
Abstract
Purpose:
Adolescent and young adult (AYA) cancer survivors (15–39 years) often struggle with their post-cancer identity. We developed an age-appropriate positive psychology group intervention with fellow AYA cancer survivors in a nature-rich environment. The aim of this study was to examine the needs and expectations of participants of this new, 1-week post-cancer identity intervention, and to evaluate their experiences to identify factors that contribute to the quality and impact of post-cancer mental health care interventions.
Methods:
This was a mixed-method exploratory pilot study evaluating a new, 1-week post-cancer identity intervention. The participants (n = 13) completed questionnaires at baseline measuring needs and expectations, and on the last day of the intervention and at 1-month follow-up, measuring experiences.
Results:
Participants' expectations to be supported in finding their post-cancer identity and receiving acknowledgment and recognition of their suffering in fellow AYAs were met. The intervention was perceived as positively contributing to post-cancer identity development (n = 11) and several aspects of well-being. Most appreciated elements of the intervention were peer support and the nature-rich environment on perceived well-being.
Conclusion:
The group-based positive psychology after care intervention in nature for AYA oncology was well received by participants and provided useful feedback for improvement of future editions. The intervention could offer support to AYA's in the promotion of their well-being and post-cancer identity development, but more research is needed to confirm this.
Introduction
Involved in the experience of having had cancer is the process of integrating the experience into one's new or renewed self-concept. 1 Moving from an identity as a healthy individual to being diagnosed with cancer and to becoming a cancer survivor often causes a shift of identities, from the old, pre-cancer identity, to a patient identity during treatment, to a new post-cancer identity. 2 Experiencing cancer can thus result in changes in the self-identity of cancer survivors. The post-cancer identity often includes easy recall of the emotions associated with cancer and recovery, concern about one's health, and a feeling of vulnerability. 1 Individuals can identify with different labels after they had cancer, such as survivor, victim, or (ex-) patient. 3 Self-identifying as a cancer survivor was found to be related to better well-being and quality of life. 4 When the diagnosis was during childhood, those identifying as cancer survivors were more likely to transition successfully into adult care. 4
Peer support with other cancer survivors has been shown to affirm a strong survivor identity by enabling bonding with positive role models and overcoming challenges during the program. 5 Yet adolescent cancer survivors often struggle with psychosocial problems around their development of this post-cancer identity, such as struggling to make a contribution to society or to redefine their values. 6 They have to establish a new identity, since they cannot reclaim the life and old identity they had before the cancer diagnosis, as they are not sick anymore, but not yet back to how they were either. Such an identity struggle can have a negative impact on their post-cancer lives. 7
Adolescent and young adult (AYA) cancer survivors generally have more mental health problems than their peers, such as more mood disorders. 8 They also generally rate their quality of life lower than their peers and report concerns in specific areas of social well-being, such as establishing and maintaining meaningful relationships with peers. 9
The impact of cancer in AYAs is especially serious, as it affects developmental aspects during an age where unfolding a sense of identity is of utmost importance. 10 Indeed it is suggested that cancer survivors' well-being and adjustment to their social environment is partly explained by their ability to reconcile their view on “an ideal healthy self with their actual experiences of new or different physical, existential, emotional, or social capabilities.”1(p240) Post-cancer identity could therefore, in part, be understood as the product of the reconciliation process regarding the discrepancy between the actual and ideal or past sense of self, and AYA survivors could benefit from support in their struggles in this reconciliation process to (re)construct their post-cancer identity and functioning in society.
Research has shown that age-appropriate mental health aftercare with fellow AYA survivors is beneficial for psychosocial recovery. 11 Globally, there are only a few age-appropriate evaluated interventions that are directed to improve the psychosocial well-being of AYA survivors after their treatment is completed. 12 For example, there are projects in Canada and Australia that address the needs of this group, although they do not focus on post-treatment or mainly use cognitive behavioral therapy approaches. 13 In the Netherlands and Belgium (Flanders), there is no structural, multiday peer intervention with psychosocial aftercare for AYA cancer survivors yet. Therefore, we developed a new intervention that addresses the specific psychosocial needs in the group of younger cancer survivors from the Netherlands and Flanders.
