
Abstract
Purpose:
Most evidence for the relationship between physical activity, nutrition education, and late effects from cancer treatment come from cross-sectional studies. The purpose of this pilot study was to determine if 8 weeks of exercise and nutrition education in adolescent and young adult (AYA) survivors positively affects fatigue, quality of life, health-related fitness, and dietary intake.
Methods:
The exercise program targeted improvement in multiple areas of health-related fitness. A Registered Dietitian conducted nutrition education sessions with goal setting. To encourage activity, social engagement, and support, participants connected to a study-specific group. Fatigue and QoL (FACIT, PedsQL Teen, and Young Adult), health-related fitness (cardiovascular endurance, flexibility, muscular strength and endurance, anthropometrics), nutrition knowledge, and dietary intake assessments were conducted at weeks 1 and 10. Participant perceptions of strengths and weaknesses within the program were assessed after program completion.
Results:
Twenty four (16.6 ± 2.8 years) AYA cancer survivors began and completed the program. Problems with fatigue (PedsQL Teen and Young Adult) significantly improved along with decreased perceived barriers to exercise. Participants significantly improved cardiovascular endurance, flexibility, and muscular strength and endurance. Trying to make healthy nutrition choices, understanding how to read nutrition labels, and identifying a saturated fat significantly improved without a significant change in dietary intake. Participants' favorite program components related to exercise and social support.
Conclusion:
In view of the short- and long-term impacts of cancer diagnosis, treatment, and survivorship, as well as the benefits of physical activity on these factors, exercise programs with social support should be considered adjuvant therapy among AYA cancer survivors.
Introduction
Focus on survivorship health behaviors has increased with improved treatment methods and survival rates. 1 Seventy percent of adolescent and young adult (AYA) cancer survivors exhibit at least one chronic health condition five years post-treatment. 2 The Childhood Cancer Survivor Study identified that late heart and blood vessel effects after certain childhood cancers and stressed lifestyle related activities promoting heart and blood vessel health are important with AYA. 3 Common lifestyle related chronic health conditions also include persistent fatigue and obesity. 4
Quality of life (QoL) is affected by severe fatigue, stressing the importance of detection and management of fatigue. 5 AYA who met the national recommendations for physical activity guidelines had significantly better scores associated with QoL. 6 AYA survivors report preferences for in-person group exercise programs to improve both cognitive and physical factors associated with QoL. 7 These outcomes highlight the need for intervention studies to validate the feasibility and efficacy of exercise interventions in improving physical function and QoL for AYA.6,7
While fatigue among healthy adolescents is common, AYA with cancer and cancer survivors experience greater levels of fatigue, which is related to hindrance for accomplishing their goals.8–12 Cancer-related fatigue results in a lower QoL in survivors and ranges from acute pain, cognitive issues, and unspecified symptoms.13,14 Both physical activity, defined as any bodily movement produced by the skeletal muscles, and exercise, defined as planned, structured repetitive activity, programs improve feelings of fatigue, physical function, low energy, psychological well-being, and QoL while concurrently reducing the risk of chronic diseases and cancer (recurrence) in both general and cancer populations.1,15–18 Increasing evidence, including systematic reviews and National Cancer Institute (NCI), supports the safety and feasibility of exercise during and after cancer treatment to improve fatigue, muscular strength, and QoL.8,19–22 There is an antagonistic effect with fatigue affecting perceived ability to exercise and recommendations for exercise to improve fatigue symptoms. 8 More research is needed to better characterize the most effective programs for AYA cancer survivors.23,24 Specific predictors of AYA survivors' engagement in exercise include social support from peers, a structured and safe environment, knowledge of the long-term benefits specific to long-term health effects, and active engagement.1,4,8,16,25–32 Preferred activities among AYA cancer survivors include biking, walking, home-based or local (<20 minutes) locations, professional supervision, and physical activity trackers.4,33 While guidelines and evidence for safety and efficacy of exercise among AYA cancer survivors are clear, few interventions exist evaluating exercise and fatigue. 24
Most recommendations for cancer prevention focus on nutrition, weight, and physical activity to effect overall health and reduce the risk for chronic diseases. 34 Moreover, a balanced diet along with appropriate exercise can reduce fatigue and improve QoL by lessening depression, improving self-image, and increasing the likelihood of long-term healthy lifestyle choices. 15 To develop healthy habit practices into survivorship, AYA cancer patients should be educated about diet quality and physical activity. 35 AYA recognize the importance of nutrition for both cancer-specific and overall health concerns, as well as barriers to healthy dietary habits such as lack of knowledge and resources for healthy eating.36,37 AYA identify education, motivational tools, and social support as ways to improve dietary habits.36,37 While an intensive nutrition intervention was beneficial in improving healthy eating index scores, 38 results of less intense methods for this population are equivocal.39–41 The majority of evidence for the relationship between physical activity, nutrition education, and late effects from cancer treatment come from cross-sectional studies with limited evidence evaluating the effects of exercise and nutrition education on late effects among AYA.35,37,39,41
The purpose of this pilot study is to determine if an 8-week structured and supported exercise and nutrition education program in AYA cancer survivors can positively affect fatigue, QoL, health-related fitness, and dietary intake.
