for cardiometabolic diseases and secondary cancers. 7 Given their increased risk of chronic health conditions, sedentary behavior in survivors is particularly concerning.
PA has been shown to be safe and effective before, during, and following cancer treatment, to reduce the adverse physical and psychological burden of cancer.8,9 Participation in PA attenuates cancer-related fatigue and improves cardiorespiratory fitness, muscle strength, body composition, and HRQOL in adult patients during treatment and in adult survivors.10–12
However, over two-thirds of survivors do not meet the recommended guidelines and are not as active as their healthy peers, despite their increased risk for associated chronic conditions. 13 Recommended guidelines for children (5–11 years) and adolescents (12–17 years) include at least 60 minutes moderate-vigorous intensity PA daily. 14 PA should be age appropriate and be encouraged through unstructured play or recreational games for children, or structured exercise for adolescents, while team sports can be appropriate across both groups.14,15 Based on the promising evidence of the benefits of exercise in adults,16,17 it is essential to increase PA levels in both childhood cancer patients and survivors.
PA interventions, if incorporated during cancer treatment or in survivorship, have the potential to increase cardiorespiratory fitness, improve musculoskeletal function, and reduce the risk of long-term health complications.18,19 However, access to exercise oncology services is often difficult for several families, given the paucity of pediatric oncology treating centers in many countries. 20 The scarcity of hospitals creates several issues for families such as additional costs (including transport, accommodation, and care for siblings of children with cancer), loss of income, and the need to travel long distances to receive specialized care.20,21 Health innovations such as online services have been therefore adopted by researchers and clinicians to monitor, engage, and motivate patients to improve supportive care accessibility and minimize the burden of travel. 22
Activity trackers or accelerometers that do not provide feedback to the user (e.g., Actigraph GT3X) can allow practitioners to monitor PA intensity, duration, energy expenditure, sleep, and time spent in sedentary behaviors,23,24 without being affected by human error or self-report bias. Activity trackers that do provide feedback to the user (e.g., Fitbit) can also assist in increasing PA levels through self-monitoring of behaviors, setting step count or activity goals, and encouraging reduced sedentary behaviors. 25
Activity trackers integrated into PA interventions as behavior change tools can be promising motivators to increase PA levels and decrease health-related risks in the general population 26 ; however, understanding of the effectiveness of wearable activity trackers for children diagnosed with cancer remains limited. A recent review also found PA interventions delivered remotely appear to be feasible for adult survivors of childhood cancer. 27 Despite the feasibility of wearing activity trackers, there is still a lack of understanding of how these tools are used to monitor, increase, and sustain PA levels in children and adolescents.
Engaging children and adolescents affected by cancer in PA may be more difficult than engaging adults due to their unique challenges and unmet needs such as their early confrontation with mortality, increased dependency on parents/carers, and disruptions to school, work, and social life.28,29 Assessing the use of wearable activity trackers in measuring and/or promoting PA levels is necessary to develop successful interventions that improve health behaviors. A systematic review is needed to provide an overview of current wearable activity tracker technology, how they are used in the interventions for children with cancer, and their effectiveness in changing behavior and health outcomes.
This study is, to our knowledge, the first to systematically review the effectiveness of wearable activity trackers (including trackers that provide user feedback and those that do not) to measure and improve PA outcomes (e.g., steps per day and moderate to vigorous physical activity [MVPA]) and other health outcomes in child cancer patients and survivors. The secondary aim is to identify common features (e.g., health professional contact and peer support) among interventions that achieve improvements in PA and other health outcomes, including fitness and quality of life.
