
Abstract
Purpose:
The purpose of the study was to create in Italian a transition protocol survey to monitor the readiness of childhood, adolescent, and young adult (CAYA) cancer survivors who are undergoing transition from pediatric to adult health care. A protocol could support clinical practice through the proposal of individualized transition care pathways for CAYA survivors and inform future scientific studies that focus on barriers to successful transition.
Methods:
Three international questionnaires that investigate the biopsychosocial issues and needs of survivors were subjected to the Forward and Backward Translation process. Following this, CAYA survivors were recruited from September 2019 to August 2020 in the pediatric oncology centers of the Interregional Pediatric Oncology Network of Piedmont and the Aosta in Italy to participate in cognitive interviews as part of the validation and cultural adaptation process of the questionnaires, which will form the transition protocol survey.
Results:
Revisions and cognitive interviews with 40 CAYA survivors identified any inadequate expressions and resolved any concepts of misunderstanding or cultural unsuitability for the Italian translation. Overall, they found the scales to be easily understandable, and an Italian version of the scales was produced to create the final transition protocol survey.
Conclusion:
The transition protocol survey might be used as a valid tool to highlight critical issues to support sustainable transition processes between Italian oncology centers. The protocol can be implemented into clinical practice thus offering CAYA the possibility of resolving some needs, receiving personalized support, and surveillance before the transition.
Introduction
The number of childhood, adolescent, and young adult (CAYA) cancer survivors has increased in recent years in the most economically developed countries. In Europe approximately 80%–84% of cancer patients now reach 5-year survival, and around 70% will survive 10 years following end of treatment.1,2 To date in Italy there are more than 44,000 Italians who, thanks to ever improved diagnosis and treatment protocols and personalized follow-up protocols, are living many years after a cancer diagnosis in young adult age and for this reason are defined as long-term cancer survivors.3,4
CAYA survivors have been at the center of new research in the literature that, over the years, has aimed to highlight not only possible sequelae of the disease on a physical level but also on a psychosocial level.4,5
For these reasons, the most important research has been carried out in the biopsychosocial field with the aim of deepening youth's global survivorship conditions by considering the mutual interactions of sequela and the impact on quality of life (QOL). 6 Following this perspective, clinicians are then facilitated to propose targeted care for survivors that takes into account all of the QOL dimensions investigated. 7
The most frequent of long-term medical complications among survivors is cardiovascular diseases, endocrinopathies, and risk of secondary neoplasm. Although most survivors seem to have good psychosocial functioning, recent studies show a high prevalence of late effects that include psychological sequelae such as mental health (e.g., symptoms of anxiety and depression, post-traumatic stress disorder, and somatization), cognitive difficulties, body image discomfort, and psychosocial concerns such as educational achievements, employment status, social relationships, and lifestyle with these being particularly prevalent among the adolescent and young adult (AYA) population.8–10
It is well known that AYA cancer survivors experience many unique challenges and QOL effects compared to those observed in younger children or older adults. 11 The particular QOL problems during AYA survival are to be considered especially in that period when the patient transfers from the reference pediatric center to the adult center: a very delicate moment during which a range of potential barriers could jeopardize the survivor's adherence to follow-up. During this transition phase, care shifts from family-centered pediatrics to independent patient-centered health care, 12 where long-term follow-up surveillance is tailored to the individual necessities and medical history of each survivor.
The factors that facilitate this transition process are: the survivor's capacity for self-management, psychological and emotional balance, the achievement of good channels of communication with and trust in new health care professionals, and the provision of adequate medical information.13–15
Nevertheless, many survivors face barriers to their transition out of pediatric care with the main ones having cognitive dysfunctions, a strong attachment to previous health care providers, stress related to the condition of long-term survival, and having difficulties in achieving self-autonomy and autonomy from the family.
Cognitive difficulty and dependency on pediatrician were the most commonly reported barriers to transition among survivors and they seem linked with each other: cognitive difficulty hindered the development of self-management skills (e.g., remembering/retelling their medical history), which could lead to overdependence on past health care providers.
