
Abstract
The extent of Advance Care Planning (ACP) among Adolescent and Young Adult (AYA) cancer patients is not well characterized. This retrospective case note audit scrutinized the records of all AYA patients (aged 16–25 years) known to a regional specialist center in the United Kingdom, and who died between 2013 and 2019, for evidence of ACP. Eighty-four patients were included. ACP was identified for 67% of patients. Sixty-four percent expressed a preferred place of death; actual place of death reflected this in 65% of cases. Creation of a bespoke document may help to standardize ACP and improve end-of-life care.
Introduction
In the United Kingdom, patient experiences at the end-of-life are often wanting, especially with regard to discussing and planning death. 1 Since 2015, however, the National Institute for Health and Care Excellence (NICE) has produced guidance to drive improvement in end-of-life care for adult patients. 2 Most appropriately, there is an emphasis on communication, including a role for Advance Care Planning (ACP). This process includes allowing patients the opportunity to identify and express their preferences for care, particularly when approaching the close of life. ACP is thus widely recognized as a mechanism through which patients feel better supported and cared for at the end-of-life. 3
Adolescent and Young Adult (AYA; aged 16–25 years) cancer patients comprise a distinctive demographic whose priorities of care are not always congruent with those for older adults. Moreover, there is evidence to suggest that the needs of these patients in the final days of life are not being met. 4 To be sure, the issues faced by AYA patients are complex, with psychosocial, interpersonal, and developmental challenges not typically encountered by other patient populations.5,6 These, in turn, present difficulties for health care professionals involved in AYA patient care. Such individuals often receive minimal, if any, training to recognize and address these issues. 7
The plight of AYA patients can be confounded during their transition from pediatric to adult services when they are regularly confronted with a brand new health care environment and a clinical staff full of unfamiliar faces. Unsurprisingly, this disruption to care continuity can contribute to feelings of isolation and impact patient willingness to participate in difficult conversations with their care team. 8 Another confounder is the involvement of parents/guardians in the care of AYA patients, which can easily add another level of complexity. Many AYA patients are adults in the eyes of the law and, as such, are entitled to make their own decisions regarding their own health care provided, of course, that they have capacity to do so. The situation can become more challenging, however, when the wishes and preferences of parents/guardians differ from those of patients themselves. Health care professionals with clinical expertise may help to mitigate some of the tension between families in response to decision making, 9 again highlighting the importance of staff well acquainted with AYA patients and their experiences.
Input from palliative care services can greatly improve outcomes for AYA patients, their families, and the health professionals involved in their care. 10 Little is actually known, though, about the extent of ACP for this important patient group. 11 The care preferences of AYA patients at the end-of-life remain largely unidentified, particularly with respect to preferred place of death and level of involvement in decision making about care. This is despite evidence to suggest that AYA patients are motivated to make treatment and care decisions. 12
It is not known what the impact of any discordance between the preferences of AYA patients at the end-of-life and the services they actually receive would be. The need for better understanding of these issues is crucial. The aim of this study was to identify what ACP, if any, is recorded for AYA patients known to an AYA Regional Specialist Center (RSC) in Birmingham, United Kingdom. We also aimed to identify the health care professionals involved in these discussions and whether care preferences, such as place of death, were later fulfilled.
Methods
A retrospective case note audit was performed by H.M. Notes were read for all patients for the 6 months before their death. When data were uncertain, a discussion with coauthors was held. This project was approved by our Trust's Clinical Audit Registration and Management System, in line with appropriate Hospital Governance processes.
Eligibility criteria
All AYA cancer patients with confirmed hematological or oncological diagnoses and who had been referred to the multidisciplinary team of the West Midlands RSC at the Queen Elizabeth Hospital Birmingham were screened for participation in this study. The West Midlands RSC is one of only 17 such specialist centers in the United Kingdom. All cancer patients aged between 16 and 25 years at the start of treatment and who died from their disease between 2013 and 2019 were included in this study. Patients whose care was undertaken exclusively by pediatric services were excluded.
Template design
Parameters to be studied were selected by the research team based on relevant literature as well as clinical expertise and experience. These included evidence of ACP, palliative care referral, as well as preferred and actual place of death. For the purposes of this study, we agreed that ACP would be present if there was evidence that any discussion around end-of-life care took place with or without an explicit expression of preferred place of death. Data collected were entered into a Microsoft Excel spreadsheet for subsequent descriptive statistical analysis.
Results
Eighty-four AYA patients in total met the inclusion criteria. Their demographics are summarized in Table 1.