Methods
General
This study was reviewed and approved by the Institutional Review Boards of Roswell Park Comprehensive Cancer Center (RPCCC) and Buffalo State College, State University of New York. Teens Living with Cancer (TLC) – Fit is a program of Melissa's Living Legacy Teen Cancer Foundation. TLC's vision is that all teens with cancer have opportunities for life-affirming experiences throughout each stage of their disease. As such, adolescents (13–17 years) and young adult (18–24 years) survivors were recruited from RPCCC. The 10-week program included fitness instruction, nutrition education, and goal setting during weeks 2 through 9. Fatigue, QoL, fitness, and nutrition assessments were conducted in weeks 1 and 10. To encourage activity, social engagement, and support, participants were provided Fitbit™ and encouraged to connect to a study-specific group through the Fitbit™ app. The first day of the intervention began with participants/guardians signing consent and an explanation of the program and the importance of complying with each intervention area.
Recruitment and eligibility
Potential participants were given a flyer about the Teens Living with Cancer Fitness (TLC-Fit) program and, if <18 years, encouraged to discuss the opportunity with their guardian(s). Exclusion criteria included any joint or orthopedic limitations preventing weight bearing exercise, uncontrolled diabetes, abnormal hemodynamic measures, 42 and malignancies or leukemia if also contraindicated by physician recommendations. Any participant/guardian interested in the program was invited to an information session where study staff described the program and answered questions. At this session, consent was explained in detail, and forms requiring physician approval for exercise, questionnaires about cancer diagnosis and treatment regimen, exercise self-efficacy, demographics, QoL, and fatigue were provided. A deadline to sign up for the program was set for 1 week after the information session. Completed consent, forms, and questionnaires were required before starting the program.
Intervention
Exercise prescription
The exercise program targeted improvement in multiple areas of health-related fitness. Under supervision of a certified personal trainer, participants completed weekly one-hour full-body strength and conditioning sessions using GRAVITY® boards, Spin bikes, and resistance bands. To limit boredom and encourage activity beyond these one-hour sessions, new exercises were introduced each week and participants were provided resistance bands and a manual with photos, with a recommendation to exercise at home three times per week. Time spent using the bands at home was not recorded but highly encouraged.
Physical activity tracking and motivation
For personal tracking and motivation wrist-based activity trackers, Fitbit Flex™, were provided. Participants shared their step count with the group and were given star stickers if they achieved the highest step count for the week. Star stickers were collected and posted in an effort to motivate participants, as well as win a prize for most steps at the end of the intervention.
Nutrition education
To improve nutrition knowledge and dietary intake habits, a Registered Dietitian (RD) conducted nutrition education sessions using group discussions, handouts, demonstrations, and activities. Sessions covered a wide array of topics targeted to this population.43–45 The teaching plan was designed to foster empowerment through interactive, supportive, and appealing methods.