The intervention has a unique, multidisciplinary approach, using positive psychology as the main framework, promoting aspects of positive functioning and emotional, psychological, and social well-being (positive mental health) rather than focusing on preventing or curing psychopathology (mental ill-health) 14 Positive psychology is the scientific study of the processes and conditions, which contribute to the optimal functioning or “flourishing” of individuals and groups, as well as institutions. 15 Although the field is still relatively young, many interventions have been developed and evaluated. 16 Positive psychology interventions either focus on positive topics, operate by means of positive mechanisms, address a positive outcome variable, or are designed to improve well-being rather than fixing weakness. 17 A recent meta-analysis indicated that positive psychology interventions are indeed effective in enhancing well-being, as well as decreasing depression and anxiety in clinical populations, such as cancer patients. 18
An innovative aspect of the intervention was the setting in a nature-rich environment. The impact of nature on (mental) health is assumed to have at least three pathways 19 : (1) through harm reduction, for example, clean air and natural sounds provide antidotes to environmental stressors; (2) through offering the possibility to restore affective, cognitive, and physiological capacities, after for example being stressed or emotionally or cognitively exhausted 20 ; and (3) through the capacity building effect of being connected with nature such as increased levels of personal growth, self-esteem, self-regulation, social competency, and an increased sense of autonomy. 21 Nature also provides an appropriate context for reflecting on one's own identity goals and values and thus contributing to self-understanding. 22 Nature-based interventions have been shown promising for the processing and recovery of young cancer survivors. 23
In this original article, we will describe the pilot-tested new intervention, which is the first of its kind combining a positive psychology framework in a nature-rich setting for this target group. The purpose of this article is: (1) to describe the intervention and its elements; (2) to assess the needs and expectations of participants before the start of the intervention; (3) to evaluate the experiences of the participants of the intervention; and (4) to make suggestions for future research.
The aim of this study was to examine the psychosocial needs and expectations of participants of this new, 1-week post-cancer identity intervention, and to evaluate their experiences to identify factors that contribute to the quality and impact of post-cancer mental health care interventions.
Methods
Design
This is a mixed-methods exploratory study, combining both quantitative and qualitative methods. Questionnaires were taken at baseline (2 weeks before the start), post-intervention on the last day of the program, and follow-up 1 month after finishing the intervention.
Intervention
A 6-day, group-based residential positive psychology intervention was organized in a nature-rich setting with the aims to (1) create an opportunity for AYA survivors to exchange experiences, foster understanding and recognition, (2) offer an intervention that stimulates participants to collectively orient themselves on their post-cancer identity and role in society, and (3) make a first step in the development of an effective and sustainable positive psychology intervention in nature for AYAs after their medical treatment.
The intervention has been developed by the three facilitators (see below) with feedback from a potential female participant. Input and feedback was received on the content, structure, and context of the intervention from the health care providers of the AYA Oncology Department of a Dutch University and a senior clinical psychologist with experience in the treatment of cancer patients (non-AYA specific) of another Dutch university.
The intervention took place in a training center located in an arboretum in Northern Italy. The natural setting was used mainly in reflection exercises to aid self-understanding and self-expression using artefacts from nature. Furthermore, nature was used for recovery from emotional and physical fatigue and to facilitate social processes.
The intervention made use of evidence-based elements of positive psychology,24,25 trauma, and body-oriented therapies, which focuses on the nervous system, 26 art, 27 yoga,28–30 and acceptance and commitment therapy (ACT). 31 ACT is a third-wave behavioral therapy, based on insights from behavioral therapy, cognitive behavioral therapy, and mindfulness-based therapies. 32 It aims to enhance acceptance of negative experiences instead of reducing symptoms, with the ultimate goal to promote psychological flexibility, the ability to act effectively, and in accordance with one's own personal values in the presence of negative private experiences. 31 It trains the positive psychological skills of contact with the present moment, values, committed action, self as context, defusion, and acceptance.
