
Abstract
Purpose:
Receiving a cancer diagnosis for young people is likely to adversely impact the individual's quality of life. Mindfulness-based interventions (MBIs) are an emerging strategy used to improve psychosocial well-being. However, challenges have been reported in relation to adherence and accessibility of face-to-face mindfulness programs among young people. This study examined the feasibility and acceptability of a mindfulness-based interactive e-Book to improve psychosocial well-being of young people with cancer.
Methods:
Concurrent mixed methods approach with a pre-intervention-post-intervention survey and semistructured interviews evaluated the feasibility and acceptability of a MBI delivered over a 6-week period, and its effect on psychosocial well-being of young people with cancer 15 to 24 years of age.
Results:
Of the 31 young people, both survivors and on active treatment, enrolled in the study, 20 (64.5%) completed the post-intervention survey. Textual data and interviews (n = 3) revealed that young people enjoyed the intervention and found it useful and easy to navigate, but wanted more attention paid to cancer-specific stressors, as well as opportunities for face-to-face or online interactions. Psychosocial well-being measures demonstrated a statistically significant decrease in depressive symptoms (2.35 to 1.25, p = 0.03) and psychological distress (23.63 to 19.79, p = 0.03), along with nonsignificant increases in mindfulness (20.05 to 22.9, p = 0.08) and quality of life (62.0 to 69.1, p = 0.13).
Conclusion:
Young people found the self-help MBI, delivered in an interactive e-Book platform, useful and acceptable. There were psychosocial benefits, although recruitment and retention were study challenges and can be improved in future research.
Introduction
Every year, it is estimated that nearly 1 million adolescents and young people are diagnosed with cancer worldwide. 1 The World Health Organization defines young people as being between 10 and 24 years of age 2 and this age group has been extended to 29 years among young people with cancer.3,4 In addition to the emotional distress associated with adjusting to different phases of the cancer process (diagnosis/treatment/post-treatment), they are also subjected to unique challenges posed by the concurrent transition from adolescence into adulthood. 5 The dissonance between expectations of young people to form an independent identity during this period, and the reality of the return to increased dependence on their family and on the health care system, can cause conflicting emotions and negatively impact quality of life.5,6 It is well known that stress related to cancer negatively impacts quality of life and can cause depression.6–8 Studies have identified the need for psychosocial interventions to support the psychosocial well-being of young people with cancer.9–11
The benefits of mindfulness-based interventions (MBIs) in promoting well-being across age groups, including young people, are well established.4,12–16 Mindfulness is a state that can be achieved by acknowledging each moment as it passes by, and accepting the existence of emotions and feelings that accompany them. 17 By developing one's attentiveness to day-to-day experiences and encouraging an attitude of acceptance, individuals are better able to recognize their mental state and focus their energy toward the present as opposed to the past or future.16,18 Formal (e.g., body scan practices and sitting meditation) and informal (e.g., mindful eating and washing of dishes) mindfulness practices can be easily learned and practiced in day-to-day life. 19
Mindfulness interventions have demonstrated benefits in decreasing stress, anxiety, and depression among adults and children with chronic illness.14,20 Preliminary evidence suggests mindfulness can improve the well-being among young people with cancer.21,22 However, in-person, multiweek mindfulness programs have limited accessibility and low compliance among this population.4,13,15
Self-directed mindfulness workbooks have been reported to be feasible and accessible, and an effective alternative to face-to-face delivery of mindfulness interventions, 12 including among young people. 23 In addition, mindfulness interventions delivered digitally through video conferencing 21 or through a mobile application consisting of mindfulness audio exercises 24 have shown promise among young people. A study comparing the benefits of an in-person or e-health mindfulness intervention among adolescents with chronic medical conditions reported no difference in improved psychosocial outcomes. 25 Furthermore, self-help workbooks provide the foundations of the mind-body connection and provide opportunities for self-reflection and evaluation of learned mindfulness practice and skills. 26
An electronic version of a self-help book (e-Book) available through a digital platform, incorporating images, voices, and engaging activities, could be a convenient and inclusive delivery mode for young people with cancer. Review of the literature, to date, identified no study that evaluated the feasibility and usefulness of a self-help e-health mindfulness intervention among young people with cancer. Before designing a randomized control trial, it is important to explore the feasibility and acceptability of this intervention and its potential benefits for young people with cancer.