Goal setting
To provide direction and encourage motivation, weekly sessions began with setting a 7-day physical activity and/or nutrition goal with the personal trainer and/or RD.46,47
Questionnaires
QoL, fatigue, and physical activity self-efficacy questionnaires were completed at baseline and postintervention.
QoL–fatigue (FACIT)
FACIT-F, comprising Fatigue and FACT-G v4, is a validated self-report questionnaire that assesses specific QoL concerns related to fatigue and well-being in cancer patients such as physical well-being (PWB), social/family well-being (SWB), emotional well-being (EWB), and functional well-being (FWB), including a Trial Outcome Index (TOI) – sum of PWB and FWB. 47 Questions are scored with totals from 0 to 52. Higher scores indicate better QoL, and scores <30 indicate severe fatigue. 47
QoL–pediatric–multidimensional fatigue teen and young adult report (PedsQL)
PedsQL is a validated self-report questionnaire that assesses fatigue and QoL in 13–18 and 18–25-year-old pediatric patients. PedsQL Teen includes six items each scored for general fatigue (GF), sleep/rest fatigue (SRF), and cognitive fatigue (CF). PedsQL Young Adult includes 5–8 items each scored for physical function (PF), emotional function (EF), social function (SF), and school/work function (SWF). For each, scores are linearly transformed with higher scores indicating less fatigue. 48
Physical activity self-efficacy
Participants completed the Godin Leisure-Time Questionnaire to assess self-efficacy (e.g., perceived barriers and benefits of physical activity). Perceived barriers measure the impact of certain conditions and feelings on exercise habits on a 4-point Likert scale from 1 (strongly agree) to 4 (strongly disagree). Lower scores indicate lower perceived barriers to exercise. Perceived benefits measure reasons for exercise on a 7-point Likert scale from 1 (strongly disagree) to 7 (strongly agree). Higher scores indicate higher perceived benefits of exercise. 49
Nutrition knowledge
To describe changes in nutrition knowledge and dietary intake, a twenty-question nutrition quiz and 3-day dietary intake records were completed at baseline and postintervention. Total energy, macronutrient, and fruit/vegetable intake were analyzed using NutritionistPro. 50
Health-related fitness
Anthropometrics
Height, weight, body mass index (BMI-kg/m2), and body composition were recorded at baseline and postintervention. Participants were asked to refrain from moderate–vigorous physical activity two hours before testing. Height was taken using a movable rod stadiometer. Body composition and weight were measured using bioelectric impedance on an InBody™ 570. For height, weight, and body composition, shoes, socks, and jewelry were removed.
Prefitness testing
Blood pressure and resting heart rate were recorded at baseline and postintervention with an Omron™ 10 series automatic cuff. To ensure safety, blood pressure and resting heart rate were also recorded before and following each training session.
Muscular strength and endurance
Participants completed curl ups and push-ups to exhaustion at baseline and postintervention. Curl ups began and ended with head and shoulders on the ground. 51 Push-ups began in the up position with shoulders and legs straight and ended in the down position with chin touching a 4-inch tall marker. 51 Modified push-ups began with knees on the mat. For both curl ups and push-ups, participants set their own steady cadence. The number of curl ups/push-ups was counted until exhaustion, form was broken, or cadence slowed.
Flexibility
Lower back flexibility was assessed with a sit and reach box at baseline and postintervention. Participants began seated on the floor with both legs straight and palms facing downwards. The subject reached out and held the position for two seconds, and distance was recorded. 52
Cardiovascular endurance
Participants completed a modified-Cooper fitness test at baseline and postintervention. 53 Participants walked/ran at a self-determined pace for 1 mile on a treadmill at 1% incline to mimic outdoor activity. 54 Cardiovascular endurance was scored as total time to complete the distance.
Qualitative review of the program
Postintervention, participants completed open-ended questions about perceptions of strengths and weaknesses within the program.
Statistical analysis
Categorical variables were analyzed with Chi square. Pre–post continuous variables were analyzed with paired samples t-tests. Quantitative data are described as frequency (n (%)) and mean ± standard deviation (SD). Qualitative data were reviewed for content analysis and themes generated. Fitbit data were not analyzed due to poor compliance with wearing the device. Data were analyzed in SPSS v 24, and significance set at p = 0.05.