As preparation, participants received a narrative autobiographical exercise 24 4 weeks before the start of the intervention that served as input for the intervention. Participants were asked with the help of guided reflection questions to write up their life story in circa five pages, structuring the text in “life phases” to reflect on their story. They were asked to provide a photo per life phase.
The arrival and first day of the intervention were dedicated to creating an emotionally safe learning environment, in which participants feel safe to express emotions, confident to take risks, and feel challenged and excited to step out of their comfort zone. This was important because most participants did not know each other and the intervention required participants to open up toward their peers about personal and sensitive topics related to the cancer experience. Participants also shared their needs and expectations regarding the week, which were evaluated on the last day.
The second day of the intervention aimed at recognizing and expressing certain negative and painful emotions related to the cancer episode, such as shame, guilt, and anger through Gestalt theater approaches and an art workshop. Days 3–5 were focused on aspects of positive functioning, using value-based living and strengths and talents as new points of reference for the post-cancer identity. The potentially traumatizing effect of the cancer experience on the nervous system was also discussed through psychoeducation, without intentionally addressing any individual traumatic experience as this would not be appropriate for the context of a group setting.
The last day of the intervention focused on the future; their post-cancer identity. All previous workshop results were input for the last day. Participants were invited to write the next future chapter of their autobiography and share this in front of the group. The afternoon was dedicated to providing psychological tools and support for the post-intervention and the evaluation of the intervention. Participants were invited daily to spend at least half an hour in solitude in the forest to reflect on their experiences. Workshops were conducted both indoors and outdoors. Figure 1 shows the timetable.
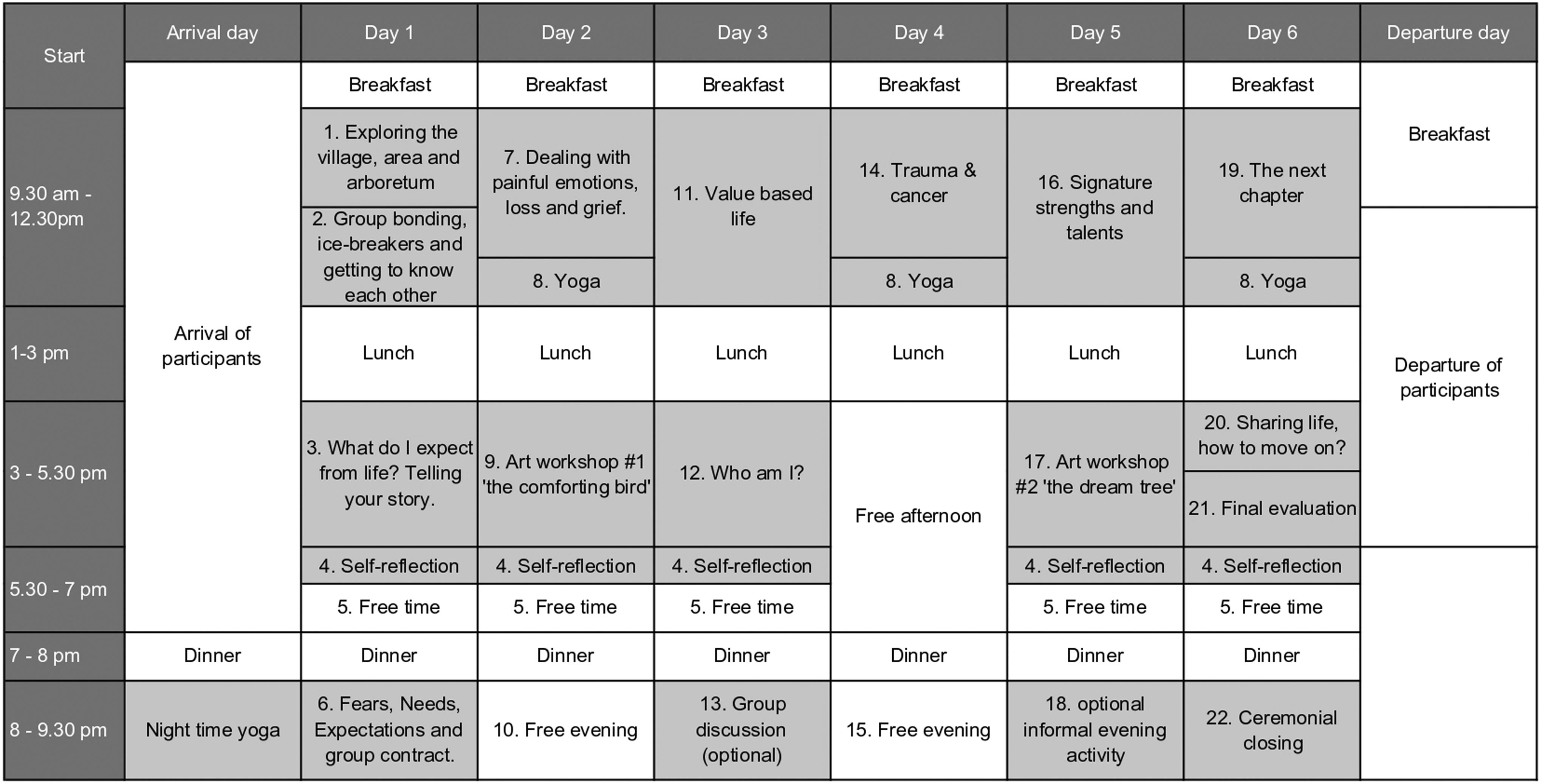
Timetable of the intervention.
The general approach of the sessions was experiential learning and stimulating self and group reflections by the participants, with the facilitators structuring the session and taking care that the input came mainly from the participants themselves.
Facilitators
Three facilitators were present during the week and guided the sessions: an ACT-certified psychologist, an art therapist, and a yoga teacher. Intervision sessions were held between the facilitators during the intervention week, to maintain high standards of mental health care and to support the well-being of the facilitators.
