
Abstract
Purpose:
In the literature, substantial differences have been reported regarding incidence and outcomes for the pediatric and adult groups with non-Hodgkin's lymphoma (NHL). Diffuse large B cell lymphoma (DLBCL) is the most common NHL subtype, and its outcome in adolescents and young adults (AYA) has not been widely investigated. This study aims at reporting our experience on the outcome of DLBCL in the AYA group.
Methods:
One hundred twenty DLBCL patients, 40 AYA patients, and 1:2 matched 80 control non-AYA patients were diagnosed and followed up at our center included.
Results:
In both groups, the median progression-free survival (PFS) and overall survival (OS) were not reached, without any difference between groups (p = 0.7, p = 0.7, respectively). The median follow-up time was 28 (range 1–133) months in all patients. In both groups, international prognostic index scores and early relapse were associated with worse PFS and OS, but in the non-AYA group, the immunohistologic type was, in fact, related to worse outcomes.
Conclusion:
DLBCL in AYA is a predominantly overlooked subject, due to the rarity of the disease. The outcome of DLBCL in this age group is not encouraging, which not only needs to be further investigated, but novel approaches must also be developed.
Introduction
Substantial differences have been reported regarding incidence and outcomes between pediatric and adult patients with non-Hodgkin's lymphoma (NHL). 1 Diffuse large B cell lymphoma (DLBCL), anaplastic large cell lymphoma, and Burkitt's lymphoma (BL) are the most common NHL subtypes in children. In adults, DLBCL and follicular lymphoma are the most frequent subtypes, with clinicopathological studies showing that the more favorable NHL subtypes are more often found in children. 2 The most prevalent NHL in adolescents is DLBCL. 3 Patients between the ages of 15 and 39 are considered as adolescents and young adults (AYA). 4 The median age of diagnosis in DLBCL is 64. 5 Although DLBCL is the most common NHL across all age groups, its incidence also increases with age, so it is relatively rare in AYA.5,6 A vital aspect of AYA care regards the needs in this age group. The support approach differs from that of pediatric or adult patients. 7 Although the prevalence of AYA lymphoma has increased over the past 20 years, recovery has not substantially changed, requiring a greater understanding of lymphoma epidemiology and physiology in this group. 8 At this age, data on the nature of the disease and treatment approaches are limited.9,10 The awareness of special medical needs in AYA has emerged, resulting in an increase in cancer-related publications from 6 in 1997 to 59 in 2007 and 269 in 2017. Cancer incidence in the AYA age group is four times higher than in the pediatric age group. 11 Specialized AYA care programs were organized in the United States and some European countries. 12 Treatments targeting prolonged survival with minimal toxicity, including fertility, are preferred in this patient group, with specific treatment options for DLBCL patients in the AYA group. Large-scale trials are expected to establish therapy approaches and clinicopathological characteristics. This study aims at investigating the outcome of the AYA group of patients with DLBCL.
Patients and Methods
Patients diagnosed with DLBCL by immunohistochemical analysis, aged 18–39 with matched controls from 2011 to 2020, were enrolled in this study. Forty AYA patients, Ann Arbor staging, international prognostic index (IPI) score, lactate dehydrogenase (LDH), immunohistochemical subtype, treatment, and radiotherapy (RT) 1:2 with 80 matched controls, 40 and older, for a total of 120 patients were included in the study. Patients with transformed or secondary lymphoma, primary central nervous system (CNS) lymphoma, or those with major organ dysfunction, preventing intensive treatment, were excluded from the study. Patients were divided into two groups: those aged 15–39, the AYA group, and patients aged 40 and older, the non-AYA group. Patient characteristics can be seen in Table 1.
The Characteristics of Patients According to Age Groups
Asterisk indicates statistical significance.
ABC, activated B cell–like; AYA, adolescent and young adult; CR, complete response; GCB, germinal center B cell–like; IPI, international prognostic index; LDH, lactate dehydrogenase; NA, not available; PR, partial response; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; ULN, upper limit normal.
This research was conducted under the ethical principles and clinical practices of the Declaration of Helsinki. In addition, local institutional ethical approval was received (No. 2020–06/678). Demographic information: Age, gender, disease-specific data, Ann Arbor staging, IPI score, extranodal involvement, LDH, immunohistologic subtype, comorbidities, RT, treatment modalities, and responses were analyzed retrospectively.