Results
Participant characteristics
Twenty-four participants (16.6 ± 2.8 years, 58.3% male), 18 adolescents and 6 young adults, began and completed the study. Participants were 3.06 years postcancer treatment. Further characteristics can be found in Table 1.
Characteristics of 24 Adolescent and Young Adult Cancer Survivors
Fatigue and QoL
Multidimensional fatigue improved, PedsQLTeen, with significant improvements in general fatigue (GF) and sleep rest fatigue (SRF) (Table 2). PedsQLYoungAdult PF significantly improved, and there were no significant changes in fatigue (FACIT), subscales, or TOI (Table 2). Perceived barriers to exercise significantly decreased in areas related to willpower (t(21) = 2.16, p = 0.042) and worries about an injury (t(22) = 2.077, p = 0.05) (Fig. 1). Overall perceived benefits for exercise did not significantly change with participants recognizing the benefits before starting the program.
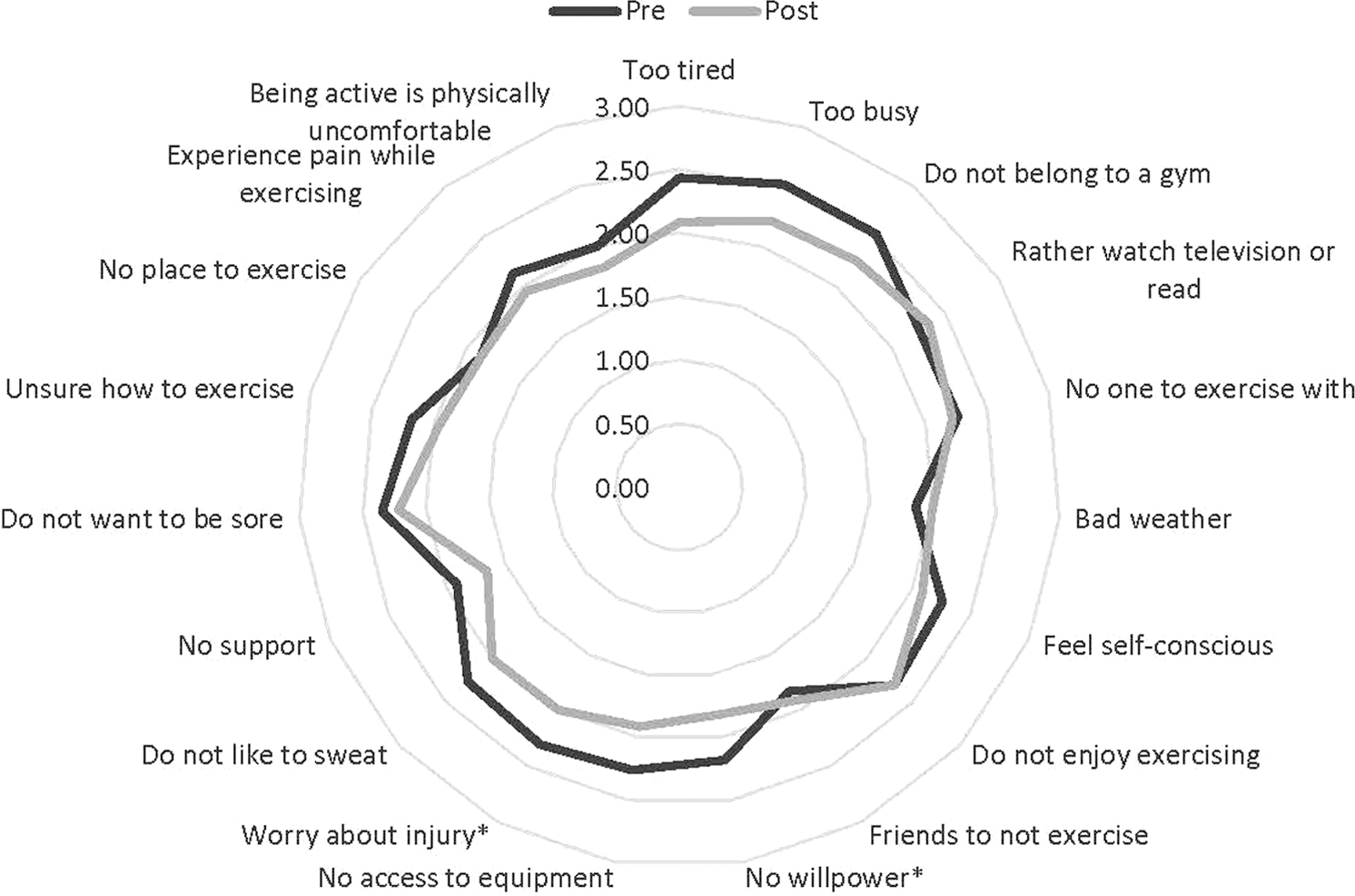
Perceived barriers to exercise before (pre) and after (post) an 8-week exercise intervention in 24 adolescent and young adult cancer survivors. *p < 0.05. Lower scores indicate lower perceived barriers. Radar map displaying perceived barriers to exercise both before in black and after in gray with significant improvement, p < 0.05, seen in “worry about an injury” and “no willpower”. Lower scores indicate lower perceived barriers.