The facilitators had several years of experience facilitating groups of young people with different kinds of disabilities (e.g., autism, stammering) on the topic of mental health promotion and identity development using positive psychology and trauma-related therapies. They did not have specific AYA experience, however, they held consultation meetings with AYA's and AYA health care specialists to familiarize themselves with the specific issues AYA's deal with in general. The facilitators were selected by the sponsors of the intervention.
Participants
Participants were recruited with the support of the Dutch and Flanders' AYA care networks and patient organizations. These networks sent invitations by emails to their members and made posts on their fora and social media channels. The participants could apply online using an application form containing self-assessment questions to assess their fit with the inclusion criteria and objectives of the intervention. The criteria were assessed by the facilitators and further phone calls with the potential participants were held when there were doubts or unclarities.
Inclusion criteria were an age between 18 and 39 years 33 and having finished the cancer treatment, with the exception of hormone treatment. Exclusion criterion was having severe mental problems, which was measured through one self-assessment question.
Thirteen participants from the Netherlands (n = 3) and Flanders (n = 10), of which 10 were females, took part in the intervention. Their mean age was 28.58 years, ranging from 19 to 36 years (standard deviation [SD] 6.2). On average, participants were diagnosed with cancer 3.1 years before the intervention (SD 6.9). Nine participants received some kind of mental health care (e.g., individual or group therapy) from health care professionals. Tabe 1 shows more detailed demographics of the participants.
Demographics of the Participants (n = 12)
Procedure
Two weeks before the start of the intervention, the baseline questionnaire, including an informed consent form was sent in hard copy to the participant's home address. Participants completed the baseline questionnaires, including demographic questions with pen or pencil. The intervention was evaluated through a questionnaire on the last day of the intervention (post-treatment) and 1 month after the intervention (follow-up). The follow-up questionnaire only contained questions for long-term effect. Regarding completion of the questionnaires, 12 people filled in the baseline questionnaire, all 13 the post-treatment, and 9 participants filled in the follow-up questionnaire.
Instruments
The outcome measures reported in this study were part of a larger measurement battery of a longitudinal effect study (these results will be presented in a separate article), including instruments measuring quality of life, anxiety and depression, mental health, self-efficacy, and spiritual attitude and involvement measures. In this study, we will only report the outcome measures that are relevant in the context of evaluation. Table 2 provides an overview of the instruments and example questions per each round of questionnaire.
