
Abstract
Purpose:
To descriptively explore semen quality among Indian men with various types of malignancies. We evaluated semen parameters of male patients referred to our hospital before commencing their cancer treatment.
Methods:
Four hundred sixty-one male patients who were within the age range of 15–50 years were recruited with diagnosed malignancies. Pre-treatment semen analyses were performed on these patients to collect data on the volume, sperm concentration, motility, and normal forms (morphology). These semen parameters were compared between cancer groups (testicular cancer, hematological cancer, and other cancers). Further comparisons were also drawn to World Health Organization (WHO) semen parameter levels (2010, fifth edition) for normal outcomes.
Results:
There were no notable variations observed in semen volume (mL) and progressive motility (%) between cancer groups. These parameters were within the WHO normal semen criteria. Differences in normal forms (%) between cancer groups were not observed either; however, they were marginally lower compared with the WHO criteria. Sperm concentration was evidently lower in testicular cancer 34 × 106/mL (IQR: 10.1–60 × 106/mL) compared with hematological cancers 66 × 106/mL (IQR: 23–84.21 × 106/mL) and other cancers (IQR: 27–86.3 × 106/mL). Testicular cancer patients also presented with the largest semen disorder diagnosis (Asthenozoospermia, Oligoasthenozoospermia, Oligozoospermia, and Azoospermia) compared with two other groups.
Conclusion:
Males with testicular cancer have shown to have lower semen quality between cancer groups and compared with WHO criteria, increasing their likelihood of them being infertile. This study further allows us to understand these outcomes, particularly in the Indian subpopulation, propagating changes in guidelines in oncofertility and medical counseling.
Clinical Trials Registry—India number: CTRI/2020/09/027720
Introduction
The estimated number of people living with cancer in India is 2.5 million.1,2 Cancer treatments have radically improved. With major advancements in diagnostic modalities and cancer therapies, the 5-year survival rates in young males of reproductive age (14–35 years) 3 diagnosed with cancer has increased dramatically. 1
Common diagnosed cancers in male patients of reproductive age are leukemia, Hodgkin lymphomas, and testicular tumors. 4 For some cancers, particularly those who are diagnosed with germ cell tumors, it has been reported that sperm quality may be compromised unrelated to cancer treatment. 5 Three quarters of cancer patients, before starting their treatment, may have poor baseline spermatogenesis.5–7 Chung et al. reported that a cancer diagnosis can interfere with endocrine and immunological function, thereby disrupting spermatogenesis, which may be cause for infertility before treatment. 8 It has also been reported that testicular cancer and Hodgkin disease have poorer reproductive outcomes. 8 Twenty-eight percent of male patients with a testicular cancer and 25% diagnosed with Hodgkin lymphoma are found to have oligozoospermia before treatment.9,10 In some studies it has been found that 47%–67% of patients with Hodgkin disease will present with poor sperm quality before treatment.10,11
Poor spermatogenesis can be confirmed by taking a patient's medical history of whether they have been previously diagnosed with cryptorchidism, antisperm antibodies, possible contralateral or intraepithelial germ cell neoplasia, and generalized stress associated with illness.5,12,13 Furthermore, 12% of male patients will not have viable spermatozoa at the time of freezing a semen sample before the start of cancer therapy. 14 Hence, the importance of adhering to international guidelines to offer the patient a timely referral for fertility preservation before cancer treatment for discussions around fertility preservation in relation to the late consequences of cancer treatment on a patient's potential for fatherhood after completion of treatment. 5
The opportunity for experiencing parenthood has significantly improved for the past 5 years with improvements and developments in fertility preservation techniques. In vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI) have afforded cancer patients and their partners the opportunity to experience parenthood. Currently, the most common and efficient options for male patients to preserve their sperm is through semen cryopreservation; unfortunately, <27% of males choose to undergo semen cryopreservation before their cancer treatment.14,15 Some males may be unable to produce a semen sample before starting treatment as a result of stress, severe illness, or sexual inexperience. However, there are also other methods used to extract sperm for cryopreservation through testicular sperm extraction (TESE) and electroejaculation. TESE involves the removal of a small section of tissue from the testis and extracting any viable sperm cells from the tissue that can be later used for IVF procedures, including ICSI. 16 Electroejaculation involves collection of semen by electrical stimulation where an electric probe or an electroejaculator is inserted into the rectum and positioned against the prostate. 17 Electroejaculation maybe a viable option for sperm retrieval from such males. 17
The objective of this study was to assess semen quality before cryopreservation before starting cancer treatment in male patients who attended a reproductive medical facility in India.
