
Abstract
Purpose:
A diagnosis of cancer often derails an individual's goals. The purpose of this mixed-methods analysis was to describe the evolution of adolescent and young adult (AYA)-reported goals in the year after a diagnosis of new or advanced cancer.
Methods:
As part of the Promoting Resilience in Stress Management (PRISM) phase 2 randomized controlled trial, AYAs with cancer (ages 12–25 years) were asked at baseline, 6 months, and 12 months: “Please give an example of a goal you hope to accomplish over the next month/year.” We used content analysis to categorize goals as follows: life milestones, physical health, mental/emotional health, cancer specific, and hobbies/interests. We summarized goal categories at each time point: for the entire cohort, by baseline diagnosis status (new vs. advanced cancer), treatment status (on-therapy vs. off-therapy), and baseline health-related quality of life (high vs. low).
Results:
Eighty-six participants completed the study and were included in the analysis (control: n = 41, PRISM: n = 45); 69 reported their goals at 6 months, and 54 at 12 months. Participants submitted a total of 169 goals at baseline, 148 at 6 months, and 126 at 12 months. At baseline, cancer-specific goals were most common for the short-term (35%), whereas milestone goals were most common for the long-term (46%). At 6 months, milestone goals were most common in both short- (38%) and long-term (51%) categories. A similar pattern was seen at 12 months.
Conclusion:
AYAs' goals change over the first year of their cancer experience, with a shift in short-term goals from cancer-specific goals at baseline to milestone goals at later time points. ClinicalTrials.gov (NCT02340884).
Background
Adolescent and young adults (AYAs) diagnosed with cancer face higher degrees of psychological distress than individuals diagnosed at other ages.1,2 One possible explanation for this difference may be that a diagnosis of cancer during this time interferes with the defining features of adolescence and early adulthood in a way that is developmentally unique. For example, typical adolescence and young adulthood is marked by the development of self-identity and autonomy from one's family. 3 The AYA with cancer must develop their sense of self while grappling with physical changes from their cancer, enduring disruptions to education, and facing mortality.1,4 Whereas many of their peers are moving out of their parent's homes and establishing financial independence, the AYA with cancer may have to relinquish autonomy and rely on parents to help with basic self-care. 4
Learning to set high-quality, achievable goals in the wake of a cancer diagnosis is thought to facilitate adaptation to illness and predicts higher quality of life in adults with cancer.5,6 Moreover, goal setting is a teachable skill that can be used to fortify resilience. 7 Particularly relevant in adolescence and young adulthood, refining goal-setting skills may help AYAs with cancer to achieve critical developmental milestones.8,9 Similar to their healthy peers, AYAs with cancer prioritize goals that maintain “normalcy.” 10 However, to tailor psychosocial care to the unique developmental needs of AYAs, we need to understand what influences goal setting in this group.
Promoting Resilience in Stress Management (PRISM) is a brief skill-building intervention designed for the specific needs of AYAs with cancer.11,12 The intervention includes a module dedicated to setting goals that are specific, measurable, and realistic. 11 Although PRISM demonstrated measurable benefit in other adaptive coping skills, previous analyses did not detect a measurable change in goal-setting skills compared with the control group. 13 Two limitations of that analysis were that neither subtle nuances in goal quality/content nor the influence of patient-specific factors could be examined. 13 The aim of this post hoc mixed-method analysis was to characterize the evolution of AYAs' goals in the year following their cancer diagnosis or relapse. As the intervention did not impact reported goals, we pooled both randomization groups into a single cohort. Because it is likely that goals are highly dependent on patient-specific factors, 10 subgroup analyses explored the role of disease status, treatment status, and health-related quality of life (HRQOL) on goal category.