Methods
Search methods/identification of studies
This systematic review was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement. 30 A summary of the screening and data extraction process, including reasons for exclusion, is provided in Figure 1. We searched four databases (Cumulative Index to Nursing and Allied Health Literature [CINAHL], Medline, Embase, and SportDiscus) and Google Scholar using the following search terms: (child* or adolescent or pe?diatric or surviv* or kid* or teen* or adult) AND (cancer* or oncology or neoplasm or tumo?r) AND (pedometer* or activity tracker or fitness tracker or activity monitor or fitbit or accelerometer or actigraphy or distance) (Supplementary Table S1). The review included published articles from January 2000 to March 2020. We selected a start date of January 2000 to reflect when digital activity trackers became more widely available.31–33
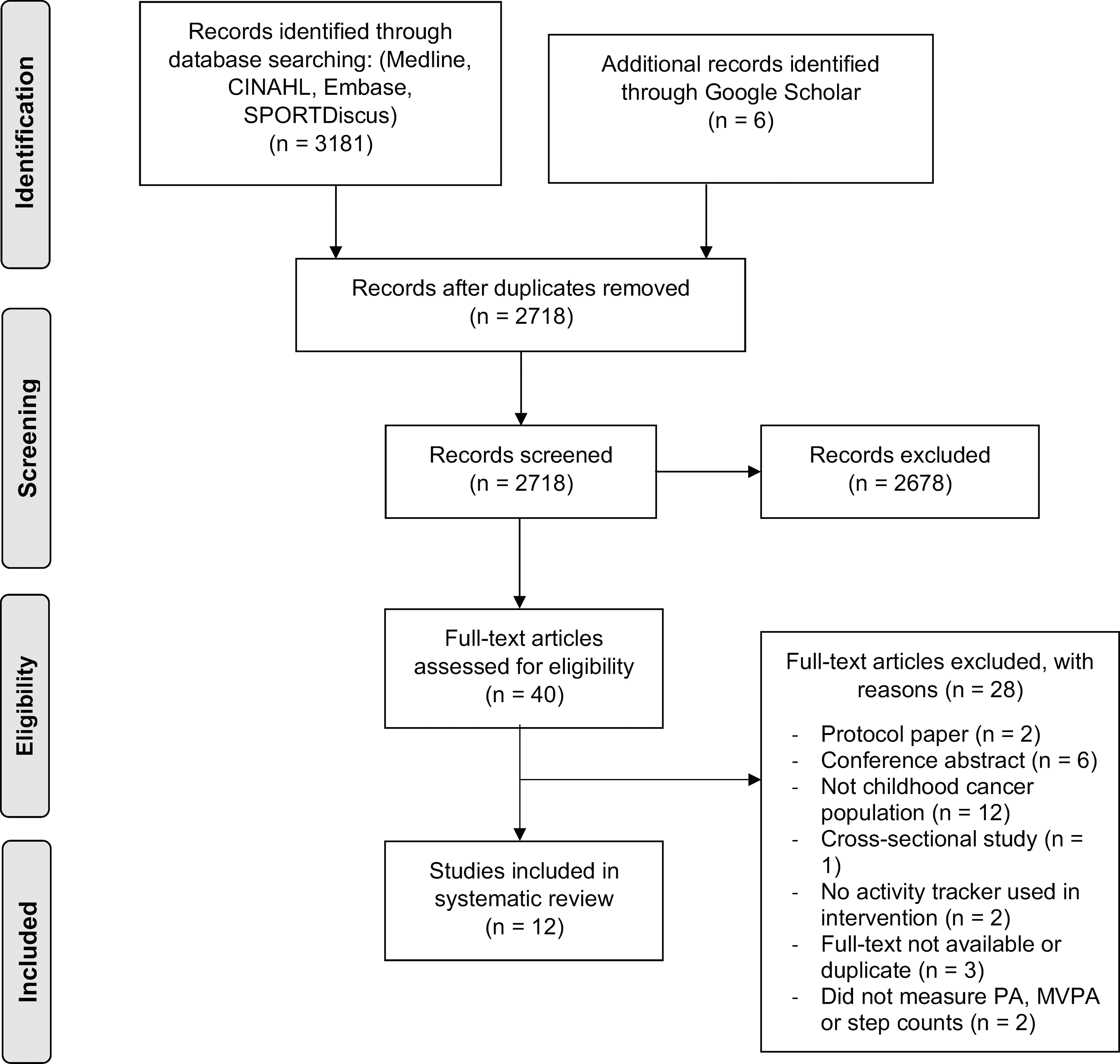
Flow diagram for study selection and reasons for exclusion. CINAHL, Cumulative Index to Nursing and Allied Health Literature; MVPA, moderate to vigorous physical activity; PA, physical activity.