Methods and Materials
Subjects
This study was approved by the Gunasheela Hospital Ethics Committee-EA/OA/11/2020.
The research group retrospectively reviewed medical records of 461 male patients with cancers. Males who were eligible for participation in the study were between the ages of 15 and 40 years. We defined our reproductive population starting at puberty, which we defined as 15 years of age, and included males up until the age of 40 years. Furthermore, only patients belonging to this age group visited the clinic during the study period. These patients had been referred to a tertiary fertility centre for sperm banking between the years January 8, 2008 and October 30, 2020. Only those patients who had cryopreserved sperm before starting treatment were included in the study. We were only interested in exploring the following semen parameters, which included asthenozoospermia (reduction in sperm motility), oligozoospermia (low sperm concentration), oligoastheozoospermia (combination of low sperm concentration and low sperm motility), and azoospermia (absence of sperm in a semen sample).
A total of 486 males presented to the fertility clinic in India to cryopreserve semen before starting cancer therapy. After the initial round of counseling by fertility experts, 461 male patients diagnosed with cancer cryopreserved a total of 1152 vials before starting cancer therapy. At referral, 2.7% of the cancer patients did not opt for cryopreservation due to personal reasons unrelated to their medical condition and other 2.6% of males did not have their medical records, including their cancer diagnosis archived. These patients were subsequently excluded from this study.
Semen collection and assessment of semen quality
Patients were initially subjected to blood screening for human immunodeficiency viruses, hepatitis B surface antigen, hepatitis C, and Venereal Disease Research Laboratory infections before conducting semen analysis. Semen specimen was collected by masturbation after being recommended to maintain 2–3 days of abstinence. However, most patients sample were collected at time of consultation as they were under time constraints to begin their cancer treatment.
Semen quality analysis
Semen samples collected were preliminary analyzed for color and viscosity. The semen volume was measured using a 14 mL graduated tube. The pH of semen samples collected was determined using a pH indicator (Bromothymol Blue solution [pH: 6.0–7.6]; Qualigens/Nice). Sperm concentration was established manually using aMakler counting chamber (Sefi-Medical Instruments) under a phase contrast microscope (Olympus cx41), in the andrology unit. The formula used to determine sperm concentration is as follows: (Σ live sperm and dead sperm)/100 squares. One hundred squares are formed by 10 vertical and 10 horizontal rows. Samples were then accounted for sperm motility in the Makler counting chamber under a phase contrast microscope as well. Grading was based on percentage of progressive motility and nonprogressive motility of sperm. Their percent-values were established based on the number of live sperm × 100/total sperm for each grade. Normal forms (%) (morphology) of sperm were assessed using the strict Tygerberg criteria on the sperm morphology of head, neck, mid-piece, and tail. They were determined by placing the sample on prestained slides (CANmorph-Pre-stained Sperm Morphology Slides; Candore) and further visualized under a microscope.
Normal sperm freezing procedure
Glycerol cryoprotectant media (Quinn's Advantage Sperm Freezing Media; Origio) was added to the processed semen sample (wash method) in a 1:1 ratio with constant stirring. Semen samples with cryoprotectant were then transferred into cryogenic vials (Nunc cryovials, Thermo Fisher Scientific). All vials were labeled with names of male patients. Married patients had their partner's name also labeled. The vials also contained information on laboratory serial number, hospital infertility number, patient registration number, and date. Vials were precooled in a refrigerator for 60 minutes at +2°C to 8°C. After 60 minutes, vials were transferred to a freezer for 10 minutes at −20°C and further transferred to liquid nitrogen vapor for 10 minutes. The vials were later plunged using a cane and canister into liquid nitrogen and then stored in a cryostorage tank (Jumbo 12).
