
Abstract
This quality improvement initiative aimed to (1) explore the impact of adolescent and young adult (AYA)-specific navigation on attendance at a monthly peer support group for survivors aged 18–39 at a large comprehensive cancer center, and (2) better understanding attendees' preferences for group structure. Group attendance significantly increased following integration of AYA navigation. Using an online survey, we identified priority topics for discussion and desired changes to group organization, leading to modifications to group structure. Results highlight the value of having dedicated staff who proactively orient patients to resources tailored to their unique needs, and the importance of flexible program development that incorporates stakeholder input.
Introduction
After decades of stagnation, 1 the 5-year survival rate for adolescents and young adults (AYAs) diagnosed with cancer between the ages of 18 and 39 is improving. 2 As such, addressing survivorship concerns is increasingly critical to improving long-term outcomes among AYAs. Common life disruptions associated with cancer may be particularly distressing for AYAs, as cancer and its treatment can impede achievement of developmental milestones such as educational and professional accomplishment, establishment of romantic partnerships, financial independence, and family planning.3,4 This contributes to worse distress for AYAs relative to cancer survivors in other age cohorts and cancer-free AYAs.5–7
In response, there is a need for dedicated, age-specific services for AYAs.7–11 Social support is a known protective factor against distress12,13; however, among AYAs, cancer-related disruptions may decrease the size of existing social networks and limit the ability to develop new connections. Thus, peer support groups can be particularly beneficial for AYAs. Despite the benefits of support groups, 14 there are many barriers to participation. For example, referrals to AYA support groups are often unreliable, and AYA preferences for the structure of support groups are poorly understood. Patient navigation is one tool to facilitate appropriate delivery of care that has increasingly been used to support AYAs. 15 Patient navigators guide patients through the health care system, providing support through screening, diagnosis, treatment, and follow-up of a medical condition. 16 Patient navigation is especially critical for AYAs because, unlike other age cohorts, care for AYAs is often spread across pediatric- and adult-focused treatment settings, which can limit providers' knowledge of appropriate supportive resources. 17
To address this problem, the Robert H. Lurie Comprehensive Cancer Center (RHLCCC) of Northwestern University and Lurie Children's Hospital of Chicago (Lurie Children's) recently expanded their AYA-specific oncology services by integrating an AYA patient navigator (J.B.C.) tasked with identifying newly diagnosed AYAs, completing an initial biopsychosocial assessment, and orienting patients to supportive services. The AYA navigator also assumed responsibility for facilitating an ongoing monthly drop-in peer support group held at RHLCCC for AYAs at any point along the cancer trajectory. In addition to integrating AYA navigation, an AYA-specific program coordinator (B.F.) was also brought on to organize patient advisory boards, run the program's marketing and communications strategy, track program data, and help coordinate events. As part of a quality improvement initiative, we (1) assessed average attendance at the peer support group before and after integrating the AYA patient navigator to explore the impact of navigation services on support group participation, and (2) administered an online survey to better understand AYAs' preferences for the group.
Methods
Participants and setting
Participants were AYA cancer survivors who had previously expressed interest in learning about and/or participating in an established monthly drop-in peer support group for AYAs. To be eligible to attend the group individuals must be between 18 and 39 years old at the time of participation, have been diagnosed with any type of cancer between the ages of 15 and 39, and have received at least a portion of their cancer care at RHLCCC or Lurie Children's. The group is held one evening per month in a RHLCCC conference room on a floor shared with outpatient cancer clinics. Each group meeting lasts 90 minutes, with the first 30 minutes dedicated to a presentation from an invited speaker about topics relevant to AYAs, and the remaining 60 minutes dedicated to private open forum peer support discussion. The group is co-facilitated by the AYA patient navigator, who is a master's-level clinical social worker, and a doctoral-level clinical psychologist or another master's-level clinical social worker. Attendance at the group is recorded for routine clinical record keeping purposes.