The aim of this study was to examine the feasibility (assessing retention and participation rate) and acceptability (through post-intervention feedback and one-on-one telephone interviews) of a mindfulness-based interactive e-Book and its preliminary effects (measuring mindfulness, quality-of-life, stress, and depression) among young people with cancer.
Methods
Design
This study used a concurrent mixed methods approach, 27 incorporating a pre-test-post-test survey and semi-structured interview, to evaluate if a mindfulness-based interactive e-Book was feasible, acceptable, and beneficial for young people with cancer. The study was approved by Western Sydney University Human Research Ethics Committee [H12783].
Participants and sample size
Eligibility criteria included young people who: (1) were between 14 and 29 years of age and (2) had a confirmed diagnosis of cancer (survivors or on active treatment). Sample size was calculated based on change in psychosocial functioning using mean change in scores on the Pediatric Quality of Life Inventory, 28 and the minimum sample size was 25 (effect size: 0.6, power: 0.8, alpha level: 0.05, and two tailed).
Intervention
The mindfulness-based e-Book was adapted from the book “Be Mindful and Stress Less: 50 Ways to Deal with Your (Crazy) Life” 29 and designed and delivered in a web-based interface platform “Kotobee Author” 30 to ensure it was accessible on mobile phones/tablets/computers. Modules focused on paying attention to the five senses and on self-care. The modules incorporated audios, reflection activities, and interactive quizzes, as described in Table 1. Previous researchers4,15,21,22 have reported that intensive, face-to-face mindfulness sessions were not feasible for young people with cancer, recommending limiting sessions to a maximum of six. Based on these previous findings, this study adapted the mindfulness-based book to be an interactive e-Book with six 1-hour modules comprising informal mindfulness-based practice.
Details of Mindfulness-Based e-Book
Measures
Pre-intervention measures
Demographic and clinical characteristics: Demographic characteristics included age, date of birth, gender, postcode, education, employment, and marital status. Clinical characteristics included age at initial cancer diagnosis, duration of treatment, and current treatment status.
Psychosocial measures:
Child and Adolescent Mindfulness Measure (CAMM) 31 : This 10-item tool is the most commonly used tool among young people with cancer. 4 It has been shown to possess good internal consistency (α = 0.84) and convergent validity.
i) Pediatric Quality-of-Life Inventory Cancer Module (PedsQL) 32 : This 27-item tool measures the health-related quality of life of teenagers and young adults with cancer. The PedsQL™ 3.0 Cancer Module possesses acceptable internal consistency (α = 0.81–0.98) for adolescents and young adults with cancer.
ii) Kessler 10-Item Psychological Distress Scale (K10)33,34: This scale measures psychological distress over the previous month and has been shown to be useful in capturing general distress and predictive distress in an Australian sample (n = 2967) of young people. 34 The K10 has high internal consistency (α = 0.93). 33
v) Patient Health Questionnaire-2 (PHQ-2) 35 : The PHQ-2 assesses the frequency of depressive symptoms over the past 2 weeks. This scale is known for its high diagnostic accuracy (87.2%), sensitivity (82.9%), and specificity (90.0%).
Post-intervention measures
Demographics: Participants were matched by collecting age, date of birth, and postcode.
Feasibility measures:
Retention rate: Retention rate was estimated by number of participants completing post-intervention measures.
Participation: Participating in at least 50% of the readings and activities in each module was considered the minimum expected for participation.
A question was asked “Were you able to engage in 50% of the weekly readings and activities” with a “yes” or “no” response.
Acceptability measures:
Post-intervention feedback survey: A satisfaction survey developed by the research team consisted of five items, including ease of navigation, meaningfulness, usefulness in improving general well-being, ability to gain mindful awareness, and whether the e-Book was challenging with a 4-point Likert-scale response ranging from agree completely to disagree with an option for open-ended response text.
nterviews: One-on-one semistructured interviews explored participants' experiences in using the e-Book. The interviewer asked questions about accessing and navigating the e-Book, usefulness of the e-Book and acceptability of the platform design and content. Interviews were conducted over the telephone and lasted 30–45 minutes in duration.
Psychosocial measures: Determined by comparing mindfulness, quality of life, stress, and depression by using the CAMM, PedsQL, K10, and PHQ-2 respectively.