Statistical analysis
The data were retrieved by paperback medical records and entered into Microsoft Excel. Semen parameter were descriptively analyzed for mean, median, interquartile range, minimum, and maximum values. Data were analyzed using R software version 4.0.2. Median difference between three group was tested by Kruskal–Wallis Test. p < 0.05 was to be considered statically significant.
Results
Table 1 describes the number of patients in various cancer groups and their mean age. Cancer was categorized into three groups: (1) testicular cancer, (2) hematological cancer, and (3) other cancers. Overall, male patients who cryopreserved their semen before starting cancer treatment had a mean age of 27.93 years (standard deviation [SD]: 4.90 years). The number of patients with testicular cancer were reported to be the highest with 199 patients (43.2%) with a mean age of 25.8 years (SD: 4.90 years) followed by hematological cancer group (171 patients [37.1%] who presented with a notably younger mean age group of 25.6 years [SD: 6.07 years]. There were 91 patients [19.7%]) with other cancers who reported a mean age of 26 years (SD: 7.00). Males diagnosed with the hematological malignancies included Hodgkin lymphoma (n = 120, 26.0%), non-Hodgkin lymphoma (n = 20, 4.3%), lymphoma (n = 20, 4.3%), and leukemia (n = 11, 2.4%). Conversely, the other cancer group include neurological cancer (n = 19, 4.1%), head and neck cancer (n = 7, 1.5%), bone and soft tissue cancer (n = 30, 6.5%), penile cancer (n = 4, 0.9%), gastrointestinal cancer (n = 27, 5.9%), lung cancer (n = 1, 0.2%), and thyroid cancer (n = 3, 0.7%).
Various Cancer Types Associated with Number of Subjects Per Group
These numbers are in bold as they represent the three main cancer groups of interest for this study.
Table also shows the mean age of subjects in each group ± SD.
SD, standard deviation.
Semen parameters are highlighted in Figure 1. The median semen volume between all the cancer groups is 2 mL (IQR: 1.5–3.5 mL), with a mean sperm concentration of 53 × 106/mL (IQR: 17–75.2 × 106/mL) and a mean sperm progressive motility of 47% (IQR: 33%–47%). Males with testicular cancer had a median semen volume of 2.5 mL (IQR: 1.5–3.5 mL) (Fig. 1A), whereas to hematological cancer group had a median semen volume of 2 mL (IQR: 1.3–3 mL), and the other cancer group is shown to have median semen volume of 2.4 mL (IQR: 1.5–4). Semen volume was between the cancer groups were seen to be normal when compared with World Health Organization (WHO) criteria for semen volume (>1.5 mL). Figure 1B highlights that males with testicular cancer had a sperm concentration that was much lower compared with males diagnosed with malignancies from the other two groups (hematological and other cancers). Males with testicular cancer had median sperm concentration of 34 × 106/mL (IQR: 10.1–60 × 106/mL), whereas hematological cancer patients presented with median sperm concentration of 66 × 106/mL (IQR: 23–84.2 × 106/mL), and the other cancer group had median sperm concentration of 62 × 106/mL (IQR: 27–86.3 × 106/mL). However, when compared with WHO criteria for sperm concentration (>15 × 106/mL) it was determined that there were differences between cancer groups. Sperm concentration across all the groups were shown to be significant (p < 0.001).