Procedures
The AYA navigator was integrated into the clinical flow in July 2019, and an anonymous Qualtrics survey was administered by email in August 2019. The primary goal of the survey was to identify AYAs' preferences to inform modifications to the group design. Given that this project was a quality improvement initiative, it does not constitute human subjects research and therefore was not supervised by an Institutional Review Board.
Data analysis
To assess the impact of AYA patient navigation on group attendance, we used a Mann Whitney U test to compare attendance during the 6 months before integration of the AYA navigator versus the 6 months post-integration. Of note, this comparison did not evaluate the impact of changes made to the group as a result of the survey, as these changes were implemented more than 6 months after integration of AYA patient navigation. We used descriptive statistics to illustrate participants' satisfaction with the group, preferences regarding the group, and topics of interest. Supportive quotes are also presented.
Results
Impact of navigation on group participation
Average attendance was 4.83 participants (SD = 1.60) per month for the 6 months before integration and 13.00 participants (SD = 2.19) per month for the 6 months after integration (Fig. 1). A Mann Whitney U test indicated that attendance post-navigation (median = 4.00) was significantly higher than it was pre-navigation (median = 13.50, z = −2.94, p = 0.003).
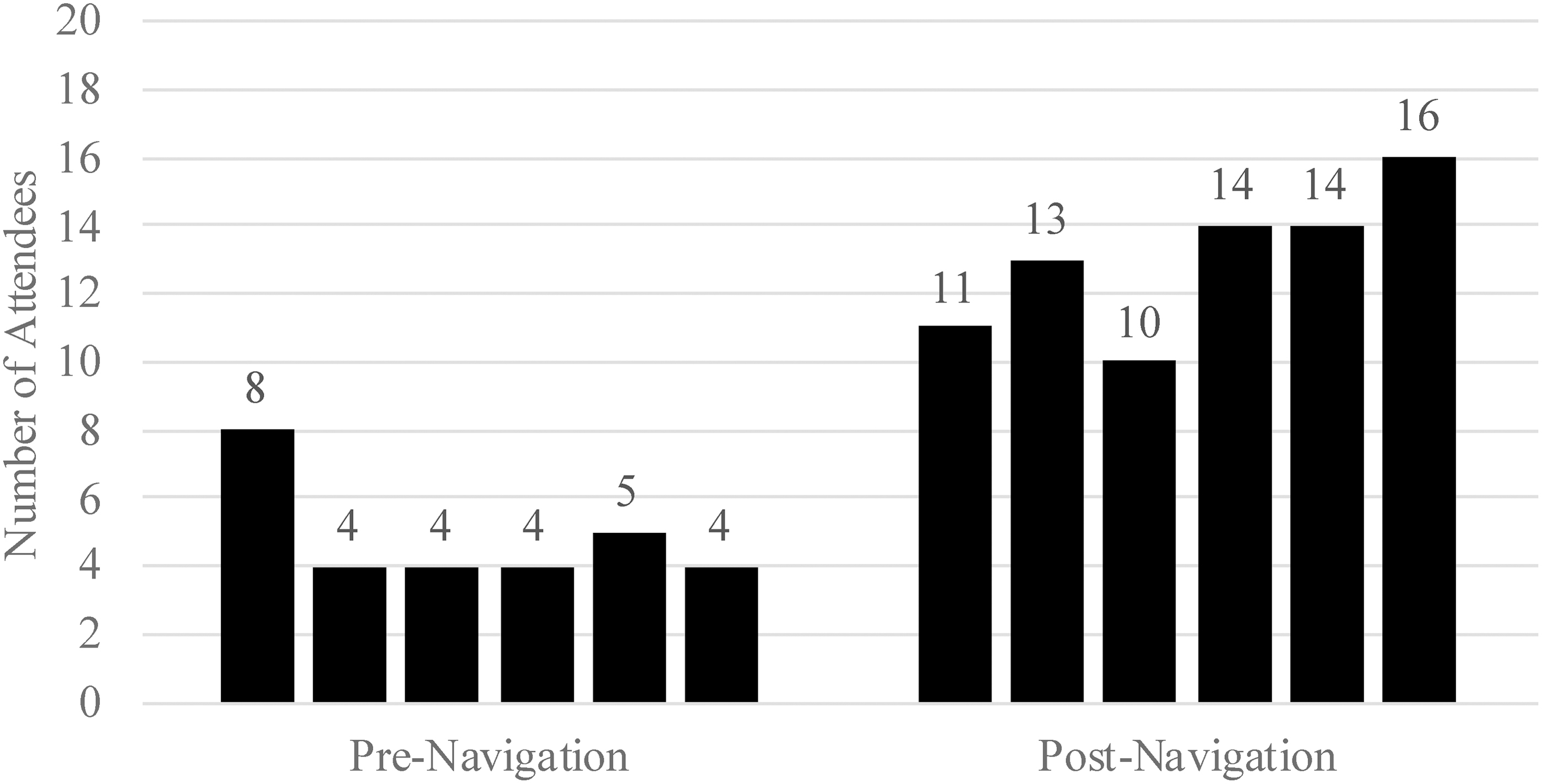
Support group attendance by month for the 6 months before and after integration of AYA patient navigation. AYA, adolescent and young adult.
Survey results
Thirty AYAs responded to the survey, although three only reported group attendance and did not answer subsequent questions. Sample characteristics are depicted in Table 1. Many participants did not provide sociodemographic information. Half of the sample was female (50.0%), and the majority attended the group regularly (33.3%) or inconsistently (40.0%).
Characteristics of Online Survey Respondents (N = 30)
n = 17.
n = 22.
Overall group satisfaction