Methods
Design, setting, and participants
The phase 2 PRISM randomized controlled trial (RCT) was completed at Seattle Children's Hospital. 11 Eligible participants were English-speaking AYAs (ages 12–25 years). Participants either had a new diagnosis of cancer (diagnosed between 1 and 10 weeks before enrollment) or advanced cancer (defined as relapsed, refractory, or progressive disease at any time since initial diagnosis) and were being treated with chemotherapy at Seattle Children's Hospital. Individuals unable to cognitively participate in the intervention were excluded from the study. Approval was obtained by the local Institutional Review Board. This trial was registered at ClinicalTrials.gov (NCT02340884).
The primary outcome of interest for this phase 2 RCT was self-reported resilience at the 6-month time point.11,12 Results from the primary and secondary outcome analyses, including HRQOL were previously published.11–15 For this planned secondary analysis, we report the qualitative analysis of AYA-reported goals over time.
Recruitment and randomization
The recruitment and randomization procedures for this study were previously reported. 11 In brief, study staff identified potential eligible participants by chart review. The Principal Investigator (A.R.R.) confirmed eligibility (criteria listed in section “Design, Setting, and Participants”). Participants 18 years of age or older provided written informed consent. Participants younger than 18 years of age at time of enrollment provided written assent and parental or guardian written informed consent was obtained. Participants were enrolled and then randomized one to one to either usual care (control arm) or usual care plus PRISM (intervention arm). Randomization was stratified by age (12–17 and 18–25 years).
Intervention
PRISM is a skills-building intervention for AYAs with serious chronic or life-threatening diseases and is based on theories of resilience, stress, and coping.11,12 College-educated interventionists (“coaches”) receive at least 8 hours of in-person instruction on intervention content and delivery.11,12 PRISM is delivered in four, 30–60 minute one-on-one sessions scheduled approximately every other week. Sessions focus on stress management, goal setting, cognitive reframing, and meaning making. In an optional fifth session, AYAs may review intervention skills in a facilitated family meeting. Intervention feasibility, acceptability, and efficacy are described elsewhere.11,12 Usual care at Seattle Children's Hospital includes a comprehensive psychosocial evaluation completed by a clinical social worker at the time of initial diagnosis. Subsequent psychosocial evaluations are completed upon family request or staff referral.
Procedures
All participants completed the Resilience in Pediatric Cancer Assessment within 4 weeks of enrollment (baseline) and then 6 and 12 months later. 11 This battery included age-validated patient-reported outcome measures of HRQOL and open-ended questions inquiring about the individual's goals. Reminders to complete surveys at each due date were provided by study staff weekly for up to 3 weeks for any survey not returned. If a survey was not returned within 12 weeks of the due date, it was considered missing. Gift cards were given to participants after completion of assessments ($25 for the baseline assessment, $50 for the 6- and 12-month assessments).
Study surveys
Participants completed comprehensive surveys consisting of validated instruments and two open-ended questions. 11 The aim of these questions was to compare the learned skills of concrete goal setting between participants randomized to PRISM versus usual care. The first question inquired about “short-term” goals for the next month (“Please give an example of a goal you hope to accomplish over the next month”). The second question inquired about “long-term” goals for the next year (“Please give an example of a goal you hope to accomplish in the next year”). The participant could submit one response to each question, identifying one short-term goal and one long-term goal at each of the three time points.