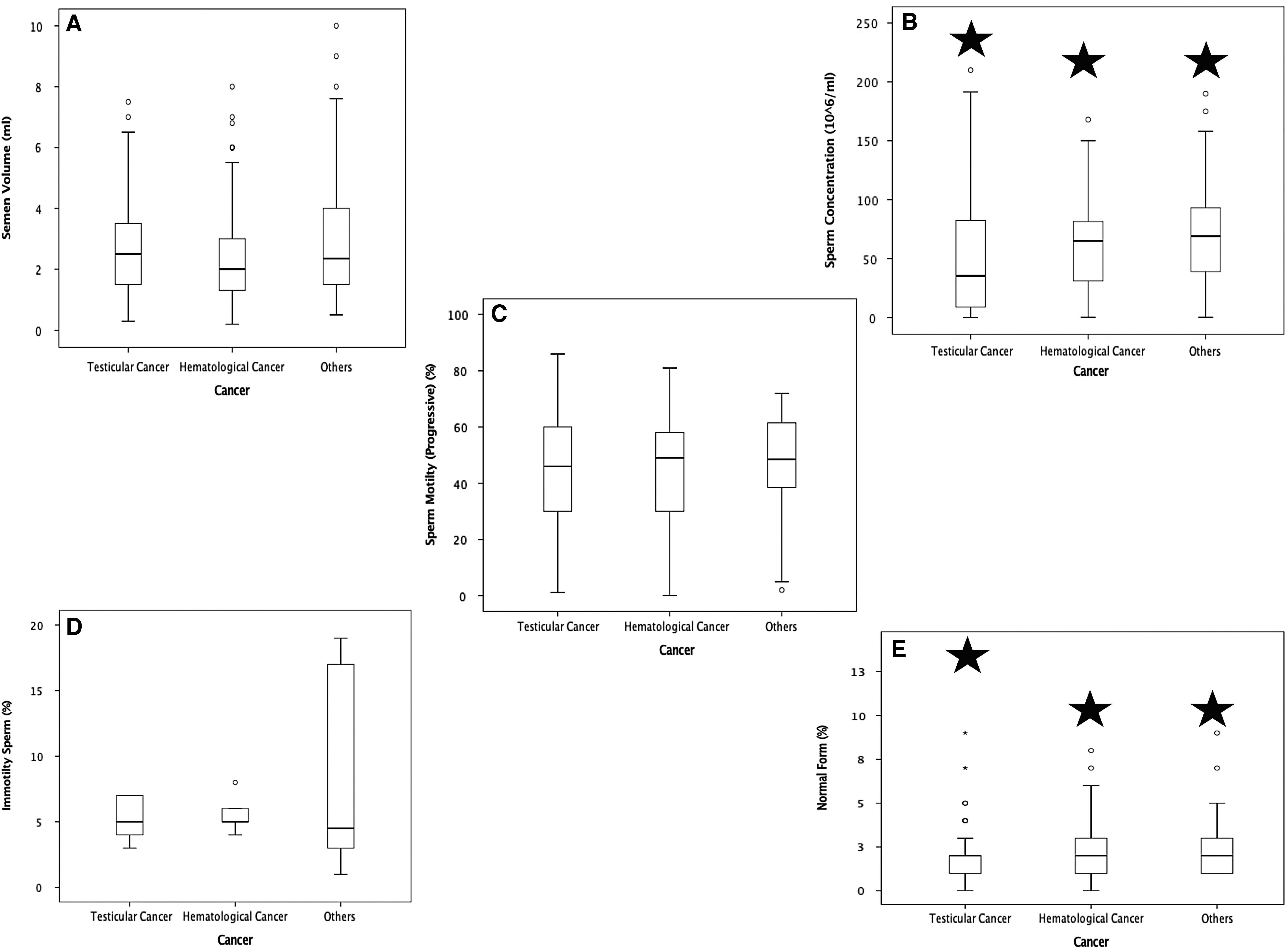
Boxplots representing semen parameter between cancer groups.