Of the 22 participants who had ever attended a group meeting, the majority reported feeling very (45.5%) or moderately (27.3%) satisfied with the group, while 13.6% reported feeling neither satisfied nor dissatisfied. No participants endorsed feeling moderately or very dissatisfied. When asked what aspects of the group were most well liked, the most commonly endorsed responses were “Meeting people my age who can understand how I feel” (86.4%) and “Discussion of topics that pertain to me” (77.3%). For example, one participant's rationale for joining the group was “I needed to find a young adult support base because all other cancer groups were older people and did not understand.” All but one respondent reported that they would be very (63.6%) or somewhat (31.8%) likely to recommend the group to others. By contrast, the most commonly endorsed drawbacks to attending the group were costs associated with meeting in-person (e.g., commuting, 18.2%) and displeasure with the location of the meetings (13.6%). As one participant explained, “it would be nice to meet in other settings than the hospital, even if it's close by!” No participants agreed with the statement that the support group was unnecessary.
Preferences for group structure
When asked about incorporating caregivers into the support group, one-third of participants (33.3%) expressed interest while the remainder were unsure (30.0%), or would prefer not to bring a caregiver (23.3%). Of those who were interested, the majority (60.0%) expressed interest in developing a separate group for survivors and caregivers in addition to a group for survivors only.
Nearly half (46.7%) of the respondents reported appreciating a diverse format of group meetings. Particular interest was expressed in continuing the split format in which an invited speaker presents for part of the meeting and a private open discussion forum is held during the remainder. Only three respondents preferred either having a speaker with no open forum (n = 1) or having an open forum with no speaker (n = 2). Group members were most interested in hearing from a presenter every session (30.0%) or every other session (40.0%). With regard to the role of the facilitators, half (50.0%) of the respondents expressed interest in a mixed therapeutic-support group where facilitators provide emotional support, insights, and techniques for coping, while a focus is maintained on meeting other AYAs. Smaller proportions of respondents were interested in an exclusively therapeutic group (3.3%) or an exclusively peer support group (20.0%). Participants were most interested in holding meetings either once (43.3%) or twice (30.0%) per month.