HRQOL was evaluated using the Pediatric Quality of Life Inventory (PedsQL).16–19 This library of measures is valid and reliable in AYAs with cancer and has been used in clinical research with good acceptability and minimal missing data. The PedsQL 4.0 Generic Core Scale is a 23-item measure of general wellbeing and includes physical, social, emotional, and school domains.17–19 The abbreviated 15-item version of this instrument (PedsQL SF-15) was used in this study to minimize survey burden. The abbreviated version omits questions pertaining to pain, fatigue, insomnia, and activities of daily living. Psychometric properties of the 23-item and 15-item instruments are equivalent. 20 Each item was rated on a five-point Likert Scale. Domain-specific and total scores are transformed to a 0 to 100-point scale, with higher scores representing better HRQOL.16,18,19 Among healthy adolescents and adolescents with cancer, the Generic Core Scale total score internal consistency was 0.92.16–19,21 Subdomain internal consistency ranged from 0.75 to 0.88.16,18,19 The minimal clinically important difference for the PedsQL 4.0 Generic Core Scale was estimated to be 4.4 points for the total score and 6.6–6.9 points for subdomain scores.18,19
Statistical methods
Qualitative analysis
The Standards for Reporting Qualitative Research guidelines were used to guide data collection and analysis. 22 Written responses to goal questions were transcribed verbatim, de-identified, blinded of randomization assignment, randomly resequenced, and entered into a new database for coding. Three study team members trained in qualitative methods scored each patient-reported entry as previously reported. 13 These reviewers (K.S.B., a senior health services researcher with no professional interactions with participants, Nicole Sherr, MS, a research associate who interacted professionally with participants, and A.R.R., a pediatric oncology/palliative care physician who interacted professionally with participants) further analyzed the goal responses using conventional content analysis. First, the primary reviewer (K.S.B.) used open coding to develop the following categories for both short- and long-term goals: physical health/sports, mental health, educational, cancer specific, life milestones, hobbies/interests, and other.9,10,23,24 These categories were reviewed and confirmed with the other two reviewers (N.S., A.R.R.).
The categories were iteratively revised with final consensus to include the following categories: (i) life milestone goals pertaining to an action or event marking a significant change or major step toward independence (educational, vocational, or otherwise); (ii) physical health goals pertaining to an improvement in physical health or a specific activity (including sports) that is not clearly directly related to cancer; (iii) mental/emotional health goals pertaining to psychological or emotional wellbeing, including relationships with family or peers; (iv) cancer-specific goals pertaining to treatment or recovery, specific to the cancer experience; and (v) hobby/interest goals pertaining to nonsports activities performed for pleasure or learning that is not related to formal education (Table 1). Rules and definitions were determined by the primary reviewer (K.S.B.) and iteratively refined throughout the process. Focused coding was completed; each reviewer independently assigned each response to a goal category. If a response was considered to have multiple goals, either the first goal was coded or an overarching goal summarizing one common goal was coded so that each goal was only assigned one category. The primary reviewer (K.S.B.) combined the results of all the reviewers' goal categorization. Discrepancies were reviewed and reconciled.
Thematic Goal Categories
Quantitative analysis
We summarized goal categories at each time point using frequencies and percentages for the entire cohort. Short-term goals (for the next month) and long-term goals (for the next year) were examined separately. We also summarized goal categories at each time point using the following subgroups: baseline diagnosis status (new diagnosis vs. advanced cancer), treatment status at 6 and 12 months (on therapy vs. off-therapy), and baseline HRQOL (high vs. low). A PedsQL score of 70 was used as the cut point delineating high versus low HRQOL, using previously established guidelines.16,25,26 Because study arm previously did not show a difference in goal setting, this subgroup was not included in the present analysis. 13 For this exploratory, post hoc analysis, we chose to present results graphically and using descriptive statistics rather than perform hypothesis testing.
Results
In total, 100 participants were enrolled and randomized (control: n = 50, PRISM: n = 49) (Table 2). One participant was excluded following randomization for not meeting inclusion criteria (not fluent in written English). A total of 86 participants completed the entire baseline survey and were included in the present analysis (control: n = 41, PRISM: n = 45). Of these, 69 (80%) completed surveys at 6 months, and 54 (63%) completed surveys at 12 months. A slight majority of study participants were male (57%). Most participants were between 12 and 17 years old (71%), Caucasian (64%), and had new diagnoses of cancer (73%). Leukemia/lymphoma was the most common cancer type (66%). Participants submitted a total of 169 goals at baseline, 148 at the 6-month time point, and 126 at the 12-month time point.