Figure 1C highlights the progressive sperm motility between the cancer groups. Patients with testicular cancer are shown to have a median progressive motility of 46% (IQR: 30%–61%). Hematological cancer patients are observed to have a median progressive motility of 49% (IQR: 30%–58%). Finally, patients diagnosed with all other cancers are seen to have median progressive motility of 48.5% (IQR: 37.8%–61.8%). It was also reported that progressive motility between cancer groups were normal in accordance to WHO criteria for progressive motility (32%). As detailed in Figure 1D, males diagnosed with hematological malignancy reported an increase in immotile sperm (median 6.1%) compared testicular cancer group (median of 5.1%) and hematological cancer (median of 4.9%). However, the other cancer group is shown to have an increased IQR (3.2%–18.2%) compared with the testicular cancer group (IQR 4.1%–7.2%) and hematological cancer group (IQR 4.9%–5.4%). None of the aforementioned semen parameters showed any statistical significance.
Figure 1E conveys that there is no difference in median normal forms (2%) between the cancer groups. However, the median was comparatively lower compared with the WHO criteria normal form of ≥4, which was statistically significant (p = 0.02)
Figure 2 describes the relationship between progressive motility (%) and sperm concentration (106/mL). In testicular cancer patients it is clear that they are more widely distributed. However, the majority of the patients in this group are seen to have poor sperm concentration and, therefore, poor progressive motility. The hematological cancer patients are seen to have better distribution with increased sperm concentration and motility. It is clear that the other cancer group is shown to have the best sperm concentration to motility relationship, in terms of increase in both the parameters.
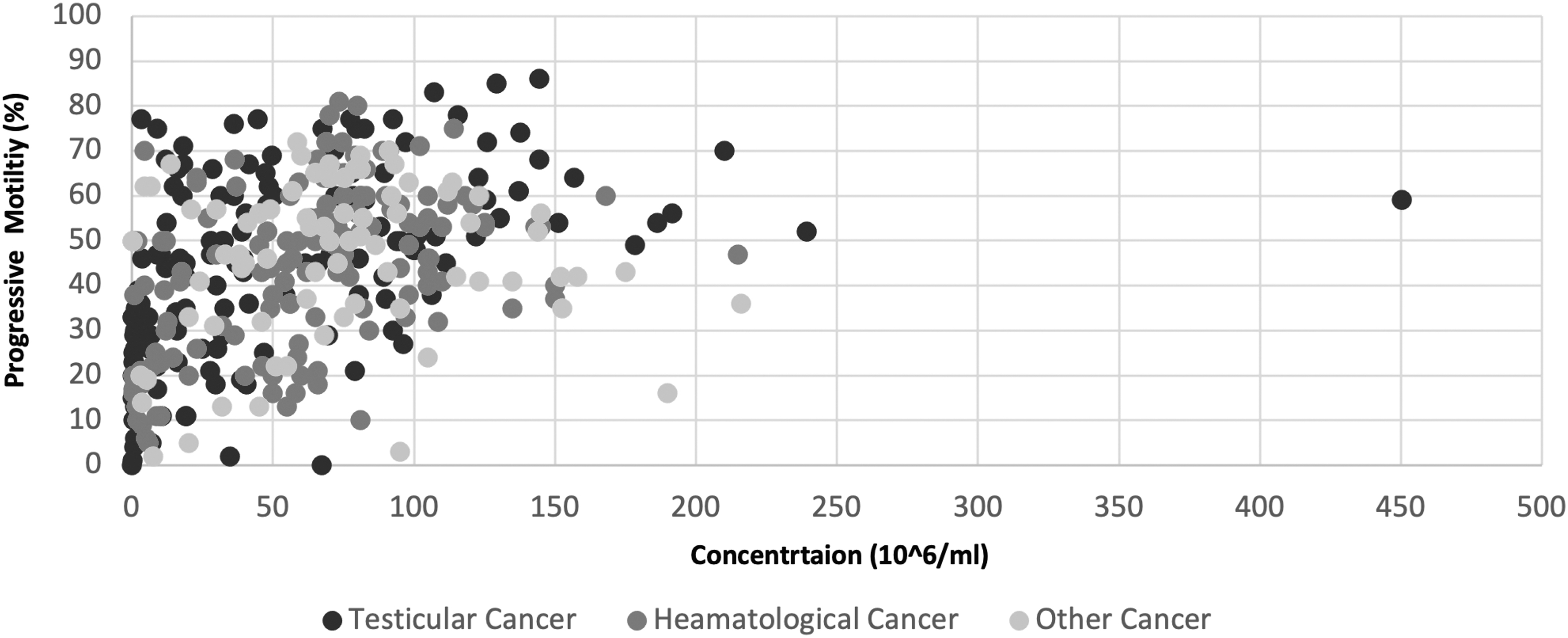
Correlation between progressive motility (%) and sperm concentration (106/mL) between cancer groups.