Ann Arbor staging was used for patients with computed tomography and/or positron emission tomography. 13 Treatment response was assessed according to the Lugano NHL response criteria. 14 High-risk patients, as identified in the National Comprehensive Cancer Network (NCCN), were administered prophylactic intrathecal chemotherapy (12 mg methotrexate, 40 mg cytarabine, and 4 mg dexamethasone). A complete response (CR) was described as the absence of all clinical evidence of disease. The overall response rate (ORR) was defined as the ratio of patients who achieved partial or complete remission. 14
Patients with early stage (I–II) received 3–4 cycles of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) and patients with CR consolidated with RT. Patients with late stage (III–IV) and also patients with the early stage with partial remission after the 3–4 cycle chemotherapy received 6–8 cycles of R-CHOP treatment. Consolidative RT was given to residual lesions after chemotherapy, and also RT was given at the extranodal site with the physician's discretion. Treatment details are given in Table 2.
Treatment Details of Patients
N/A, not applicable; ORR, overall response rate; R-EPOCH, rituximab, etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin; R-GCVP, rituximab, gemcitabine, cyclophosphamide, vincristine, prednisolone.
Diabetes mellitus, hypertension, coronary artery disease, congestive heart failure, chronic obstructive disease, chronic kidney disease, cirrhosis, and other cancers in remission were evaluated as comorbidities.
Statistical analysis
IBM SPSS Statistics v. 26 (Armonk, NY) was used for statistical analysis, as well as to summarize data. Categorical data were given as ratios, and numerical data as medians (minimum to maximum) and means (±standard deviation). A chi-square test was able to compare categorical variables. Progression-free survival (PFS) was defined as the period from diagnosis to the first recurrence of disease (progression or relapse), death from any cause, or the last follow-up in patients without relapse. Overall survival (OS) was described as the period from diagnosis to death from any cause. Kaplan-Meier survival analysis was applied for PFS and OS, with log-rank tests used to assess factors affecting survival. p Values of ≤0.05 were regarded as statistically significant.
Results
There were 40 patients in the AYA group and 80 in the non-AYA group. The median age for both groups was 31 (range 19–39) and 57 (range 41–73), respectively. Median follow-up was 28 (range 1–133) months in all patients. Patient characteristics can be seen in Table 1.
AYA group patients
In the AYA group, after first-line therapy, the ORR was 75% in the germinal center B cell like (GCB) subtype and 85.7% in the activated B cell like (ABC) subtype (p = 0.3). In AYA group patients, median PFS and OS were not reached, although after 1, 3, and 5 years—OS was 84%, 80%, and 75%, respectively. Relapse was detected in nine (22.5%) AYA groups. Median relapse time was 15.6 (2–51) months. Factors affecting PFS and OS in the AYA group are depicted in Table 3. A high IPI score was linked to worse PFS (p = 0.02) and OS (p = 0.02), and early relapse was related to poor PFS (p = 0.01) and OS (p = 0.001).
Factors Affecting Progression-Free Survival and Overall Survival in Diffuse Large B Cell Lymphoma in Adolescent and Young Adult Patients
Asterisks indicate statistical significance.
CI, confidence interval; IHC, immunohistochemical; NR, not reached; OS, overall survival; PFS, progression-free survival.
Non-AYA group patients
After first-line therapy for non-AYA patients, ORR was 95.2% in the GCB subtype, and 74.4% in the ABC subtype (p = 0.09). In non-AYA patients, median PFS and OS were not reached; whereas after 1, 3, and 5 years, OS was 82%, 74%, and 65%, respectively. Relapse was seen in 19 (23.8%) patients. Median relapse time was seen in 8 (1–71) months. Factors influencing PFS and OS in non-AYA patients are depicted in Table 4. Similar to the AYA group, a high IPI score is associated with worse PFS (p = 0.001) and OS (p = 0.001), and early relapse coincided with inferior PFS (p = 0.001) and OS (p = 0.001). Unlike AYA, the immunohistologic-GCB subgroup had inferior PFS (p = 0.03) and OS (p = 0.04).
Factors Affecting Progression-Free Survival and Overall Survival in Diffuse Large B Cell Lymphoma in Non-Adolescent and Young Adult Patients
Asterisks indicate statistical significance.
Groups were matched for gender, IPI scores, Ann Arbor staging, immunohistochemical subtype, extranodal involvement, and treatment, with the exception of comorbidity (p = 0.001). For AYA and non-AYA groups, the median PFS and OS were not reached, with no differences detected regarding PFS (p = 0.7) and OS (p = 0.7) among groups (Fig. 1).
