
Abstract
Purpose:
The distress and unique needs of AYAs (adolescent/young adults) with an oncology diagnosis have been well explored and documented in the literature. However, effective means of reducing distress and meeting needs has been more elusive. This study explored the impact of a 6-week psychoeducational pilot group on AYA distress.
Methods:
Patient surveys and literature review were conducted to develop content for a 6-week psychoeducational group to reduce AYA distress through peer support and increased knowledge related to symptom management, physician communication, body image, family relationships, autonomy, sexuality, fertility, and coping skills. Distress was measured using the Hospital Anxiety and Depression Scale (HADS).
Results:
Twenty-one AYAs receiving oncology treatment enrolled in the group. Thirteen completed the program. Reasons for attrition included transportation, severity of symptoms, procedures, disinterest, and death. A correlated t-test demonstrated a significant decrease in HADS total score from pre- to post-test.
Conclusion:
This pilot study suggests that providing AYAs with information relative to their unique developmental needs and opportunities to process those needs in an environment of peers is challenging but can have benefit. nCT01817335
Introduction/Background
Adolescent and young adulthood is marked by a challenging period of emotional, social, and cognitive development as individuals attempt to navigate the multiple developmental demands associated with this crucial phase of life. 1 Although psycho-oncology literature in the area of the unique needs of adolescents and young adults (AYAs) diagnosed with cancer is becoming well established, research into the effectiveness of interventions is still developing. Since the discovery of less improvement in survival rates for AYAs relative to pediatric and adult populations, 2 attention has been drawn to the unmet needs of this group that impact both distress and treatment outcomes.
Research on the unmet needs of AYAs suggests several categories of need: information, counseling, practical service, social, and physical. The need for information is predominant and persistent. The need for information on medical care (treatment, possibility and signs of recurrence, long-term side effects, and possibility of new cancer developing), navigating the health system and fertility are seen across multiple studies.3–6
Counseling needs for AYAs range from the need for coping and normalization to mental health and drug and alcohol treatment.1,4,5,7,8 Zebrack et al. found that not having counseling needs meet was associated with more distress over time. 9 Reported practical service needs focused on maintaining school and work 8 as well as assistance with finances, transportation, children, insurance, and disability.10,11
Needs for social interactions were not always included in studies of AYA needs, but research utilizing interviews reported needs for peer interactions, peer support, camps, and retreats.7,8,12,13 Several studies reported a support group as a need.10,14 The need for peer interaction was reflected in studies that suggested a need for inpatient age appropriate care space and entertainment areas with internet access to connect with peers inside and outside the hospital.7–9 The final category of need, physical need, included symptom management, including pain management, rehabilitation, diet and nutrition, and activity or exercise.3,6,8–10
Although the needs of AYAs have been well explored, research on the effectiveness of interventions to meet the psychosocial needs of AYAs is yet immature. Walker et al. 15 identified 18 studies with varied interventions (individual therapy, group therapy, family intervention, educational interventions, skills-based interventions, and physical activity) and outcomes. These studies generally showed a positive effect for participants overall, but disappointing effects on distress, resilience, and quality of life. Thornton et al. 16 reviewed research on interventions and categorized them into the areas of creative expression, peer interactions, individual coaching, technology, promoting physical activity, and clinical interactions. Reciprocal support between peers can have positive effects on AYAs with cancer, including reduction of distress and anxiety,17,18 yet research on support groups or peers groups is minimal. Of the groups reported in research, few if any take on the breadth of information, counseling, practical service, social, and physical needs reported for AYAs across the literature.19–21
Although the needs of AYAs have been well documented, meeting the psychosocial and educational needs of this group remains a challenge. In addition, research has indicated that meeting the supportive and educational needs of AYAs can have an impact on distress and quality of life.3,9 This study sought to examine the feasibility of an educational peer interaction group for patients on or recently off treatment and explore the impact of the group on patient distress.
Methods
Procedure
IRB approval was sought and obtained to conduct this prospective study. All participants were consented, informed of the risks and possible benefits of participation, and provided with the opportunity to ask questions or withdraw at any time.
Information from a review of the literature and a needs-assessment conducted at City of Hope was used to develop the psychoeducational program.1,5,13 A multidisciplinary team of supportive care providers (clinical social work, psychology, child life, and patient education) reviewed the available literature as well as information gathered from the needs assessment and identified the following areas of need: symptom management, coping skills, self-image, relationships, fertility, and communication with the medical team. A 6-week educational and peer support program was developed to address the defined areas of need. Information on the session topics and objectives are presented in Table 1. The group was facilitated by two team members (social work and child life) in the treatment hospital. Sessions included a presentation by a subject matter expert on each topic for 45 minutes followed by 45–60 minutes of facilitated peer discussion and support. Each attendee was entered into a raffle weekly and had the opportunity to win a gift card for attendance. The 6-week program was conducted four times to gather the number of evaluable subjects needed for the pilot study.