Regarding family and autonomy, studies in the literature highlight that families and providers continue to have an important role in supporting survivors especially in transition logistics and medical decision-making, which can unwittingly weaken the incentive for autonomy in survivors. 16
Furthermore, CAYA survivors may experience distress as they regain independence and return to normalcy and as a consequence of the fear of neoplasm recurrence and the impact of late effects (e.g., infertility). 13
It is also known that survivors often lack knowledge about their tumor, their treatment, and their risk of late effects and can be consumed by worries about those effects, all factors that may impede their successful transition into adult care. The literature emphasizes that the goals of “best practice” in the transition phase are to provide survivors with versatile and developmentally appropriate constant education regarding their cancer, potential late effects, and required surveillance and intervention strategies.15,17,18
For these reasons, a clinical screening of CAYA survivors' status can support both clinicians and survivors in the transition process 19 by overcoming several of these barriers to transition. 20
The primary goal was to create an Italian transition protocol survey that investigates the unique biopsychosocial issues experienced by CAYA survivors that are, for this report, individuals who were diagnosed with cancer before the age of 18, during the transition process, which takes place only after the survivor has reached the age of majority and at least 5 years have passed after the treatment completion.
First of all, to gain the primary goal, a literature search was performed to find validated patient reported outcome (PRO) measures tailored to the biopsychosocial issues involved in the transition process of CAYA survivors. As described above, the literature21–23 and clinical experience itself suggest that the most commonly implicated biopsychosocial issues in survivors' transition are: the distress left by the cancer experience in the different spheres of life (e.g., physical, social, sexual), the ability of survivors to take care of their own health (self-management skills), and survivor expectations at the moment of transition (concerning doctors, appointments etc.). After a careful search three transition tools were identified as the most scientifically sound measures of these issues: Cancer Distress Scale (CDS-AYA), 24 TRANSITION-Q, 25 and Childhood Cancer Survivor (CCS) Expectation Scale, 26 which have all been validated by a group of Canadian researchers. So, as a secondary goal, an Italian translation of these three international questionnaires was performed: linguistic validation is the process used to ensure that the PRO concepts were equivalent and easily understood by people from countries not involved in their development. The translation was performed in accordance with the translation guidelines of the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) and the World Health Organization (WHO)27,28 who provided guidelines for good practice in translation, linguistic validation, and cultural adaptation processes.
The validation of the Italian questionnaires will allow us to create a transition protocol survey to take into many and different aspects involved in the youth's survival and to intervene, if necessary, in filling some survivors' needs before the transition.
Materials and Methods
We obtained permission to translate the CDS-AYA, the TRANSITION-Q, and the CCS Expectation Scale from the developers. The administration of the three scales was approved by the Ethics Committee of the Regina Margherita Children's Hospital, in Italy. The approval number for observational studies (No. 125016).
The CDS-AYA scale 24 consists of 48 items divided in 5 subscales, which investigates the stress the tumor has caused to the patient's life from a biopsychosocial perspective. The following areas are investigated: Impact of Cancer (12 items), Physical (12 items), Emotional (11 items), Cognitive (8 items), and Worry (5 items). Each item comprises four response options (None = 1 to Severe = 4).
TRANSITION-Q 25 includes 14 items, and it investigates the self-management skills that CAYA possesses to better manage own cancer follow-up care pathways. The content of the scale was designed to include a range of skills from those that young adolescents should be able to perform (e.g., answer a doctor's or nurse's questions) to those that may require instruction or training (e.g., book a clinical appointment).
Each item includes three response options (Never = 1 to Always = 3). This scale can be used to help clinicians evaluate the survivor's readiness for transition.
The CCS Expectation Scale 26 verifies the expectations that CAYA survivors have toward the moment of transition from the pediatric hospital to adult center: it includes 12 items with 4 response options (Strongly agree = 1 to Strongly disagree = 4).