Overview of Variables, Instruments, and Example Questions
AYA, adolescent and young adult.
Baseline
The baseline questionnaire consisted of questions on demographic and personal health care characteristics (21 questions, e.g., age, gender, cancer type, sort, and satisfaction of medical treatment received), needs and expectations for the intervention (5 open questions), and experiences with and the impact of the cancer experience on well-being and identity (5 open questions).
Post-intervention
Regarding the evaluation of how far expectations were met (1 multiple choice with 4 choices between not at all met and met beyond expectation), quality of the intervention (10 questions on a scale from 0 to 10 with optional comments), favorite and least favorite session and what they would change (3 open questions), and the perceived effect of the intervention on well-being and identity (10 multiple-choice questions, 1 open question) were measured.
As there is no validated instrument available to measure post-cancer identity as to how it was defined for this study, it was measured through an open question and multiple choice items that are based on the definition of post-cancer identity as a product of reconciliation process (items acceptance, finding meaning in having had cancer) and positive functioning in society (item role in society). These items were complemented by typical constructs of well-being (items self-worth, purpose in life, and trust in the future). Conversations held with noninvolved AYAs, before the intervention suggested the items dealing with the fear of death, feeling peace in mind and body, and processing trauma and sadness.
Experience of the intervention was also measured using the validated Dutch translation of the Session Rating Scale (SRS). 33 The SRS contains four subscales measuring satisfaction (overall, approach and method, goals and topics, and relationships with facilitators and the group) on a 10-cm-long continuum. Reliability (Cronbach's alpha) is 0.90. 34 Participants rated their experience by marking the line with an “X” on the continuum. Scores closer to 0 represent negative experiences and scores toward 10 are more positive experiences. The SRS was slightly adapted as questions were changed to rate the experiences of the entire intervention (i.e., the past week) instead of individual sessions, as in the original scale.
Follow-up
At follow-up, it was measured how participants would describe their experiences, what they liked best and what they did not like about the intervention, and tips for improvement (four open questions).
Analysis
Descriptive statistics were used to describe the SRS and other structured questions, indicating mean and SD, as well as minimum and maximum score. The open questions were coded by the first author applying quantitative content analysis, 35 with categories emerging from the participants' responses. Quantitative content analysis is a research method that analyzes features of textual, visual, or aural material through systematic categorization and recording. 35 Substantive words and phrases of the responses were coded using objective (e.g., yes/no) and conceptual categories (e.g., positive/negative perception, negative mood issues, finding acknowledgment). The aim of the content analysis was to identify and categorize the responses for each variable. Computational analysis was done using Microsoft Excel.
Results
Baseline (n = 12)
Participants reported on their “health care satisfaction.” Eight participants out of 12 reported to be dissatisfied about the health care received during medical treatment. They mainly mentioned poor communication with health care providers (n = 3) and the absence or limited mental health support (n = 5). They were discontent with the quality of health care after their medical treatment (n = 9). Eight participants mentioned that they were not offered any kind of mental health care at post-treatment, while they would have liked to receive such care.
Regarding the “needs and expectations” before the intervention started, 9 participants out of 12 reported having a need and the expectation to resolve post-cancer identity-related issues, such as attitudes toward the self, the future, and relationships. They also hoped to be able to understand and process the experience of having had a life-threatening disease better after the intervention. Other participants expected to find recognition and acknowledgment of their personal experiences among other participants, rather than finding direct emotional support.
“Experiences with and the impact of the cancer experience on well-being and identity.” Eight participants reported at the time of the baseline measurement to experience more symptoms of stress or negative mood (e.g., irritability, anxiety) than usual. Other issues were poor concentration, forgetfulness, and difficulties reasoning. Eleven participants reported that the cancer diagnosis changed their sense of identity, of which seven said it was rather a negative change and four a rather positive change. The negative perceptions mainly referred to changes in the social domain of life, for example finding it more difficult to relate to others due to no or less mutual understanding. The perceived positive changes were due to having become more assertive, more open in expressing oneself due to experiencing less shame, and to be better able to enjoy life.