Inclusion/exclusion criteria
This review was restricted to studies published in English. Articles were eligible if participants were (1) diagnosed with childhood cancer at ≤18 years of age and were ≤18 years of age at the time of the study, (2) undergoing or had completed any oncology treatment regimen (receiving maintenance chemotherapy was included), and (3) receiving an intervention incorporating any type of wearable activity tracker to provide quantitative assessment of PA levels (non-feedback; defined as step count or MVPA) or used as a behavioral change tool (with feedback). Articles were excluded if participants were adults (i.e., older than 18 years at time of study participation). Interventions including both children and adults were excluded if the mean age of the participant sample was >18 years. Cross-sectional or case report studies and studies that did not measure PA as an outcome measure were also excluded.
Screening and extraction
Two reviewers (L.H. and D.M.) independently screened 2718 abstracts after removal of duplications and screening reference lists of included articles. Consistency between reviewers was high (97.2% agreement). Any discrepancy was discussed and resolved with a third reviewer (C.S.). Forty articles were eligible for full-text screening. After full-text screening, 12 articles were deemed eligible and included in this review. Data extraction was conducted by two reviewers. Reviewer one (L.H.) extracted data from all eligible articles. Reviewer three (C.S.) extracted data from three included articles to confirm reliable extraction (percentage agreement = 100%; κ = 0.91). Data extraction included demographics, study population and design, activity tracker information (including feasibility and compliance, wear time, and acceptability), and intervention features.
Assessment of methodologic quality
We assessed study quality using the Downs and Black checklist for the assessment of randomized and nonrandomized studies of health care interventions 34 (Supplementary Table S2). Scoring in this 27-item quality assessment included quality of reporting (e.g., is the intervention clearly described, have all adverse events been reported), internal validity (e.g., was an attempt made to blind those measuring the outcome), external validity (e.g., were participants representative of the population), selection bias (e.g., were participants randomized), and statistical power. Two reviewers (L.H. and D.M.) assessed all eligible articles, with discrepancies mediated by a third reviewer (C.S.). Some items on the Downs and Black checklist were not applicable: we eliminated items related to blinding as blinding the intervention itself is not feasible in PA interventions. 35
As done in a review by Richardson et al., we modified the categorization of the quality assessment checklist to focus on pre-comparisons and post-comparisons as opposed to randomized group comparisons. 35 We modified the original five-point power item by substituting with an item simply scoring whether a power analysis was present (yes = 1 and no = 0). 36
With the blinding items omitted and the modified scoring of statistical power, all items were scored with 1 point (yes) or 0 points (no) and summed together, making the highest possible total score of 25. Scoring ranges were therefore adjusted to the following levels of quality: excellent (23–25), good (17–22), fair (12–16), and poor (<12). 36
Results
Study identification
After identification of 3187 articles through our database search, we screened 2718 articles after duplicates were removed (Fig. 1). We assessed 40 full-text articles for eligibility and included 12 studies in our final analysis.
Study characteristics
Intervention features included in this review are presented in Table 1. Five studies recruited childhood cancer patients during their cancer treatment (n = 261)37–41 and two studies during maintenance therapy (n = 31).42,43 Five studies recruited childhood cancer survivors (n = 225), including two studies focusing on early survivorship with survivors <5 years post-treatment (n = 33)44,45 and three studies focusing on early and long-term survivors up to 14 years post-treatment (n = 192).46–48 Most studies were conducted in the United States (n = 8),39,41–44,46–48 followed by Germany (n = 3)37,38,40 and Sweden (n = 1). 45
Description of Interventions and Summary of Physical Activity and Other Health Outcomes
ALL, acute lymphoblastic leukemia; AVG, active video gaming; CG, control group; F/U, follow-up; HR, heart rate; HRQOL, health-related quality of life; IG, intervention group; MPA, moderate physical activity; MVPA, moderate to vigorous physical activity; n/a, not applicable; PA, physical activity; PDPAR, previous day physical activity recall; RCT, randomized controlled trial; RPE, rate of perceived exertion; SD, standard deviation; SMS, short message service; T1, time point 1; T2, time point 2.