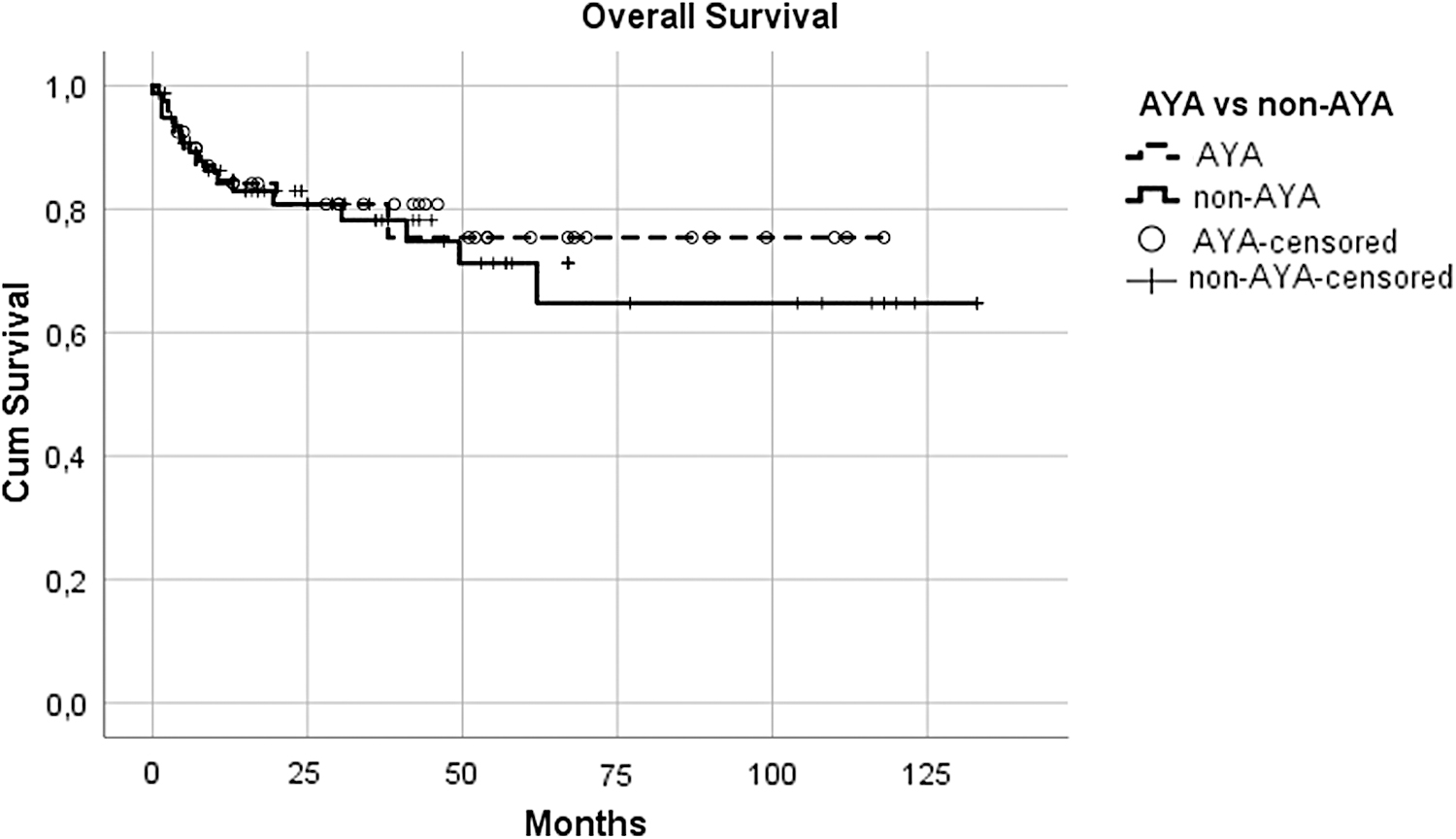
Overall survival between groups.
Discussion
As stated, no difference was seen regarding survival in AYA and non-AYA groups. Although the AYA group had less comorbidities, this did not reflect a survival advantage. High IPI and early relapse were associated with poor survival in both groups.