Post-intervention (n = 13)
As a general evaluation, 8 out of 13 participants (62%) reported that the intervention “met their expectations” fully or exceeded them. Five participants (38%) reported the intervention partly met their expectations, with the main feedback that they would have liked to receive more individual support during the intervention or had pending issues that were not covered in the intervention such as relationship issues. To the question “What has the intervention brought you thus far?,” the most prominent answers were related to the acknowledgment received from others about their suffering, recognizing yourself in stories of others, positively connecting with fellow AYAs, receiving practical advice about mental issues, feeling safe, and feeling listened to.
The average scores in Figure 2 represent “perceived quality of the intervention” on a 10-point scale. Most appreciated were the presence of nature, the appreciation of the location (the arboretum), the role of peer AYA cancer survivor, the quality of the trainers, and the content of the workshops.

Mean score and SD on 10 qualities of the intervention on a 10-point scale. SD, standard deviation.
Especially the session on the physical aspects of having had a traumatic experience due to surgery and facing a life-threatening disease, as well as the yoga sessions were most appreciated. As the least-appreciated session, the art workshops were mentioned by three participants, other participants either did not report anything or mentioned informal aspects of the program, such as daily walks or collective dinners. As a “suggestion for improvement” of the intervention, the majority of participants mentioned having more facilitators present for the possibility of one-on-one sessions, and more individual support during the group sessions.
Regarding the “perceived effect of the intervention on well-being and identity,” seven participants were fully positive (58%) about the intervention having contributed to development of their new post-cancer identity, whereas four said it partly did (33%) and one participant said it did not do so yet (8%). Participants reported that the intervention mainly helped them to realize that they already do what they would like to do (n = 2), to recognize that other AYA's are struggling and suffering as well due to the cancer experience (n = 3), and to realize that “it is not about returning to my ‘normal’ self, but about finding my new self” (n = 1). Practically, the participants mentioned that the moments of (self) reflection, the positive feedback received from other participants, and the experiential nature of the exercises contributed to the development of post-cancer identity. More specific aspects of the intervention that positively contributed to the promotion of well-being and identity development of the participants are shown in Table 3.
Frequency Table of Multiple-Choice Questions at Post-Intervention (n = 13)
Of the items on the “SRS”, the participants (n = 13) appreciated the relationship with the group and the facilitators throughout the week (7.7 cm; SD 2.16). The overall appreciation of the intervention and the participants' involvement scored second highest (7.3 cm; SD 2.24), followed by the extent to which the approach and methods were a fit with the participants (6.8 cm; SD 2.15) and the extent the goals and topics discussed during the week met the needs of the participants (6.4 cm; SD 2.16).
Follow-up (n = 9)
Seven participants (78%) still rated their “perceived experience of participation in the intervention” as positive, whereas 2 (22%) as negative. As “most appreciated aspects of the intervention” the good outline of the course in content and the beneficial aspect of the recognition and acknowledgment of the individual situation from fellow AYAs were described. The experienced new post-cancer identity was however mentioned only by two participants. The “least-appreciated aspects of the intervention” referred to not having experienced understanding from other participants as a consequence of having different needs than other participants. “Suggestions for improvement” mainly referred to having more facilitators present during the intervention, in line with the suggestions given at post-intervention.
Discussion
The intervention met the expectations of the participants to receive acknowledgment of their personal suffering due to the cancer experience, and to find recognition in the stories of the fellow AYAs. Finding acknowledgment and recognition are two fundamental aspects of recovery for AYAs and this is best found with fellow AYA cancer survivors in an intense intervention. Previous research confirmed that the connection with cancer-survivor peers is indeed very beneficial to the well-being of AYAs 36 and that they are in need of peer interactions and support that are meaningful and providing a sense of connection and belonging. 37
The group-based format seemed to be valuable for the majority of the participants. It was seen as especially beneficial to be together with peers outside the home setting. However, some participants profited less, as their individual psychological needs differed from those of the rest of the group. Nature was an element that was seen as beneficial for self-reflection and relaxation, in line with the existing literature findings on the benefits of nature.21,22
Participants reported that the workshops on trauma, cancer, and the nervous system, the yoga, and the nature-rich setting were most appreciated. This is in line with literature findings on the link between nervous system functioning post-cancer 38 and the positive effects of being in nature on the nervous system and cancer survival prognosis. 39 A meta-analyses on yoga has shown that it is associated with an increase in psychological well-being in healthy adults, 30 a reduction in distress, anxiety, depression, and fatigue, as well as increased quality of life, social and emotional functioning, and functional well-being in cancer patients and survivors. 28 Yoga has also been shown to be valuable in improving negative moods in patients suffering from breast cancer. 29 Yoga as part of an intervention, however, has to be respectfully adapted to the physical abilities and limitations of the AYAs for it to be beneficial.