Session Topics and Objectives
Subjects were recruited for the study through fliers, electronic media internal to the hospital, and referrals from medical or supportive care providers. Subjects aged 18–39 years, in treatment for a cancer diagnosis, without significant psychiatric or developmental issues, and English speaking were invited to participate in the study.
Measures
The Hospital Anxiety and Depression Scale (HADS) is a measure of anxiety, depression, and overall distress for hospital populations. 22 The overall distress score is determined by adding the anxiety and depression subscores. The HADS was chosen to measure distress due to its ease of use, short time of completion, helpfulness in determining clinical distress, and prior use in the oncology population. 23 The tool was administered at the time of consent, during the sixth and final session, and 6 weeks after the final session. The HADS overall distress score was used for analyses.
Attendance was collected and reasons for nonattendance of group members documented to track attrition. A subject satisfaction survey was administered after each education session and at the end of the program.
Data analysis
Descriptive statistics were used to characterize the patient sample and reasons for attrition from the group. Independent t-tests were run to explore changes in participant HADS scores before and after participation in the group. Analyses were planned between HADS scores at time of consent (pre-test), at the final session (post-test), and at the 6-week follow-up. Owing to attrition, many subjects had missing HADS scores for the post-test or the follow-up data collection points. HADS scores from the post-test and follow-up tests were combined to provide sufficient data for analysis. In the four cases in which the participant provided both post-test and follow-up data, the score closest to the pre-score was used. Subjects with pre- but neither post- nor follow-up HADS scores were excluded from pre- to post-analyses.
Results
Sample demographic characteristics
Twenty-one AYAs receiving oncology treatment enrolled in the program, completed preprogram questionnaires, and attended at least one session. The average age of the participants enrolled was 22.62 years (range = 18–29). Participants identified as female in 52.4% of the cases. More than half identified as Hispanic (52%), 29% as white non-Hispanic, 9% as Asian, and 9% as other ethnicity. Sixty-two percent of the participants carried a diagnosis of leukemia or lymphoma, 24% solid tumor, and 14% other diagnoses.
Attrition
Of the 21 participants enrolled, 13 completed the program. Reasons for attrition included challenges with transportation (for outpatients), a medical procedure scheduled during the same time, side effects of treatment preventing attendance, isolation precautions, death, and disinterest. Unfortunately, the relative quantity of each reason for attrition was not measured. Five of the 21 participants attended just 1 session and only 1 participant attended all 6 sessions. The distribution of attendance is shown in Figure 1.
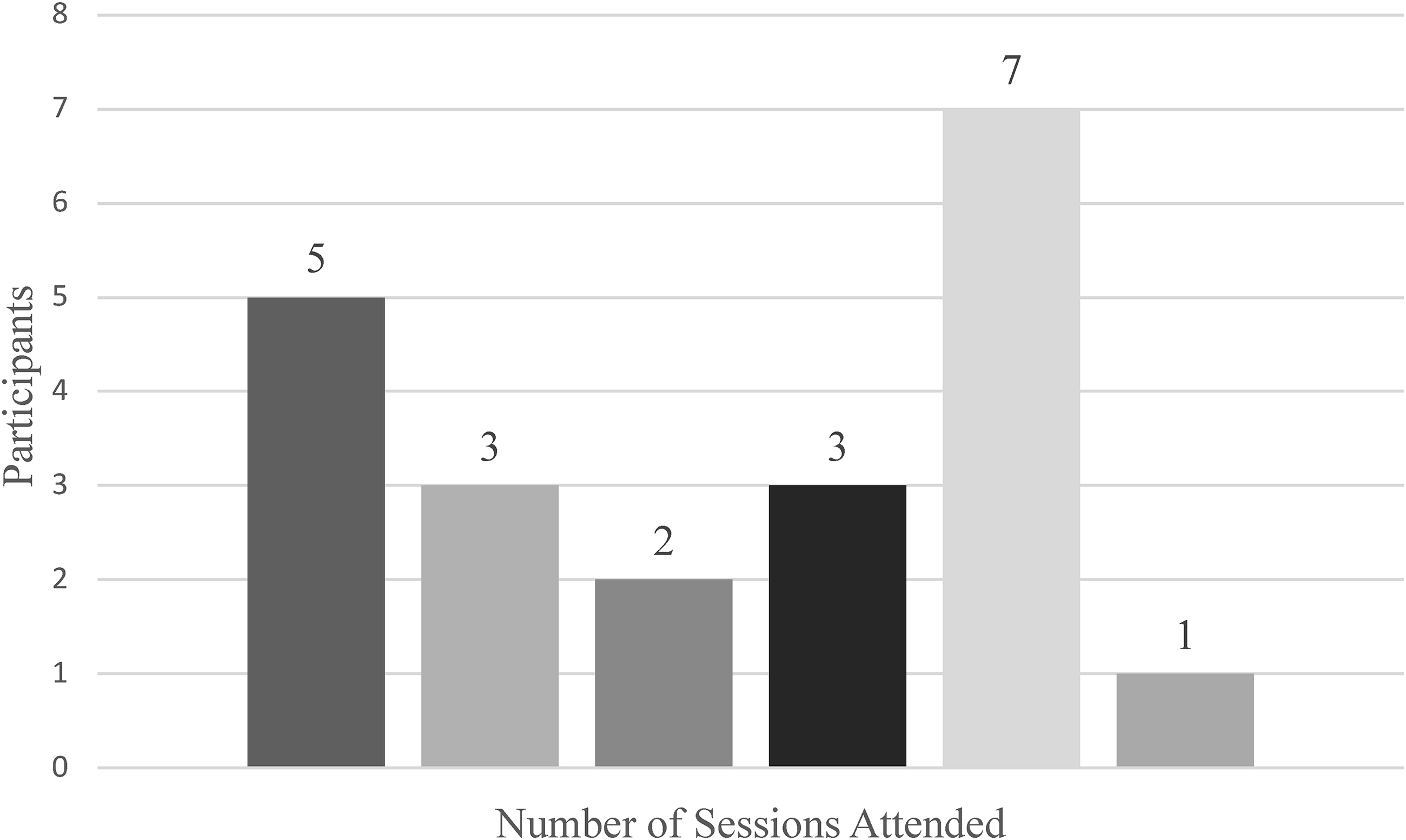
Number of sessions attended by participants.