Baseline Characteristics of Participants Who Completed Assessments at Time of Enrollment, Six-Months, and Twelve-Months
PRISM, Promoting Resilience in Stress Management.
At baseline and when thinking about the next month (short-term goals), AYAs most commonly reported cancer-specific goals (35%) (Fig. 1). Short-term cancer-specific goals included “recover from surgery,” “get discharged,” and “take less narcotic pain medications.” Physical health goals unrelated to cancer were the second most commonly reported short-term goal category at baseline (23%). These included “shoot hoops,” “exercise more,” and “eat healthy.” Milestone goals were the third most common short-term goal category at baseline (20%). Most milestone goals were subcategorized as educational goals (n = 15), including “staying on track with school” and “doing well in/pass” a certain class. Mental/emotional health goals were the least commonly reported short-term goals (8%) and were primarily focused on “staying positive.”
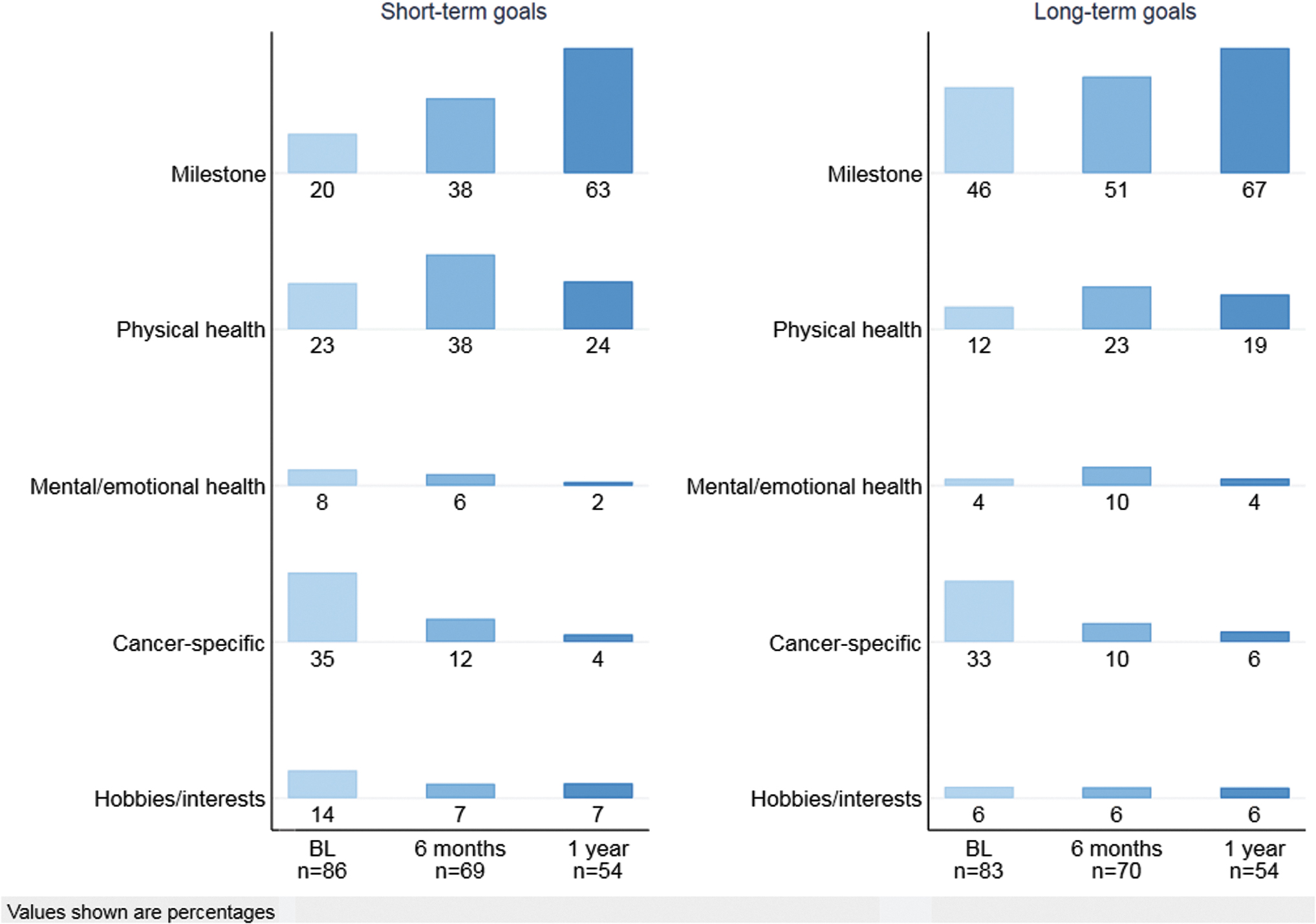
Short- and long-term goal categories by time point.