The translation process is described in Figure 1. The Forward and Backward Translation methodology was used for the translation procedure.27,28 First, the scales were translated into Italian and then back-translated into English to verify for item consistency and adaptability.

Steps of Italian translation. Steps of translation of CDS-AYA, TRANSITION Q, and EXPECTATIONS SCALE from English to Italian. CDS-AYA scale, Cancer Distress Scale.
The following steps were taken:
The initial forward translation from the original English into Italian was performed independently by two professional translators who have a detailed knowledge of the issues surrounding QOL for cancer survivors. These professionals are Italian native speakers with a proven knowledge of English and familiarity with this culture. The two translators provided two forward translations (Forward Translation 1 and Forward Translation 2). The two versions were then to be merged in the next step. The participants in the reconciliation procedure reviewed the two forward translations. Two forward translators and 1 clinician dedicated to survivors from the oncology research group with a good knowledge both of English and of the target language discussed and held a reconciliation meeting to address any divergences and to produce a single harmonized version of the instrument. An independent professional translator produced a Backward translation of the harmonized version. The translator's mother tongue was English and was fluent in Italian. The result of the backward translation process is a back-translated version of the Reconciled Forward Translation. We reviewed the Forward and Backward Translation to provide a Final Forward Translation. At this phase II experts of the panel with good knowledge of both English and Italian participated alongside one member of the forward translator group. The back-translated version of the three scales was compared item-by-item with the original one. Any discrepancies were noted and discussed with the scale developers, and any items with different meanings were retranslated. This process continued until a satisfactory result was achieved, leading to a Final Forward Translation. The translation had to be simple, clear, and concise, without conceptual discrepancies between the English Original and the Final Forward Translation. International Harmonization serves to assure and, if necessary, generate interconceptual equivalence. The feedback received was used to revise the scales, leading to consensus on an Italian Finalization version that was made ready for pretesting. The Pretest was expected to show whether all the items were comprehensible and acceptable. To determine the quality of the translation and to obtain feedback on the scales and their content, we performed cognitive interviews with a sample of 40 CAYA survivors in transition from the Pediatric Oncology Division of Regina Margherita Children's Hospital to the Transition Unit for Childhood Cancer Survivors, Città della Salute e della Scienza Hospital in Turin, Italy (Table 1). The eligibility criteria for this study were: cancer diagnosis at age <18 years; age at the time of the study >18 < 30 years; and off therapy >5 years. Patients with cognitive impairment or conditions otherwise hampering the participation to the study were excluded. Interview papers were conducted by a researcher on the occasion of the last visits made to the pediatric hospital with survivor without caregiver. Questions that were difficult to understand were explored and then asked to the survivors if the items were relevant to them or not and if any questions should be added. The survivor was asked to explain what each question meant to them in their own words. Meanwhile, the research assistants recorded any questions or problems the parents had and shared these findings with the research panel to aid the revision process. We asked them to highlight problems with the instructions, response options, and items and to suggest potential alternative wording. Their feedback was used to make some adjustments to the translation, and items that were difficult to understand in the Italian language were highlighted, leading to a final Italian version of the three scales. In the final step, we proceeded with International Harmonization to ensure the comparability between the translated questionnaire versions. We discussed all the questions raised to others concerning conceptual and cultural aspects of the item translations. The Final Questionnaire version was generated as a result of the process of International Harmonization.
Demographics and Clinical Characteristics of Participants
Results
The translation process led to an Italian version of the three scales that was linguistically validated and conceptually equivalent to the original English version. The changes made throughout the translation process on items of the scale can be found in Table 2.
Validation Process of Scales
CDS-AYA, Cancer Distress Scales-Adolescent and Young Adults.