Quality of Life–Fatigue (FACIT) and Quality of Life Pediatric–Multidimensional Fatigue Teen and Young Adult Report (PedsQL) Before and After an 8-Week Exercise Intervention in 24 Adolescent and Young Adult Cancer Survivors
TOI = PWB+SWB
Health-related fitness
Participants significantly improved cardiorespiratory fitness, flexibility, and muscular strength and endurance (curl ups and push-ups) (Table 3). There were no significant changes in anthropometrics, heart rate, or blood pressure.
Health-Related Fitness Before and After an 8-Week Exercise Intervention Among 24 Adolescent and Young Adult Cancer Survivors
Decreased time indicates improvement, faster to complete distance.
Nutrition
There were no significant changes in dietary intake. Nutrition knowledge significantly improved, including trying to make healthy choices (t(13) = −3.122, p = 0.008), understanding how to read nutrition labels (t(12) = 2.245, p = 0.044), and identifying a saturated fat (t(11) = 3.317, p = 0.007).
Program perceptions
Participants' favorite program components centered on exercise and social support. All felt that the program affected them in a positive way, including health-related fitness, nutrition, social connections, and general health. Recommendations for program improvements were related to exercise prescription and nutrition education. Final impressions of the program were very positive for all participants (Table 4).
Qualitative Results of Participant's Program Perceptions
Discussion
The primary purpose of this study was to determine if 8 weeks of exercise in AYA cancer survivors positively affected fatigue and QoL. Overall, symptoms of multidimensional fatigue (PedsQL) improved. Many cross-sectional studies exist describing a positive correlation between increased physical activity, reduced fatigue, and improved QoL.8,24,32,55,56 Similar to these results, 10-weeks counseling to increase physical activity significantly improved fatigue in adult survivors of childhood cancer. 57 Furthermore, a 16-week group exercise program improved health-related fitness and QoL. 58 However, a 12-week exercise intervention among 9.3 ± 3.2 year olds did not significantly affect QoL in cancer survivors. 59 Differing results may be related to several factors such as sample size, age, and duration of intervention. First, sample sizes in AYA intervention studies may be small due to low enrollment and high attrition.57,60 Second, it may be easier for older survivors, teens, and young adults to enroll and participate in interventions.24,60 Finally, with longer (10–12 weeks) interventions, the time commitment burden may outweigh perceived benefits of participation.24,60 For example, in a 12-week intervention among younger participants attrition was 55.6%. 59 Results of this study, in support of current recommendations, support exercise as standard of care adjuvant therapy for AYA to improve fatigue and QoL. 61
Regular participation in this exercise program significantly improved health-related fitness, including muscular strength and endurance, flexibility, and cardiorespiratory endurance. However, no significant changes occurred in anthropometrics. Similar to these results a 16-week group program significantly improved physical fitness. 58 However, a 12-week progressive program did not affect muscular strength or cardiorespiratory fitness but did improve BMI. 59 A primary difference between these studies is the group/social component. A specific predictor of AYA survivors' engagement in exercise includes peer social support.1,4,8,16,25–32 A favorite feature of this study among participants included social support. Social support from peers and family is recognized as an essential component during treatment and through survivorship. 62 Future studies should consider the benefits of social engagement among AYA cancer survivors for exercise interventions.