Topics of interest
Participants were presented with a list of 37 topics relevant to AYAs and asked to identify all topics of interest (Table 2). The five topics most commonly endorsed were: body image and self-esteem (60%), intimacy and sexuality (60%), survivorship/finding a “new normal” (60%), diet and nutrition (56.5%), and self-care/taking better care of ourselves (56.5%). Participants also identified non-queried topics, including “scanxiety,” changes in relationships, survivors' guilt, and exercise.
Topics Queried in Online Survey
ADA, Americans with Disabilities Act; RHLCCC, Robert H. Lurie Comprehensive Cancer Center; SSDI, Social Security Disability Insurance; SSI, Supplemental Security Income.
Discussion
As part of a quality improvement initiative, our team evaluated the impact of AYA patient navigation on support group participation. We also administered an online survey to better understand AYAs' preferences for an ongoing monthly drop-in peer support group.
Regarding the first aim, results demonstrated that integration of AYA clinical navigation positively impacted group attendance. This is consistent with the broader literature linking patient navigation to increased health care utilization. 18 To participate in the AYA peer support group, AYAs must be aware of this service. The significant increase in support group participation that we observed after integrating an AYA patient navigator illustrates AYA survivors' desire to participate in such services, and it highlights the impact of having dedicated staff to proactively identify and orient patients to resources tailored to their unique needs. In addition, providing AYAs with an opportunity to develop a relationship with the group facilitator before first attending a meeting may increase AYAs' willingness to participate in the group.
Regarding the second aim, overall the group was evaluated highly by attendees, who expressed particular appreciation for the opportunity to meet other AYAs. Participants provided targeted feedback for improving the peer support group, and we have since modified the group design in direct response to this feedback. Specifically, we have formed an additional monthly group that is open to AYAs and a “plus one.” There are no limitations around the type of relationship a survivor must have with their “plus one.” This additional group follows a similar format to the survivors-only group, in which an invited speaker presents relevant resources for 30 minutes, and then a private open forum supportive discussion is held for 60 minutes. AYAs are invited to attend the survivors-only group, the survivors-plus one group, or both each month. In addition, changes were made in response to participants' expressed interest in diverse formats for group meetings. Every other month, the survivors-only group now dedicates the entire 90-minute meeting for open forum peer support discussion rather than having a speaker present at every meeting. Unfortunately, it was not possible to change the meeting location due to concerns with security and confidentiality. However, although a different location may be preferred, follow-up discussion with group members clarified that the environment is not a barrier to attendance.
In addition to discussing group structure, survey respondents identified priority topics to be addressed during meetings. Topics identified were consistent with previously reported patterns of unmet needs among AYAs. 19 This feedback has helped guide the search for speakers to present at the monthly meetings, ensuring that the content addressed is relevant for participants. It has also been incorporated into the open forum discussion part of the group meetings, as facilitators use this information to initiate conversations when group members do not raise topics on their own.
This study has limitations. Unassessed variables may have also contributed to the observed increase in support group attendance. In addition, it was not possible to account for potential confounding factors; therefore, results should be interpreted cautiously. Finally, survey results may have been influenced by selection bias.
In sum, through a quality improvement initiative we identified opportunities to enhance a monthly peer support group from the perspective of AYAs. Results led to the development of an additional monthly group that incorporates a plus one, an enhanced focus on AYA-identified priority topics, and increased opportunity for peer support by dedicating more meetings solely to open forum supportive discussion. This work was enabled by the integration of an AYA-specific patient navigator and an AYA-specific program coordinator, who spearheaded the quality improvement effort. Thus far, we have observed improved support group attendance simply through integration of AYA patient navigation. Future efforts will include re-evaluation of and iterative revisions to the support groups to ensure that they continue to meet AYAs' needs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The Northwestern Adolescent and Young Adult Cancer Program is funded in part by a partnership grant from Teen Cancer America.