Procedure
Recruitment took place between August and December 2019, through distribution of flyers on the Canteen (Australian Organization for Young People Living with Cancer 12–25 years) website, invitation emails to young people registered with Canteen, and advertisements on social media platforms (Twitter, Facebook, and LinkedIn). Young people were also encouraged to share information to their networks. Those who indicated interest in participating in the study were sent an email with a link directing them to the participant information sheet and the pre-intervention questionnaires for completion. All measures, including clinical characteristics, were self-reported and were administered using the Qualtrics survey platform. A list of free counseling services was provided in the participant information, should completion of any of the study questionnaires cause distress. Completion of the pre-intervention measures was deemed as consent to participate in the study as informed in the participant information sheet. Following completion of the pre-intervention questionnaires, participants were provided with access to the e-Book on mobile phones/tablets/computers and were encouraged to spend at least 1 hour per week on each of the six modules within the e-Book. Weekly reminders were sent either through email or as short message service (SMS). Following the 6-week intervention, participants were asked to complete post-intervention questionnaires, and asked if they would like to take part in an interview. Interviews were conducted on the telephone within 1 week of completing the post-intervention survey and written consent was obtained before each interview. Participants received a voucher for 60 Australian dollars to reimburse them for their time and internet costs.
Data analyses
Quantitative data in this study were analyzed using Statistical Package for the Social Sciences (SPSS) software package, Version 25. 36 Descriptive statistics were used to summarize the demographic and clinical characteristics of respondents, categorical variables were presented as frequency and percentages, and continuous variables were presented as mean and standard deviation. The distributions of the continuous variables were examined for normality using one-sample Kolmogorov-Smirnov test and Chi-Square test was conducted to examine for group differences between respondents and nonrespondents to post-intervention follow-up. Nonparametric-Wilcoxon Signed Rank test was used to examine for changes pre-mindfulness and post-mindfulness intervention. For changes in CAMM, PedsQL, PHQ-2, and K10 scores, effect sizes (Cohen's d) were computed, where values of 0.2, 0.5, and 0.8 were indicative of small, medium, and large effect sizes, respectively. 37
Semi-structured interviews and open-ended responses were supported by a topic guide and were audiotaped and transcribed verbatim. The interviews were thematically analyzed and followed the six-step process as described by Braun and Clarke 38 : (1) familiarization of the data by repeated reading of transcripts; (2) generation of initial codes; (3) examining codes to develop themes; (4) reviewing themes; (5) defining and naming themes; and (6) writing the report. An audit trail of the coding process is stored within Quirkos™ software. 39
Results
Participant characteristics
Among 31 participants enrolled in the study, the majority (61.3%) were female and 80.6% had completed cancer treatment. Table 2 provides comparative data of the demographic characteristics of participants.
Comparative Data of Demographic and Clinical Characteristics of Participants (n = 31)
Feasibility
Retention rate
Of the 31 participants who completed the pre-intervention questionnaire, 20 (64.5%) of them completed the post-intervention questionnaire and three young people participated in the interview. Eighty percent of those who completed the post-intervention survey were female. Computed Chi-Square test found that respondents and nonrespondents were comparable across gender (χ 2 = 0.22, p = 0.484), student status (χ 2 = 0.08, p = 0.53), marital status (χ 2 = 2.35, p = 0.12), and current treatment status (χ 2 = 0.02, p = 0.64). Further data analysis was performed to examine if there were differences in the psychosocial measures between participants who completed the post-intervention survey and those who did not and no statistically significant differences in mindfulness, depressive symptoms, stress, or quality of life were found.
Participation
The post-intervention survey revealed that most participants (90%) had accessed more than 50% of the e-Book.
Acceptability
Post-intervention survey results
All participants either completely or partly agreed that the e-Book was easy to navigate and meaningful, and improved their general well-being. One-fifth of the young people (20%) found the e-Book challenging (see details in Table 3).
Postintervention Survey (n = 20)
Qualitative results
Four themes were generated from both sets of qualitative data (open-ended responses and individual semi-structured interviews). The majority of the participants (65%) responded to the open-ended questions in the post-intervention feedback survey. These themes relate to the feasibility and accessibility of the e-Book, mode of delivery and presentation, perceived usefulness to self and others, and recommendations for improvement. See detailed description in Table 4.
Qualitative Data—Feasibility and Acceptability of the Mindfulness-Based e-Book
PAWS, paying attention with senses.