Summary Table of Demographics Collected from Patient Records
There was evidence that ACP was offered to 63 patients (75%, Fig. 1). For seven of these patients (8%) there was evidence that the topic had been raised, but that the patient declined to engage. In 11 cases (13%), ACP was not offered before death. In 10 cases (12%), the record was ambiguous (e.g., illegible). When they took place, ACP discussions were usually facilitated by an oncology or hematology doctor (34 patients, 61%). The next biggest group was specialist palliative care doctors or nurses who facilitated the ACP discussion for 13 patients (23%). Other health care professionals, including oncology clinical nurse specialists, discussed ACP with nine patients (16%).
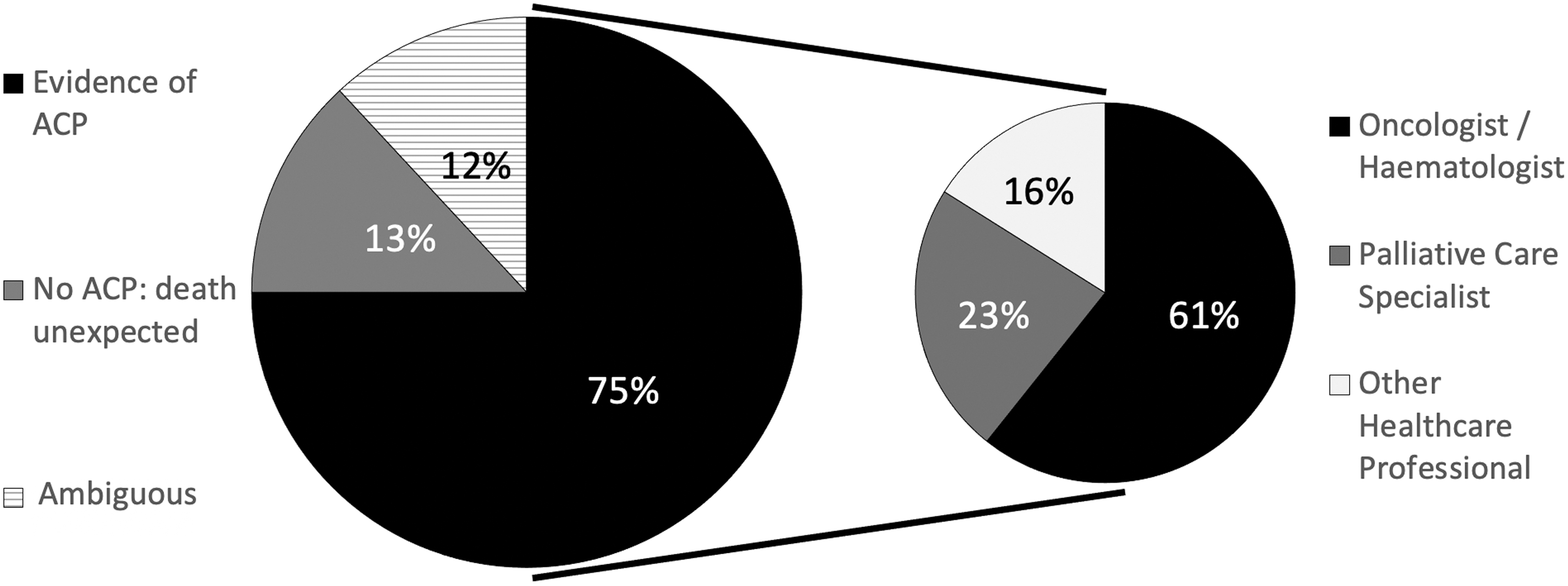
Evidence of end-of-life discussions with patients as recorded in the clinical notes. Pie chart on left shows percentages of patients who did/did not engage with the ACP process. Pie chart on right shows which health care professionals were primarily responsible for facilitating ACP discussions that took place and were documented. ACP, advance care planning.
For our study population a preferred place of death was recorded for 54 patients (64%). Of those patients who expressed a preferred place of death the most frequently expressed setting was home. This was the case for 34 patients (40%). Six patients (7%) expressed a preference to die in hospital and 14 patients (16%) wished to die in a hospice. A hospice in the United Kingdom is a specialist community palliative care unit; all the patients in the audit were eligible to access this care setting Regarding those patients who expressed a preferred place of death, 21 patients (39%) died at home, 9 patients (17%) died in hospice, and 24 patients (44%) died in hospital, usually on a dedicated AYA cancer unit. Overall, the actual place of death reflected the previously stated preference in 35 cases (65%) (Fig. 2).