In contrast, at baseline and when looking ahead to the next year (long-term goals), AYAs most commonly reported goals in the milestone category (46%), such as “starting a company,” “graduating,” “going to college,” and “moving out” of their parents' home. This was followed by cancer-specific goals (33%) and physical health goals (12%), which were similar in content to the short-term goals.
At the 6-month study time point, short-term goals shifted from cancer-specific goals (12%) to milestone goals and physical health goals (38% for each). Educational goals remained the most common milestone subcategory (n = 20); “graduating” was the most common goal reported (n = 15). Most physical health goals focused on “losing weight,” “eating healthier,” “getting in shape,” and “increasing endurance/activity.” Milestone goals remained the most commonly reported long-term goals (51%) at 6 months, followed by physical health goals (23%), cancer-specific goals (10%), and mental/emotional health goals (10%).
At the 12-month study time point, the majority of both short-term and long-term goals were categorized as milestone goals (n = 78; short-term: 63%, long-term: 67%). Educational goals remained the most common subcategory (short-term: n = 25, long-term: n = 29), including “graduating” and “doing well in school.” Vocational goals and other goals focused on achieving independence (e.g., “find a place to live,” “getting a driver's license”) became more numerous (n = 13). Physical health remained the second most commonly reported goal category, representing 24% of short-term and 19% of long-term goals. Only 4% of short-term goals and 6% of long-term goals were categorized as cancer-specific goals at 12 months.
In subgroup analyses, AYAs with high HRQOL most commonly identified milestone goals (32%) in the short term (Fig. 2). In contrast, AYAs with low HRQOL most commonly reported cancer-specific goals (38%) in the short term. Over time, short-term goals for both groups became predominantly focused on milestones (12 months: high HRQOL: 62%, low HRQOL: 64%). Regardless of the AYA's disease status (Supplementary Fig. S1, new diagnosis vs. advanced cancer) or treatment status (Supplementary Fig. S2, on- vs. off-therapy), there was a shift in short-term goals over the 12-month study period from cancer-specific goals to milestone goals. Across all time points, milestone goals were the most commonly reported long-term goal category regardless of HRQOL, disease status, or treatment status group.

Short- and long-term goal categories by baseline quality of life.
Discussion
In this mixed-methods secondary analysis of the phase 2 PRISM RCT in AYAs with cancer, we found that the focus of short-term goals changed over time, such that physical health and cancer goals became less common and milestone goals became more common. Of the patient-specific factors examined, only baseline HRQOL demonstrated a difference in short-term goal prioritization, where AYAs with poorer HRQOL focused on cancer-specific goals, and those with better HRQOL focused on life milestones. At all time points, AYAs reported long-term goals focused on milestones, regardless of HRQOL score, treatment status, or diagnosis status.