Psychosocial outcomes
Nonparametric Wilcoxon Signed Rank Test was conducted to compare the pre-mindfulness and post-mindfulness intervention across the psychosocial outcome measures, with Cohen's d calculated to examine the effect size. Findings revealed a significant decrease in depressive symptoms (p = 0.027) and stress (p = 0.028) with a moderate effect size (d = 0.53 and d = 0.5, respectively) in both areas (Fig. 1). Improvements in the mean scores for mindfulness (20.05 to 22.9, p = 0.079) and quality of life (62.0 to 69.1, p = 0.130) were noted, although the difference was not statistically significant.
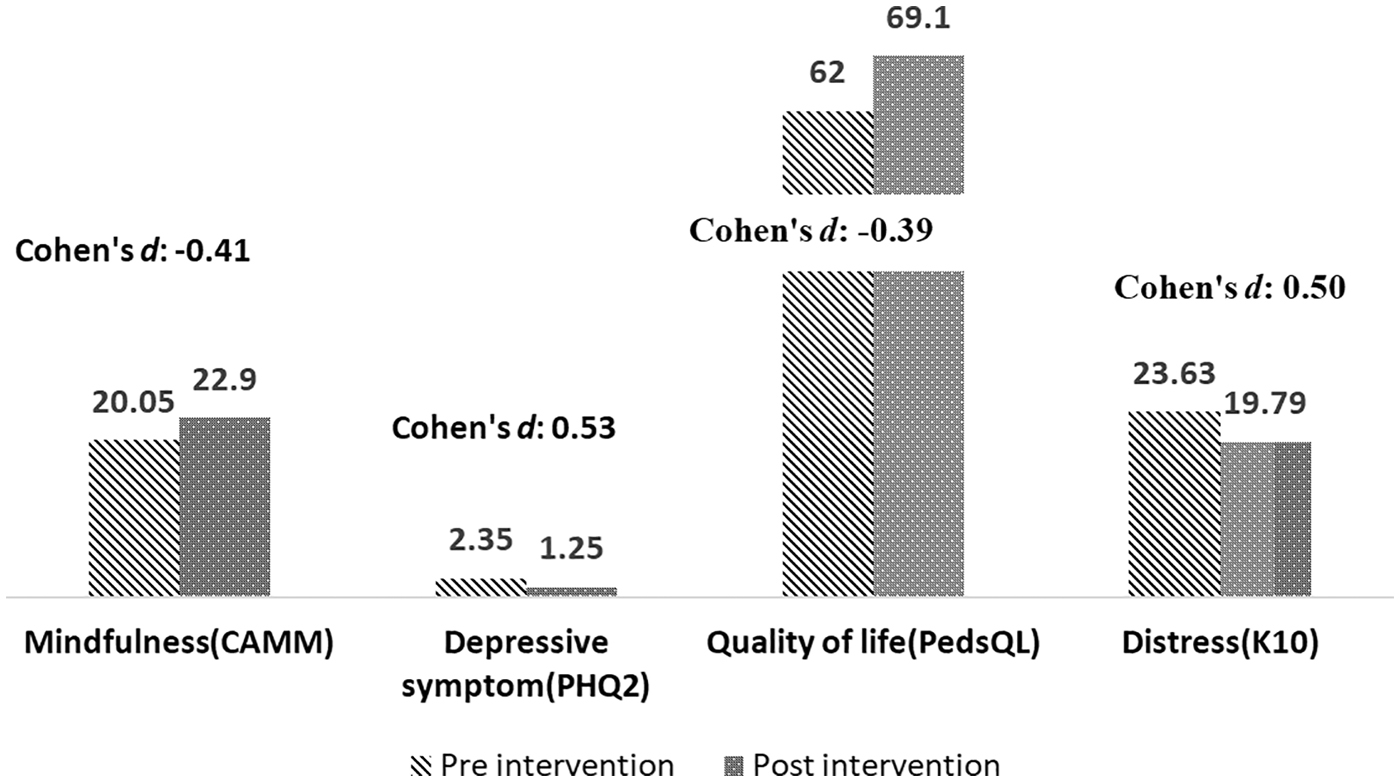
Pre-intervention and post-intervention mean and Cohen's d of the psychosocial outcomes. CAMM, Child and Adolescent Mindfulness Measure; K10, Kessler 10-Item Psychological Distress Scale; PHQ-2, Patient Health Questionnaire-2; PedsQL, Pediatric Quality-of-Life Inventory Cancer Module.
