
Abstract
Choriocarcinoma is an aggressive malignant trophoblastic neoplasm. The rapid growth of neoplastic tissue and myometrial invasion can cause uterine perforation. It is important to quickly diagnose the disease and plan treatment because these tumors are nearly always curable, and fertility can be preserved in most cases with proper management. The outbreak of novel coronavirus disease has affected the whole world since January 2019 and caused delays in treatment and follow-up of patients all over the world. In this study, we report a case of choriocarcinoma who postponed her admission to the hospital after diagnosis because she was afraid of the pandemic and lost her fertility due to uterine rupture and massive intra-abdominal hemorrhage.
Introduction
The COVID-19
Choriocarcinoma is a relatively rare and highly malignant variant of gestational trophoblastic neoplasia (GTN). It can occur after a molar pregnancy, abortion, term, and ectopic pregnancy. Proliferated fetal tissue in maternal tissues can be considered as a neoplastic allograft.
Choriocarcinoma tends to metastasize to the lung, vagina, pelvis, or liver in >50% of patients. Combination chemotherapy is the treatment of choice, and the prognosis for the disease is excellent after treatment. Surgical procedures might be necessary for chemoresistant patients or in emergencies due to bleeding.
This article aims to present a uterine rupture case due to delayed treatment in a patient diagnosed with choriocarcinoma during the COVID-19 pandemic.
Case Report
A 19-year-old gravida 2, parity 0 refugee woman who had previously been diagnosed with choriocarcinoma, was admitted to our emergency department with a vaginal bleeding complaint. Other vitals were stable upon examination, apart from mild tachycardia. All hematological tests were within normal limits. Beta human chorionic gonadotropin (βhCG) value was 21,005 IU/L.
Transvaginal ultrasound showed thickened heterogeneous endometrium measuring 22 mm with no vascularity. Evacuation curettage was performed with prediagnosis of abortion or mole pregnancy, and the patient was discharged from the hospital a day after. She was instructed to follow the pathology result.
Histopathological examination of curettage specimen and immunohistochemical staining revealed gestational choriocarcinoma. The patient did not come for control examination due to fear of COVID-19 transmission and could not be reached from the phone number in the hospital records.
Thirty-three days after the evacuation curettage, she applied to our outpatient clinic with mild vaginal hemorrhage. Ultrasound showed a grossly enlarged uterus with hypervascular miscellaneous echogenic shadows in the myometrium with signs of invasion to the serosa and bilateral ovarian enlargement. She had a βhCG value of 965,540 IU/L. Computed tomography scan excluded extrapelvic tumoral masses, and after the patient was stable, she was transferred to the medical oncology clinic for chemotherapy treatment.
The International Federation of Obstetrics and Gynecology (FIGO) grading and scoring were done, and one course of chemotherapy (etoposide 100 mg/m2 + cisplatin 20 mg/m2) was given to the patient. On the second day of chemotherapy, diffuse abdominal pain and uterine bleeding developed, and the patient was re-evaluated. Computed tomography images show intra-abdominal free fluid, bilateral theca lutein cysts, and an extremely heterogeneous uterus (Fig. 1). The patient had features of hypovolemia with anemia. She had received 2 U of blood transfusion.

Abdominal CT images show intra-abdominal free fluid, bilateral theca lutein cysts, and extremely heterogeneous uterus. CT, computed tomography; RO, right over.
The operation decision was made due to uterine rupture and abdominal hemorrhage. The patient was immediately prepared for surgery. First diagnostic laparoscopy was performed. There was a massive hemoperitoneum, two ovoid perforation areas in the anterior and posterior uterine corpus, and extreme bleeding from the uterus at the perforation site (Fig. 2). Bilateral ovaries were enlarged with multiple cystic lesions. Conversion to laparotomy decision was made. The abdomen was entered through a Pfannenstiel incision, and a total abdominal hysterectomy was carried out. The ruptured cysts in both ovaries were excised, and the remaining ovarian tissues were primary sutured. Intraoperatively 1 U of packed red blood cells and 2 U of fresh frozen plasma were transfused.