The incidence of NHL increases with age, but it is relatively rare in the AYA group. 15 Advancement in the management of hematological malignancies in the AYA group was less significant than gains achieved in children and older adults in the past two decades. 16 Given that age is one of the prognostic indicators of IPI, in previous studies of increased age, the incidence of adverse molecular markers often escalates with DLBCL. 17 We anticipate that treatment outcomes in AYA patients could be better than in adults; previous studies on clinical outcomes had been unsatisfactory. Specific molecular markers (e.g., the ABC subtype and BCL-2) were associated with worse prognoses and increased age. This supports the theory that lymphoma cell biology may help us understand some outcome discrepancies, rather than just treatment approaches. 17
Malignancies in the AYA group have attracted attention to therapeutic approaches, considering patient-related factors: late complications, psychological, and social aspects.16,18 Recent studies indicate improved outcomes in acute lymphoblastic leukemia treating AYA patients with pediatric protocols versus with adult protocols.19,20 Similar regimens are used in pediatric treatment of DLBCL and BL, which consist of cyclophosphamide, anthracyclines, high-dose methotrexate, and cytarabine (in the BFM—Berlin-Frankfurt-Münster—group trials).21,22 Conversely, BL is treated with short-term protocols in adults, but DLBCL receives standard R-CHOP-like regimens. In a study in which adults were treated with pediatric protocols, the outcomes were slightly worse. 21 Treatment of AYA varies substantially, and no consensus exists on the ideal treatment protocol. No evidence indicates that AYA DLBCL patients gain an advantage from pediatric therapies. To improve the clinical outcomes of AYA DLBCL, it is critical to further examine the clinical and biological characteristics of the poor prognosis subgroups and investigate therapeutic strategies. 16
French–American–British (FAB)/Lymphome Malins de Burkitt (LMB) 96 study included both pediatric and adolescent patients with B cell NHL. In a univariate analysis for ages ≥15 years, a significantly worse 5-year event-free survival (EFS) was demonstrated, with a 5-year OS in the adolescent group versus in younger children (5-year EFS for <15 years vs. ≥15 years: 87% ± 1.1% vs. 80% ± 3.6% [p < 0.045]; 5-year OS for <15 years vs. ≥15 years: 91% ± 0.03% vs. 85% ± 3.2% [p < 0.041]). Age difference outcomes faded with Cox multivariate regression and clarified by tumor histology (DLBCL), advanced stage (bone marrow/CNS involvement), and elevated LDH yielding a twofold upper limit of normal in adolescents versus children, aged >15 years. 23 In a previous study, 36 AYA DLBCL cases were included with 1328 patients with DLBCL, accounting for 2.7% of patients. The 5-year EFS and OS rates in AYA were 52% and 58%, respectively, which were relatively low versus pediatric patients. OS was not affected by gender, stage, LDH, B symptoms, or size of the largest mass at diagnosis. 8
Coso et al. investigated 55 patients aged >15–30 years, matched with 365 patients aged 31–65 years. The AYA patients presented with a bulky mediastinal mass (51% vs. 21%), and the LDH value was significantly higher (73% vs. 54%). The CR rate was similar in the two groups. Five-year OS and EFS for AYA were 73% and 68%, respectively. Analysis showed no difference for OS or EFS, as this outcome coincides with older patients. Our results were similar, with no survival differences among different age groups. 24
In a study conducted by Suzuki et al., 798 DLBCL patients older than 15 years old were included, with a median age of 68 years; there were 42 AYA DLBCL cases, or 5.3% of patients. The 2-year PFS and OS rates in AYA were 61.9% and 68.5%, respectively, which were relatively low compared with patients in the age group from 40 to 60 years old (65.3% and 78.7%, respectively); however, differences between the two groups were not statistically significant (p = 0.0724 and p = 0.4016, respectively). Our findings emphasize that there was no survival difference between the AYA and non-AYA groups. 25
The limitations of our study involve unavailable data; due to its retrospective nature, a few patients enrolled due to low incidence of DLBCL in AYA; groups were unmatched for comorbidities and also had a relatively short follow-up.
Moreover, DLBCL in AYA was largely overlooked due to its rarity. On the other hand, the outcome of DLBCL in AYA was discouraging, which should be investigated in future, while simultaneously developing novel approaches.
Footnotes
Acknowledgments
Tahir Darçın and Derya Şahin assisted in data accumulation. Dicle İskender and Nuran Ahu Baysal assisted in improving the language of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.