Other studies described the impact of goals among patients with cancer. However, the evolution of goal patterns over time is limited to adults. In adults with colorectal cancer, social-oriented goals (e.g., spending time with family or friends) tend to predominate at diagnosis and physical-oriented goals predominate 6 months later. 23 This pattern is thought to reflect an alignment of goals with patients' present situation, perhaps to preserve wellbeing.6,23 How this framework applies to the developmentally relevant priorities in AYAs is unclear. This population may endorse different needs, and thus different goals. A key developmental need among adolescents, for example, is to “fit in” among peers; thus, AYAs with chronic illness may prioritize developmentally typical goals over specific physical health needs.10,27 Both well adolescents and those with cancer report similar academic, leisure, and interpersonal goals. 9 Similarly, we found high proportions of milestone-oriented goals (e.g., graduating or getting a job) at all time points, especially pertaining to long-term goals. However, a greater proportion of adolescents with cancer also report health-related goals and most identify a new goal because of their cancer. 9 Likewise, we saw high proportions of short-term cancer-specific goals and noncancer-related physical health goals at baseline. Health-related goals and goals with concrete, shorter term (and thus achievable) timelines are associated with positive coping. 8 Our findings suggest that AYAs may focus on concrete, physical health goals for the short-term to cope with initial changes in their health status, yet remain focused on long-term developmentally typical goals to preserve normalcy. Moreover, maintaining life-milestone goals, even if infeasible, may be a product of maintaining hope and, thus, reflect positive coping.28,29 Over time, and as the AYA adjusts to their illness, short-term goals become focused on developmentally typical milestone goals.
Illness-related factors influence the goals we set and how we attempt to achieve them.23,30 In this study, baseline HRQOL seemed to influence the prioritization of short-term goals, whereas treatment and disease status did not. This makes sense; HRQOL is determined by the presence and severity of symptoms. 26 Patients with poorly controlled symptoms may only be able to focus on goals that address their immediate physical needs. 31 Addressing symptoms must be the first priority of clinicians; only after symptoms are addressed may AYAs start to set other short- and long-term goals, including those that direct them toward meaningful life milestones.
This analysis has several limitations. Primarily, in this post hoc analysis, we have limited power to detect differences, especially in subgroup analyses. Because of the exploratory intent of the analysis, we elected to omit hypothesis testing. Second, because of the nature of the qualitative data collection, we have access to limited detail in goal content. We were unable to clarify ambiguous goals or query secondary goals. Participants often wrote only single phrases or sentences; we were unable to capture complex goals, steps toward their achievement, their relative feasibility for clinical status. 13 Together, this approach may have resulted in goal category misclassification. Third, we observed attrition over the 12-month study period, primarily owing to disease progression and death. 11 As a result, the experience of participants who are most critically ill is not represented. If we assume these patients have worse symptom burden and corresponding poorer HRQOL, and that poorer HRQOL influences immediate goals, we might also assume that these patients did not have the same evolution in goals over time. Rather than shift from cancer-specific to milestone goals, these patients may have remained focused on cancer-specific goals relevant to their symptoms. Finally, the larger clinical trial was conducted at a single pediatric institution and was limited to English-speaking participants. Results may not reflect the cancer experience of all AYAs.
The priority of goals in AYAs with cancer appears to evolve during the course of their disease trajectory. Early in the experience, whether following a new diagnosis or a recent relapse, many AYAs endorse goals specific to their cancer diagnosis. As time goes on, and perhaps as AYAs adapt to their illness and their symptoms improve, developmentally typical milestones seem to be prioritized. Ultimately, understanding how priorities evolve with time may help to risk-stratify psychosocial care, leading to better patient-centered care in AYAs with cancer.
Footnotes
Acknowledgment
The authors acknowledge Nicole Sherr, MS for her contribution to the analysis.
Disclaimer
The data used for this secondary analysis were collected as secondary outcomes for a randomized controlled trial.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded through grants from the National Institutes of Health (KL2TR000421) and CureSearch for Children's Cancer, both awarded to A.R.R. This work was conducted through a T32 Training Grant (5T32CA009351-40) and the St. Baldrick's Foundation, both awarded to A.S.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.