Five articles assessed intervention feasibility.39,40,42,43,48 The duration of interventions varied across studies. Two interventions were <7 weeks long,37,42 five were between 10 and 16 weeks long,39,40,45,47,48 and five were more than 6 months long.38,41,43,44,46 Half of the studies were distance-delivered programs, with five studies using web delivery42,45–48 and one study focusing on telephone delivery. 39 Four studies were hospital based37,38,41,44 and two were home based.40,43 Interventions for patients on treatment included mostly hospital-based programs,37,38,41 studies for children in survivorship included mostly web-delivered interventions,45–48 and studies during maintenance therapy included one web-delivered 42 and one home-based program. 43 One study included follow-up assessments at 6 and 12 months post-intervention. 37
Study quality
The quality assessment included studies ranging from fair to excellent (scores 14–24) and is displayed in Table 1. The mean quality score was 18 (good). The consistency between reviewers was high (99.96% agreement). Items relating to reporting, including descriptions of aims, hypotheses, characteristics of participants, interventions, and main findings, were most adhered to (100%). Reporting for adverse events was least commonly adhered to (33%).
Activity tracker characteristics
We identified two distinct monitoring modalities for the activity trackers that studies used within this review (Table 2). Activity trackers were either used as a measuring tool that did not provide any feedback to the user or as a self-monitoring tool that provided feedback to the user (e.g., daily step count). Six studies used nonfeedback activity trackers (e.g., Actigraph) that measured MVPA,37,38,41,44,45,47 and four used trackers for self-monitoring by providing step counts.39,40,42,43 One study used both 48 and another study used an unnamed pedometer paired with a nonfeedback activity tracker. 46
Overview of Wearable Activity Trackers Used in the Included Intervention Studies
g's, units of gravity; MET, metabolic.
Of the six studies that provided feedback to the user, four used an activity tracker that allows the provision of real-time feedback to the researcher about the performance of the participants through an online dashboard.39,40,42,48 One study involved the study nurse to check the online dashboard daily and email the participant and parent(s) their activity level from the previous day with an encouragement message. 42 Activity tracker wear time during the intervention ranged from 2 weeks to 6 months across the studies. Six studies reported on activity tracker compliance and feasibility.37–39,42,44,48 All six studies reported high compliance ranging from 71.5% to 100% (Supplementary Table S3). Two studies reported on user experience and showed high acceptability of the Fitbit trackers due to its ease of use and ability for goal setting.40,48 The same studies also reported on limitations of the Fitbit with participants reporting technical issues and short battery life.
PA level outcomes
Nonfeedback activity trackers
Overall, two of six studies reported significant increases in MVPA.37,47 The Fit4Life intervention was a 4-month web-and-text weight loss intervention for childhood leukemia survivors 8–18 years of age. 47 Compared to controls, intervention Fit4Life participants older than 14 years (n = 9) increased their MVPA over 4 months (p < 0.05), whereas those younger than 14 years (n = 10) showed no change in MVPA.
Müller et al. also used a nonfeedback accelerometer and evaluated a 4-week inpatient rehabilitation program in children and adolescents with cancer. 37 Participants' MVPA decreased post-intervention at 4 weeks compared to baseline, and then increased at 12-month follow-up (p < 0.05), with the authors suggesting that the decrease followed by the improvement may have reflected participants' transition from undergoing cancer treatment to after cessation of cancer treatment. 37
Four out of the six studies using nonfeedback activity trackers showed no change in MVPA or step counts (n = 111 patients and survivors).38,41,44,45 Three of these four studies were 6-month hospital-based interventions for children and adolescents undergoing treatment38,41 or in early survivorship. 44
One study delivered a 10-week active video gaming intervention for children treated for brain cancer. 45 Participants were also provided with weekly video coaching sessions for motivation and evaluation of enjoyment. No change in MVPA was found (p = 0.22). Hooke et al. incorporated the Actigraph® to measure PA levels at 2, 4, and 6 months during clinic routine visits in children with cancer. 41 Step count did not change significantly over the three measured time points (p = 0.52). Children with lymphoma displayed a significant decrease in PA at 4 months from baseline, and then increased at 6 months (p < 0.001), whereas children with a solid tumor or acute lymphoblastic leukemia (ALL) did not show any improvement in steps per day (p = 0.12 and p = 0.37, respectively).