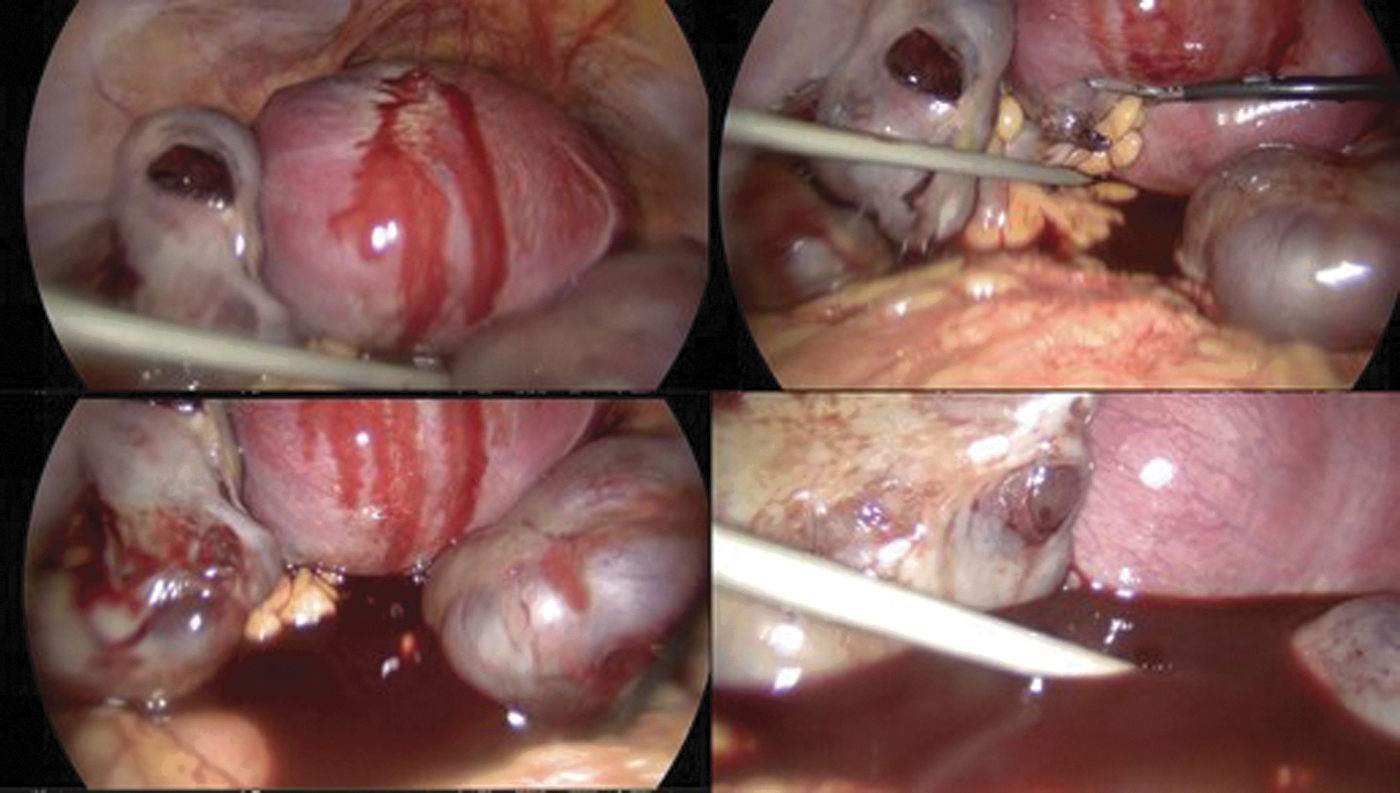
Uterine rupture areas and fragile ovaries are observed in the operation images.
During her postoperative period, the patient recovered well, and thereafter seven cycles of cisplatin+etoposide were given to the patient. Final βhCG value of the patient: 3.34 IU/L (Fig. 3).

Case report timeline. βhCG, beta human chorionic gonadotropin.
Discussion
Choriocarcinoma is a rare trophoblastic tumor, which was curable and may be developing after any gestational events. There are two forms of choriocarcinoma: gestational and nongestational. The former arises after a hydatidiform mole, normal pregnancy, or most commonly, abortion, whereas nongestational choriocarcinoma arises from pluripotent germ cells. 1 The majority of the gestational choriocarcinoma cases reported in the literature follow the diagnosis of a hydatidiform mole.
The diagnosis of a molar pregnancy might be suspected based on several clinical features: abnormal vaginal bleeding and uterus large for dates, pain from large benign theca-lutein cysts, and quantitative serum βhCG level is higher than expected, often exceeding 100,000 IU/L. 2 Histologically it includes areas of necrosis that show extensive infiltrative or destructive growth. The immunohistochemical markers hCG, cytokeratin, and inhibin are strongly stained in all trophoblasts. Ki-67 is widely expressed in about half of the cells. 3
In our case, she had vaginal bleeding and slightly elevated βhCG values (21,005 IU/L) during the first application and she had curettage for prediagnose of early pregnancy loss, and choriocarcinoma diagnosis made histopathologically.
Treatment of choriocarcinoma is done according to the stage of the disease and risk score. Early treatment is important because it is a rapidly spreading type of cancer.
The patient, in this case, is stage three due to lung metastasis. Also, the FIGO prognostic scoring of GTN is nine. Multiagent chemotherapy regimens are used for the treatment of high-risk GTN. The complete remission rate is about 85%. 4
According to published data, the primary treatment option is chemotherapy; surgical treatment may be required in massive hemorrhage, life-threatening conditions, and complications. Choriocarcinoma causing a uterine rupture and subsequent hemoperitoneum is rare, and the pathogenesis of uterine rupture in choriocarcinoma is unknown. The uterine vessels' invasion by malignant trophoblasts causes multiple infarctions due to thrombosis, vascular aneurysms, and intratumoral bleeding after vascular damage. 5 These pathologies seem to lead to uterine rupture.
COVID-19 pandemic made cancer treatment more difficult. It is necessary to balance treatment timing and protect social distance and care services against the pandemic's harms. As in this case, delaying in control examination in patients with fast-spreading cancer reduces the chance of treatment. Unfortunately, in our case, the fear created by the COVID-19 pandemic delayed the patient's access to treatment and caused a young patient to lose her reproductive ability.
During the COVID-19 pandemic, many patients, especially cancer patients, did not have their routine hospital checks out of fear of virus. This situation has brought about the problem of delayed diagnosis and treatment. Although the COVID-19 virus can be quite scary, we think that especially cancer patients should have their controls by taking the necessary precautions during the pandemic.
Footnotes
Author Disclosure Statement
All authors declare that they have no conflicts of interest.
Funding Information
There is no funding.