Table 2 shows different semen disorders in various cancer groups. Testicular cancer patients presented with higher frequencies of asthenozoospemia (4.8%) versus 3.3% in hematological cancer and 2.2% in other cancers, oligoastheozoospermia (5.4%) versus 5.4% in hematological cancer and 0.9% in other cancers, oligozoospermia (5.2%) versus 2.8% in hematological cancer and 1.1% in other cancers, and azoospermia (4.3%) versus 1.7% in hematological cancer and 0.4% in other cancers. Using WHO criteria (fifth edition 2010), 18 5.2% of males with testicular cancer presented with oligozoospermia compared with males diagnosed with hematological (2.8%) and other cancers (1.1%) (Table 2). Male patients with testicular cancer were more likely to be azoospermic at the time of cryopreserving their sperm compared with males diagnosed hematological cancers and other cancers.
Sperm Analysis Between Cancer Groups
These numbers are in bold as they represent the three main cancer groups of interest for this study.
Table also displays the total number patients (%) with sperm disorder between cancer groups and within cancer group. Normal concentration and normal sperm motility is also shown across the cancer types.
Discussion
This analysis represents a significant contribution in better understanding semen quality in males diagnosed with cancer in an Indian subpopulation. We report that males diagnosed with testicular cancer report a lower sperm concentration compared with males diagnosed with cancers from the other two groups (hematological and other cancers). These patients should be afforded the opportunity to discuss their fertility in relation to their diagnosis and treatment. Hence, a timely referral to a reproductive specialist should be prioritised for counseling regarding the potential late consequences in relation to cancer treatment on a patient's reproductive potential. 5
Several studies have reported an increase in fertility-related anxiety in cancer patients in the survivorship period if their reproductive potential has been negatively affected by their cancer treatment. 19 Current clinical guidelines5,20,21 recommend that male cancer patients be referred for oncofertility counseling and discussions regarding infertility as part of their comprehensive cancer management plan, including those men who may have already fathered children. 5
The literature reports that a diagnosis of cancer has adverse effects on semen quality. A study by Colpi et al. 22 reported outcomes for males in Italy who cryopreserved sperm before undergoing cancer treatment and showed that <40% with lymphoma, 37% with testicular cancer, and 37% with other tumors presented with normal semen parameters. Similarly, studies by Lass et al. also reported that 50% of men with cancer who cryopreserved semen before starting treatment had <10 million motile sperm per milliliter. 23 Hallak et al. indicated that patients with testicular cancer, presented with inferior semen parameters compared with controls.24,25
Conversely, Meseguer et al. reported on semen parameters of 184 Spanish males who cryopreserved semen before cancer therapy had reported no significant differences in total sperm concentration among these men with a prior cancer diagnosis.25,26 These results were also supported by Chung et al., van Casteren et al., and Žáková et al. who also convey no significant differences in motility between different cancers.8,25,27,28
This study shows poorer semen parameters in testicular cancer patients at the time of cryopreservation compared with the other cancer groups. Several studies have indicated that histological modifications such as dysgenesis syndrome (25.2%) as well as fibrosis of the seminiferous tubules (24%–60%), sertoli cells only (8%), and in situ carcinoma (5%–8%) are evident in the contralateral testis in patients.12,29 Impairment of spermatogenesis in cancer patients with testicular cancer at the time of sperm banking is multifactorial and may be related to (1) hormonal aberration (increased FSH, b-human chorionic gonadotrophin, a-fetoprotein, estradiol and Luteinizing Hormone (LH), and decreased inhibin B and testosterone); (2) a history of cryptorchidism, which seems to present more frequently in males with testicular cancer (Virtanen et al., 2007); and (3) general dysfunction due to cancer (increased catabolic rate and malnutrition).12,27,30