Activity trackers that provide feedback to users (self-monitoring)
Six studies used self-monitoring activity trackers and did not result in any significant increase in step count or MVPA.39,40,42,43,46,48
Gotte et al. evaluated the effect of a home-based intervention using the Fitbit® as a goal-setting and behavior tracking device in children and adolescents receiving cancer treatment. 40 The intervention group received a 6- to 8-week individualized exercise program comprising daily step goals and strength, coordination, and endurance exercises. The intervention group displayed improvements in individual step goals after the program (p < 0.05), although there was no significant difference between the intervention and control groups (p > 0.05).
Hooke et al. delivered their online intervention using the Fitbit website to children with ALL receiving maintenance chemotherapy, including full doses of corticosteroids. 42 Participants' median steps per day did not reach statistical significance (p = 0.08).
Ovans et al. delivered a telephone intervention that included physical therapist coaching and goal setting to increase steps. 39 They reported no significant change in the median daily steps from baseline to weeks 9–12 (p = 0.72), or from weeks 1–4 to 9–12 (p = 0.69). Two studies using both devices (Actigraph and a self-monitoring activity tracker) in their intervention also resulted in no significant change in PA.46,48
PA and health outcomes
Table 1 describes the health outcomes addressed in the reviewed interventions. Six out of 12 studies using activity trackers found improvements in health outcomes, including decrease in negative mood, 47 increased motivation, 48 improved body coordination, 45 increase in HRQOL,37,40 and improvement in aerobic endurance. 43 HRQOL was found to be improved immediately after 4-week intervention and sustained in the 6- and 12-month follow-up in one study (p < 0.001). 37 Müller et al. delivered an individualized inpatient exercise program without the use of a self-monitoring activity tracker. 37 The Fit4Life web-and-text and phone counseling intervention used a nonfeedback activity tracker and found that survivors older than 14 years (n = 9) demonstrated less weight gain (p = 0.05) and all participants (N = 19, 8–18 years old) reported reduced negative mood compared to controls (p < 0.05). 47
Intervention features
Common intervention features or approaches that complimented the use of activity trackers were identified in the included studies, such as goal setting and communication with health professionals. A summary of intervention features identified in each study is presented in Table 3. Study features ranged from two to six features, including offering health professional support, peer or parental support, education, goal setting, distance delivery, and individualization of programs, messages, or information (i.e., tailored specifically to the participant).
Number of Intervention Features Involved in Each Study
Intervention features that achieved the most significant positive effects on PA or other health outcomes are ordered from left to right.
Statistical significance of achieving significant positive effect on PA or other health outcomes (*p < 0.05, **p < 0.01, ***p < 0.001).
√ represent intervention features included in each study.
Used feedback activity tracker.
Parents received information on behavioral and parenting strategies.
We identified that both studies that achieved increases in PA offered individualization of programs. One intervention delivered an individualized exercise program for children and adolescents on treatment, 37 and the Fit4Life web-delivered intervention offered tailored text messages to each participant twice per day. 47 Studies that tailored programs to the individual appeared more likely to achieve improvements in other health outcomes than programs that did not include an individualized component. Four out of seven individualized programs reported significant improvements in health outcomes, including improved HRQOL,37,40 reduced negative mood, 47 and improved aerobic endurance. 43
Six out of 12 studies used goal-setting, with four studies pairing goal-setting with the use of feedback activity trackers (Fitbit),39,40,42,48 while two utilized goal-setting with a health coach or research staff.44,47 Significant improvements in health outcomes such as fatigue were identified in three of these six studies.42,47,48 Three studies using the Fitbit set a goal range of a 10%–20% increase in steps/day above participants' baseline in their intervention.40,42,48 In these studies, no change in MVPA was evident; however, improvements in other health outcomes included improved HRQOL and reduced negative mood.