Self-efficacy for exercise improved along with reduced perceived barriers to exercise. Even though AYA recognize the benefits of and confidence in their ability to engage in exercise, symptoms of fatigue negatively impact perceived ability to exercise.1,4,8 The nature of the barriers to exercise in this study is similar to those identified by others such as safety concerns, physical limitations, and low energy along with an equivalent recognition of the benefits among AYA.4,36,63 This study did include methods to influence behavior change, including information, planning, social support, and goal setting. Self-efficacy is an important predictor of exercise maintenance. 64 Understanding the psychosocial aspects of caring for teens with cancer will drive the development of tools to provide them with the knowledge and self-efficacy to choose a healthy lifestyle. Taken together, the results of this study support the use of a similar intervention to improve self-efficacy and reduce perceived barriers to exercise.
The second aim was to determine if 8 weeks of nutrition education improve nutrition knowledge and dietary intake. There were no significant changes in dietary intake, but nutrition knowledge did significantly improve. A longer, four times over 3 months, nutrition education program for AYA significantly increased nutrition knowledge and fruit/vegetable intake while decreasing sweets/snacks intake. 38 In the current study, parents were the primary food purchasers and preparers. Only 12.5% of participants were solely responsible for meal preparation. Furthermore, 42% of participants reported eating outside the home less than once per week. Nutrition investigations among AYA are cross-sectional and describe dietary intake behaviors below recommendations with recognition of resources, social/peer support, and emotions as factors in dietary behaviors.37,39 Taken together, nutrition education improves nutrition knowledge; however, dietary changes may be dependent on age, independence, and/or education session intensity.
This pilot was successful in demonstrating benefit in Caucasian, two parent households with income >$60,000 but may not translate well into other groups more reflective of the population served by RPCCC. Other limitations include a small sample size and incomplete reporting from participants. Enrollment, participation, and follow-up are common problems of intervention studies in AYA.39,65 This pilot study had several strengths. First, AYA prefer programs that are both meaningful and motivational with goal setting.1,66 The participants enjoyed the program and were vested in each other and themselves as evidenced by their feedback (Table 4). Second, 65% of adolescents indicate biking as their preferred activity, and this program included Spin bikes. 4 Third, previous research identified social-related factors such as embarrassment and a lack of physical activities when with family and friends as barriers to exercise; this study addressed this concern by creating groups and a social network for participants to engage with cancer survivor peers, a favorite component of the program (Table 4).1,4 Finally, results of as few as six exercise intervention studies with at least 50% of the sample from the AYA population exist. 24 With the bulk of literature among AYA being cross-sectional, causal inferences are challenging. A review by Munsie et al. highlights the need for more intervention studies in this population. 24 The results of this study add to the limited causal data available.
In summary, this study demonstrated that an 8-week multifaceted behavioral and socially supported intervention significantly improved fatigue, QoL, and health-related fitness among AYA cancer survivors. In view of the short- and long-term impacts of cancer diagnosis, treatment, and survivorship, as well as the benefits of physical activity on these factors, exercise should be considered adjuvant therapy among AYA cancer survivors. Results of this study add to the limited and growing body of evidence describing effective exercise and nutrition education programs for AYA cancer survivors.
Footnotes
Acknowledgments
This study was reviewed and approved by the Institutional Review Boards of Roswell Park Comprehensive Cancer Center (RPCCC) and Buffalo State College State University of New York.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was financially supported by a Research Incentive Grant and an Undergraduate Summer Research Fellowship award from Buffalo State and by Teens Living with Cancer Fit (TLC-Fit) —a subunit of Melissa's Living Legacy Teen Cancer Support—which is funded, in part, by RPCCC and by Body Blocks Fitness in downtown Buffalo, NY.