Impact on distress
The mean HADS scores before the program was 13.83 (n = 21, range = 0–28), which is lower than cutoff of 16 for an indication of distress recommended by Singer et al. 23 Examination of individual distress scores revealed that 41% scored higher than the recommended cutoff for distress. The mean preintervention HADS score for participants who completed the program (completed pre- and post- or follow-up measures and attended greater than half the sessions) was 14.38 (n = 13, range = 0–26), which is higher than the mean of the total enrolled but still below the recommended cutoff for distress. Clinical distress was indicated in 33% of pretest HADS scores for the 13 who completed the program.
A correlated t-test of the significance of change in HADS scores from pre- to post-intervention was performed. Results demonstrated a significant decline in HADS distress scores from pre- to post-test for those who attended the group. These results are shown in Figure 2 [F(1,12) = 9.39, p = 0.01]. The relationship between group attendance and decline in distress scores were examined. An F test of correlation demonstrated that the correlation between the number of groups attended and change in HADS score was very low (r = 0.20) and not significant [F(1,10) = 0.40, p = 0.54]. Similarly, a correlated t-test of the changes in distress for those who attended four or more groups versus those attended three or less groups found no significant difference [F(1,11) = 0.29, p = 0.7].

Change in HADS scores. HADS, Hospital Anxiety and Depression Scale.
Discussion
The goal of this study was to explore the feasibility of a psychoeducational peer interaction group on young adult patient distress. Results demonstrated that although it was quite easy to enroll patients in the group, attrition was higher than desired. Reasons for attrition included medical procedure scheduled during the same time, side effects of treatment preventing attendance, isolation precautions, transportation, death, and disinterest. This research was conducted in the era before Covid-19 and the acceleration of efforts and removal of barriers to providing such services online. Future research utilizing electronic means of participants joining the group is of interest and might reduce barriers to attendance observed in this group, including transportation and isolation precautions.
Although adolescents and young adults are not always keen to engage in a support group,11,21 peer interventions have been shown to have potential effectiveness for reduction of anxiety and overall distress. 17 Informal peer activities and adventures can be quite successful in fostering peer bonding and promoting effective coping skills.24,25 However, they are not always feasible for patients on treatment or for care providers to offer and do not meet the information needs of patients during treatment. Although research into group interventions with AYAs is sparse, several recent articles have explored utilizing a cognitive-behavioral therapy model and found perceptions of acceptability and efficacy among participants.26,27 This research suggests the possibility that an educational peer group might also be an avenue to address AYA psychosocial needs.
Although the primary goal was to explore the feasibility of a psychoeducational peer interaction group, we were also interested in exploring the distress of young adults on or recently off treatment and examine trends in distress while attending the group. Although distress scores of participants declined with attendance in the group, it does not appear that the decline is related to the number of groups attended. Because this was not a randomized control study, we cannot attribute declines in distress scores to participation in the group. Further opportunities for research include increasing the power of the analyses by enrolling more subjects, comparing participation in the group with a randomized control option, and reducing barriers to participation through electronic attendance options.
Young adults are in a developmental phase of life in which socialization with peers is of premier importance. Often, a diagnosis of cancer and need for treatment interferes with reaching social, educational, and occupational milestones, and results in feelings of isolation and being left behind. 20 Continued attempts to address the distress and needs of young adults are necessary and should make use of advances in electronic means and telehealth to connect patients with peers that share their experience and concerns.
Footnotes
Acknowledgments
We thank the Department of Supportive Care Medicine and the Department of Pediatrics for support of this clinical effort and research.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by grants from the Held Foundation next Gen Board and the Simon Strauss Foundation.