Professional support was used in different ways, paired with the use of activity trackers, including face-to-face coaching or distance-delivered support (e.g., telephone calls or web-facilitated programs). Two out of nine studies used nonfeedback trackers and incorporated professional support resulting in significant improvements in PA37,47 and five resulted in improvements on other health outcomes.37,40,42,45,48 Hooke et al. included health professional support in their intervention by providing participants with tailored weekly step goals and daily emails with feedback from the study nurse, in addition to the use of the Fitbit monitor. 42 Similarly, Mendoza et al. used the Fitbit and involved research staff to facilitate a peer-based Facebook group with a focus on daily step count goal-setting and badges as a reward system for increasing PA. 48
Seven studies utilized a distance-delivered program, but only one achieved a significant increase in PA involving a nonfeedback tracker to measure PA levels at baseline and post-intervention. 47 Four out of the seven distance-delivered interventions using a mixture of feedback and nonfeedback activity trackers achieved significant improvements in health outcomes,42,45,47,48 such as improvements in body coordination. The study by Sabel et al. also used a nonfeedback activity tracker and delivered a Nintendo Wii movement game intervention, with video coaching sessions for brain tumor survivors, and found a 15% improvement in body coordination score (p < 0.05). 45
Discussion
This review is the first to investigate the effectiveness of activity trackers in PA interventions to improve PA levels and other health outcomes in the pediatric cancer population. Overall, findings from our review suggest that interventions using activity trackers did not show increases in MVPA or step counts in this population. However, interventions using activity trackers demonstrated positive impacts in other health outcomes such as improvements in aerobic fitness and HRQOL. These findings are notable as cancer survivors are at increased risk for short- and long-term comorbidities from cancer treatments, including obesity, cardiovascular disease, anxiety, and depression, with this risk potentially mitigated by increasing PA or fitness.9,49
Due to the limited number of studies and heterogeneity of study population, study design, and intervention characteristics, our findings showed limited evidence regarding which intervention features might have contributed toward a positive effect on PA. Nonetheless, activity trackers that provide feedback can be used as a motivational tool for users, whereas activity trackers without feedback can support objective measurements of PA to assess the efficacy of the intervention.
Activity trackers are being increasingly used as tools for researchers and clinicians to measure and monitor PA levels, in addition to being used as motivational tools to promote behavior change. Interventions varied between using an accelerometer to measure PA, using a pedometer (e.g., Fitbit) as a motivational device, or both. Wearable activity trackers appear feasible to use, with most studies showing high compliance with wearing the device (>71%). Only two studies reported on user acceptability, which was also high. Individualizing programs for participants appeared to be more common in interventions, which improved health outcomes compared with interventions that failed to do so. More research is needed to identify which intervention features are effective in increasing PA levels when paired with wearable activity trackers.
The two studies that showed an increase in MVPA did not use activity trackers as a strategy for users to self-motivate to increase PA levels in children and adolescents diagnosed with cancer.37,47 Instead, they used the activity trackers as a tool to measure activity, suggesting their improvements in MVPA were due to the intervention itself.
Six studies using feedback activity trackers showed no improvement in PA levels. These findings contrast with a review by Lubans et al. in healthy and obese children and adolescents 50 showing significant increases of PA levels in 12 out of 14 studies. Our review suggests that children affected by cancer may face additional barriers to increasing PA levels through PA interventions. Five of 12 studies included in our review involved children and adolescents during cancer treatment, which may pose additional challenges to increasing PA levels. Activity levels are expected to decline during the first year of cancer treatment 5 ; however, no change in PA levels may suggest a sustained level, where this may be a positive factor for children during treatment.
Key barriers to exercise have been identified in the adult cancer survivor population, some of which are also experienced by the general population, but exacerbated by cancer treatment. 51 Barriers identified include experiencing treatment-related side effects, lack of time, and fatigue. Further research is needed to identify guidelines on how to optimally promote PA in children and adolescents being treated for cancer and those who have survived cancer.
Results from our review focusing on childhood cancer also differ from studies in adult cancer survivors. A recent systematic review assessed the feasibility of 12 randomized controlled trial exercise interventions using activity trackers in adult cancer survivors and effects on PA levels. 52 The review reported that the use of digital activity trackers is feasible in adult cancer survivors. 52 They further found improvements in daily step counts and MVPA, as well as health outcomes, including fitness and body composition in some studies.