The participants perceived the intervention as beneficial to the development of their post-cancer identity and aspects of well-being. These first results seem promising, however, it should be taken into consideration that the instruments used of post-cancer identity and well-being are limited as they have not been validated, were based on self-reported perception, and there was no long-term measurement. The longitudinal study on the effect of the intervention on well-being (as presented in a separate article) could give more substantial evidence to the effectiveness of the intervention.
A limitation of the intervention was the aftercare, as there was only an informal aftercare weekend, initiated and organized by the participants to offer peer support as aftercare. Not all participants were able to attend due to the travel distance. It is possible that the weeks after the intervention could be difficult for the participants because of the contrast between the supportive setting of the intervention and the home setting that could be more challenging with less understanding from the environment. Therefore, it would be beneficial if participants would be offered psychological support once back in their home environment. In future interventions, a component should be added on how to move on after the intervention, preparing participants on how to deal with possible issues at home, such as less understanding from their environment. This could be done by discussing all possible problems and pitfalls, and how to deal with them.
There were several methodological limitations to the study that could have created a bias in the results, especially since the sample size was rather small. First of all, the age range was relatively broad in the context of identity development, as younger and older participants find themselves in different phases of development. However, the intervention was aimed at (re)finding one's own unique post-cancer identity after the experience of cancer regardless of age, through a focus on individual character strengths and values. This could thus be a personalized approach that can be applied and be beneficial to AYA cancer survivors of any age. Anyhow, it might be even better to take the developmental stages of the AYA population into consideration to provide developmentally appropriate psychosocial care. 40 Second, the average time since completion of treatment was relatively high (4.5 years; SD 6.27) as psychological processes around the development of post-cancer identity could have been started. The average time of completion in this study was relatively biased due to the fact that one participant completed treatment 23 years before the intervention, at age 11, through which the average number and SD increased. This participant was strictly speaking not as an AYA, but was accepted to participate in the intervention as she expressed a strong need for it. Lastly, the participant group was relatively highly educated and consisted of mainly female participants. This could have biased the findings greatly as they may not be representative for the actual AYA population in the Netherlands and Flanders.
This research shows that AYAs could benefit from a peer-oriented one-retreat approach on their psychosocial recovery. As the results of this study give a first explorative insight into an intervention that targets post-cancer identity and well-being, further study into the specific elements of post-cancer identity and well-being is needed to identify what a post-cancer identity that promotes well-being exactly is comprised of, what its antecedents are, and its consequences. Future research could compare the intervention in a randomized controlled trial with an alternative intervention such as traditional individual psychological treatment at home, and a control group where AYAs do not receive an intervention but go on a 1-week, nonstructured vacation together.
Conclusions
To conclude, this first group-based positive psychology aftercare intervention in nature for oncology AYAs was well received by participants and provided useful feedback for improvement of future editions. The intervention could offer support to AYA's in the promotion of their well-being and post-cancer identity development, but more research is needed to confirm this.
Footnotes
Acknowledgments
The authors want to thank the Majin Foundation (Belgium) and the Anatta Foundation (the Netherlands) for the funding of our project, as well as the participants and the volunteers who helped with the intervention.
Ethical Approval
All procedures performed in our study were in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments. Informed consent was obtained from all individual participants included in the study. The study protocol was exempted from medical ethical review by the RUMC (the Netherlands).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The development and implementation of the intervention was funded by the Majin Foundation (Belgium) and the Anatta Foundation (the Netherlands).