In this study, patients with hematological cancer had a mean sperm concentration of 66 × 106/mL, which was markedly higher compared with patients in the other cancer groups (testicular and other cancers). However, these findings are higher compared with those by Bizet et al. 31 who reported a sperm concentration of 15 × 106/mL. The literature reports that hyperthermia can contribute to alter semen parameters and contribute to impairment of spermatogenesis, due to the adverse effects of elevated scrotal temperature.31–33 Van der Kaaij et al. presented a correlation between decrease in semen parameters and B-symptoms associated with lymphoma (e.g., fever and night sweats). Hyperthermia may also affect the germinal epithelium and, cause disturbance to the hypothalamic–hypophyseal axis, which could negatively affect sperm production.31,34,35
This study shows poorer semen parameters in testicular cancer patients at the time of cryopreservation compared with the other cancer groups. Several studies have indicated that histological modifications such as dysgenesis syndrome (25.2%), fibrosis of the seminiferous tubules (24%–60%), sertoli cells only (8%), and in situ carcinoma (5%–8%) are evident in the contralateral testis in patients.12,29 Impairment of spermatogenesis in cancer patients with testicular cancer at the time of sperm banking is multifactorial and may be related to (1) hormonal aberration (increased FSH, b-human chorionic gonadotrophin, a-fetoprotein, estradiol, and LH, and decreased inhibin B and testosterone); (2) a previous medical history of cryptorchidism, which seems to present more frequently in males with testicular cancer (Virtanen et al., 2007); and (3) general dysfunction due to cancer (increased catabolic rate and malnutrition).12,27,30
Patients with hematological cancer had a mean sperm concentration of 66 × 106/mL, which was markedly higher compared with patients in the other cancer groups (testicular and other cancers). However, these findings are higher compared with those by Bizet et al. 31 who reported a sperm concentration of 15 × 106/mL. Hyperthermia in Hodgkin and non-Hodgkin disease has been reported to alter semen parameters and contribute to impairment of spermatogenesis, due to the adverse effects of elevated scrotal temperature.31–33 Ragni et al. showed azoospermia rates at the time of cryopreservation and before starting cancer treatment of 11.6% 36 ; we observe lower overall azoospermia rates of 5.2% across all cancer types.
Poor semen quality in cancer patients, before starting treatment, is multifactorial. Patients may have underlying conditions such as pre-existing defects in germ cells, local tumor effects, endocrine disturbances, autoimmune, and systemic effects.25,36
Limitations
The total sample size for this study was lower compared with other studies. 5 Furthermore, there were different sample sizes between each of the cancer groups, with an over-representation of patients diagnosed with testicular cancer. In addition, semen analysis, including sperm concentration and motility, was manually analyzed, which may potentially cause human error with greater accuracy generated with the use of a computer-assisted semen analysis (CASA) for increased accuracy. 37
We also did not have an age-matched control group (without a history of cancer) to compare semen parameters. However, despite some of the limitations associated with this study, we still report several interesting findings.
Conclusion
This study presents outcomes in support of international guidelines that recommend patients be referred for discussions around treatment-related fertility impairment before starting cancer treatment as well as psychosociological support in oncofertility. 5 This study also gives us an insight into how different types of cancers affect semen parameters in male patients among an Indian subpopulation. Further studies with larger sample size are recommended to show significance and to investigate semen parameters between cancer types in males of a reproductive age.
Data Availability Statement
All data pertaining to this study are contained and presented in this article.
Footnotes
Authors' Contributions
B.G, L.A, A.N., and D.G were responsible for the conception and design of this study. I.S.B was responsible for semen analysis and cryopreserving sperm. A.K., B.G., and L.A were responsible for the analysis of data. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.