Our review suggests that new and novel strategies are needed to increase PA levels in children and adolescents diagnosed with cancer, who have different needs compared to adults with cancer. Young cancer patients and survivors experience unique impacts of cancer concerning self-esteem, identity development, family functioning and parental influence, social relationships, psychological distress, education and employment, and physical functioning. 53
Most studies included in our review targeted their intervention to a wide age range of participants, for example, 8–18 years. An exercise intervention delivered to an 8-year old may not be appropriate for an 18-year old, and vice versa. Structured exercise interventions may be more suitable for adolescents and young adults compared to children who achieve most of their activity through unstructured play. 54 Thus, due to developmental differences, children and adolescents may benefit from age-appropriate PA programs and services that could be enhanced by incorporating wearable activity trackers.
In our review, we identified common features of intervention studies that involved the use of a wearable activity tracker, including engagement with a health professional. Receiving individualized support from a health professional may be vital for this young population, particularly in a context where children affected by cancer have unmet needs regarding accessing age-appropriate information and services.53,55,56
Children and adolescents affected by cancer, and their parents, may need exercise-specific education, particularly in the context of cancer, to assist with maintaining or safely increasing PA levels during treatment and in survivorship. Providing education on healthy behaviors paired with activity trackers may assist children and adolescents in promoting risk-reducing behaviors such as increasing PA levels and reducing time spent in sedentary activity, so that these health behaviors can continue into adulthood. 57 One included study that increased MVPA in survivors provided education for parents to assist their family in healthy behaviors. 47 Furthermore, distance delivery, including home-based programs, telephone interventions, and digital applications, has been popular in reaching a wider network of cancer patients and survivors.32,58,59 Adolescent and young adult cancer patients have reported a preference for home-based programs, due to their low cost and convenience. 56 However, more research is needed to determine how to increase PA among this population, particularly when pediatric treating centers are geographically dispersed. 21
Limitations
Few of the eligible studies in this review were randomized controlled trials, with the majority being pilot studies with small sample sizes. Pediatric oncology research is typically limited due to the geographical dispersion among this population, fewer diagnoses in childhood cancer compared to adults, and heterogeneity in cancer diagnoses and treatments. These factors often result in small sample sizes. 60
There was large variability in the populations of cancer patients and survivors, age, outcome measures, types of interventions, measures of PA, and types of activity trackers. This heterogeneity and varied reporting of primary outcomes limited our ability to draw comparisons and make strong conclusions from the interventions, or to conduct a meta-analysis, which is common in reviews on related topics. 61
Few studies in our review investigated long-term effectiveness, hence it is important that future studies include longer follow-up periods to assess long-term behavioral changes. Future studies will also need to address the needs and barriers within this diverse population of children and adolescents diagnosed with cancer, including individualizing content to age-specific participants, giving consideration to race, socioeconomic status, health literacy, and geographic location.
Conclusion
PA interventions incorporating activity trackers within pediatric oncology are highly diverse in study design, study population, and intervention features. Our review revealed that PA interventions that used activity trackers in the pediatric cancer population did not increase MVPA or step counts. However, they did demonstrate positive impacts in other health outcomes such as improvements in aerobic fitness and HRQOL.
Further research is needed to understand how the use of activity trackers paired with specific intervention features (e.g., education or health professional support) can increase PA levels for this population. Nonetheless, activity trackers have the potential to provide objective measures of the level, intensity, and patterns of PA and sedentary behavior in children affected by cancer to both health care teams and the survivor themselves. Activity trackers can also allow health care teams to monitor activity patterns additionally with health outcomes such as fatigue and sleep, and may help to reveal how cancer treatments have impacted a child's engagement with PA.
Authors Contributions
All authors contributed to this article and approved the final version of the article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The Behavioural Sciences Unit at Sydney Children's Hospital is supported by the Kids with Cancer Foundation. Prof. C.E.W. is funded by a Career Development Fellowship from the National Health and Medical Research Council of Australia (APP1143767) and Kids with Cancer Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.