Preferred and actual places of death for patients who previously expressed a preference. Vertical bars indicate the actual places of death for those patients who previously expressed a preferred place of death, as represented by the horizontal bars.
Sixty-five patients (77%) had a palliative care referral made on their behalf at some point during their disease trajectory. Twenty-seven referrals (42%) were made for symptom control, three (5%) for emotional support, and one (2%) for an end-of-life discussion. There was no documented reason for the referral to palliative care in 34 cases (51%).
Discussion
In this study, we sought to appraise the extent of ACP taking place among AYA patients and to determine which health care professionals were chiefly involved in this process. Given the observation that the median time between diagnosis and death for our cohort was <18 months, one could readily argue in support of a more urgent call for ACP in this patient population. Patient case notes were retrospectively scrutinized for evidence of these conversations. Our results are surprisingly encouraging. Although end-of-life discussions and preference for place of death were both recorded for only around two-thirds of all patients whose records we surveyed, there was, nevertheless, evidence that an additional fifth of all patients at least had the opportunity to engage with the process. For the remaining patients it is also still possible that some relevant discussions were had, but simply not documented.
Reasons for lack of ACP engagement are not straightforward, but may be linked to the challenges that health care professionals often feel are inherent in discussing death with younger patients. 13 This is despite evidence to suggest that AYA patients are both willing and able to participate in these conversations. 14 We note that our RSC does not presently make use of any standardized ACP document. Creation of such an instrument bespoke to AYA patients might well help to normalize the process and, in so doing, allow these patients to communicate their decisions with greater clarity and confidence. Enthusiasm for this, however, must be tempered with acknowledgement of the risk of transforming end-of-life discussions into tick-box exercises. 3 All patients, including the AYA group, should be empowered by ACP without risk to their sense of individuality.
End-of-life discussions in our study, when documented, were most often led by specialists in oncology or hematology as opposed to one in palliative care. This is consistent with the suggestion that members of the multidisciplinary team who are more acquainted with a patient are better positioned to discuss possible outcomes with him or her. 15 Palliative care specialists were involved with just under one quarter of the patients in this study who had ACP discussions. In contrast, the most common reason for referral to palliative care was for specialist symptom control. Unfortunately, though, the particular reason for referral was not specified in the patient's clinical notes in half the cases. Accordingly, it was difficult to ascertain the true nature of palliative care involvement with these patients. A more transparent noting system would help clarify the role for future referrals to palliative care and how this team might best be utilized.
Discussions about care preferences in the context of prognosis can be complex, challenging, and emotionally charged. These often span multiple conversations and it is not uncommon for multiple health care professionals to be involved. For this reason it can be argued that written communication becomes more important than ever to provide as much continuity of care as possible. The AYA years can be an awkward time for anyone, let alone a person with a life-limiting malignancy. This complexity is only magnified by the dynamic of the parent–patient relationship. Although it is entirely understandable why loving family would want to protect a patient from the harsh realities of their illness, they can nonetheless make it sometimes difficult to discern the voice of the patients from their well-meaning proxies. Given the differing levels of maturity and understanding within this patient group, it is imperative that the uniqueness of each patient be preserved and this needs to be reflected in ACP, too.
This study featured several limitations. First, we are reminded that, as the saying goes, absence of evidence is not evidence of absence. That is to say, the lack of ACP documentation does not, by extension, mean that such discussions did not take place at all. Moreover, entry into the medical notes is by no means a prerequisite for ACP. For example, it is far from certain whether any relevant discourse between the patient and their general practitioner (aka family physician) would be documented in the RSC notes. Future efforts may find it helpful to evaluate various facets of ACP separately to gain a more detailed understanding of the elements involved in this process. Teasing out the nuances, however, was beyond the scope of this study; for example, we did not collect specific information about proxy decision makers. It is also worth pointing out that our RSC has not adopted any systematic way of recording ACP discussions.
Limitations notwithstanding, our study represents, to our knowledge, one of the earliest methodical efforts of assessing for the presence of ACP in this important patient cohort. Previous studies have focused on other care settings with more extensive emphasis on decision making 5 We were able to formally collect data from all patients known to our AYA specialist team who died over a 6-year period. In doing so, we have created a baseline resource, which we anticipate shall stimulate further research to improve the service provided to our patients. It may be useful to explore whether an AYA-specific ACP document may help to facilitate ACP discussions with this patient population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.