Discussion
This study assessed the feasibility, acceptability, and psychosocial outcomes of a mindfulness-based interactive e-Book and the potential benefits for psychosocial well-being, with young people who have cancer. Earlier studies have consistently reported low rates of enrolment and retention in psychological interventions for young people with cancer.4,15,22 However, the retention rate in our study was 64.5%, which is greater than the highest reported compliance rate of 61% in any digital health intervention among young people with cancer. 40 In addition our study supports the trend that female adolescents tend to self-select and engage in mindfulness interventions more than males. 41 Gender-specific mindfulness interventions could improve retention rates of young male participants. This study did not elicit the reasons for participant attrition. However, participants who dropped out did not differ with regard to their demographic characteristics and psychosocial measures to those who completed the study.
The majority of participants reported that they accessed and completed more than 50% of the e-Book and that they enjoyed participating in the interactive activities, which were integrated into the e-Book. Earlier studies4,15,21,24,42–44 identified that both nonclinical and clinical youth prefer to engage in brief interventions, which include multimedia components. Evidence suggests digital interventions with wide-scale implementation capability are currently not available. 40 The intervention in this study, which did not depend on hardware for deployment, demonstrated feasibility in delivery as most participants accessed more than half of the e-Book. While there are limited studies on psychosocial interventions involving young people in the active stage of cancer treatment, 40 we found that our e-Book was accessed by some young people receiving treatment (n = 4).
Earlier studies15,24,45 have recommended that mindfulness interventions should be tailored to cancer-specific needs. This study adapted a mindfulness workbook, which was intended to reduce stress and anxiety of young people with diverse needs. 29 While the post-intervention feedback survey and the qualitative interview data revealed the intervention was on the whole positive, in that it was accessible and easy to navigate and reduced rumination, some (20%) participants experienced challenges such as technical difficulties in navigating the e-Book, which they reported in the open-ended responses. The recommendations received from the young people were to supplement the e-Book with a hardcopy version and to include some face-to-face sessions. An alternate strategy could be the use of a blended delivery (online and face-to-face) with, for instance, a synchronous online orientation session to introduce the mindfulness concept followed by the e-Book. An online support platform connecting peers and guidance from an instructor may improve adherence to the mindfulness intervention as reported in a pilot study by Eysenbach G et al. 24
Initial psychosocial outcomes of the intervention were promising. The clinical benefits of the mindfulness-based e-Book revealed a significant reduction with moderate effect size in depressive symptoms and stress. These findings are in line with previous studies on the effects of MBIs for young people with cancer, who received a face-to-face 8-week intervention, 22 or alternatively, a videoconference intervention. 21 These positive benefits of a self-administered e-Book MBI are encouraging, considering the possibility of its wide reach and cost effectiveness, highlighting its feasibility as a support intervention for this vulnerable population. In addition, there have been no reported adverse effects among those using mindfulness interventions in nonclinical and clinical populations.
Limitations
Self-selected participants, the majority being survivors (off active treatment), and the small sample size for interview were the main limitations of this study. The majority of the participants was female; therefore, findings cannot be generalized to males. In addition, the psychosocial outcome results should be viewed with caution due to the lack of a control group. This feasibility study did not assess other contributing factors such as adherence in the use of the e-Book, duration of mindfulness practice, and the long-term impact of the intervention. We acknowledge that the workbook used in this study was not cancer specific, instead, it was designed for young people in general. Despite these limitations, this study adds to the paucity of literature evaluating the feasibility of a self-help mindfulness intervention for young people with cancer.
Conclusion
Young people found the self-help MBI, delivered in an interactive e-Book platform, useful and acceptable. There were potential short-term psychosocial benefits, notwithstanding recruitment and retention challenges. This study contributes further evidence demonstrating that young people were able to learn mindfulness skills using the e-Book, in the absence of an instructor or therapist, and enjoyed the flexibility of delivery through a digital platform.
Footnotes
Acknowledgments
The authors thank the young people who participated in this research.
Author Disclosure Statement
The e-Book referred to in this publication has been adapted from parts of Gina M Biegel's book, “Be Mindful & Stress Less: 50 ways to deal with your (crazy) life” for which Gina receives royalties from Shambhala Publications.
Funding Information
This study received early career researcher fellowship award from Western Sydney University (20341.87744).