In the first step we did not find any discrepancies between the two independent forward translations. For the CDS-AYA (Table 2), the only discrepancy that emerged was concerned with the use of the term “cancer” or “tumor.” By mutual agreement it was preferred to use “tumor.” Regarding observation and cultural issues surrounding the translation we highlighted a few considerations: we chose not to use the term “death” and “fertility” because we think these are too emotionally impacting for CAYA survivors in Italian oncology centers, which were replaced by “possibility of having children in the future” and “possibility of not being able to overcome the disease,” respectively. For TRANSITION-Q (Table 2) we used “medical” instead of “doctor” to highlight the role of all the health care professionals involved. In the CCS Expectation (Table 2) we did not find any divergences. Therefore, following discussion and revision, the two translators reached consensus on the first version in the Italian language (second step).
In the following steps (from the third to the fifth), the comparison of the back translation identified different items or instructions where the meaning differed, requiring a retranslation of those items and a subsequent review by the developers.
For example, in the CDS-AYA the original item “Impact of cancer on the pressure I feel to live a ‘meaningful’ life?” was initially back translated as “Impact of the tumor on the pressure that I feel to give my life meaning?” which was judged better as “Impact of cancer on the pressure I feel to live a ‘meaningful’ life?.” Another example was “Trouble putting my thoughts into words?” which initially we translated as “Difficulty turning my feelings into words?” but “feeling” and “thoughts” do not have the same meaning, so we translated it as “Trouble putting my thoughts into words?.”
Initially in TRANSITION-Q we translated the original item “I travel on my own to a doctor's appointment” with “I am able to get to my doctor's appointments by myself” but there was a wording discrepancy in the meaning so we retranslated it to “I travel on my own to a doctor's appointment.”
In CCS Expectation, for example, the original item “I expect the doctor will become like a friend” was translated as “I expect the doctor becomes almost a friend,” but following discrepancies we retranslated it and we found reconciliation with “I expect the doctor will become like a friend.”
The interactive process of comparing the Italian and English versions in an ongoing discussion with the developers helped to find consistent conceptual solutions. The panel of experts helped to identify and resolve unsatisfactory expressions and concepts in the back translation.
Specifically, 70 items or instructions were needed to be changed (50 on CDS-AYA Scales, 11 on CCS Expectation Scales, and 9 on TRANSITION-Q Scales). For example, in the original version of CDS-AYA the instructions for patients were “In the PAST WEEK, how much DISTRESS have you experienced as a result of the following.” We preferred to use “LAST WEEK” and “STRESS,” so we changed it to “In the last week how much stress have you felt thinking about.” In the follow phase (sixth step), we proceeded with Cognitive Interviews with a sample of 40 survivors which represented the sample of survivors who pass through the adult center every year.
We did not find particular difficulties in the administration. We changed 10 items (4 on CDS-AYA Scales, 3 on Expectation Scales, and 3 on TRANSITION-Q Scales).
For example, in the CDS-AYA Scale the item “Impact of the tumor on the pressure that I feel to give my life meaning?,” the patients highlighted that in the Italian language it is difficult to understand and too direct. This was similarly felt in the item “Impact of the tumor on my ability to participate fully in daily life?.”
In TRANSITION-Q the item “I look for an answer when I have a question about my health” and “I ask the doctor or nurse questions” are too general for the patients who asked more information about what kind of questions the answer referred to. In CCS Expectation the patients underlined difficulties for “I expect to go willingly to the follow-up appointments for my illness,” because they found it hard to imagine going with pleasure, so they suggested changing it to “I expect to be well received by the doctor.” For item “I expect the doctor becomes like a friend,” patients underlined that “friend” is culturally inappropriate and it is probably better asking “have a good relationship with the doctor.” Furthermore, in item “I expect the doctor to spend lots of time with me,” patients underlined that it is probably better to ask “I expect the doctor to dedicate the amount of time that I need.”
In the last phase, these changes were discussed followed by reconciliations and harmonization that led to the Italian version. Overall, the patients found the scales to be easily understandable.
The final proofreading stage led to minor change in grammar, resulting in a linguistically validated and equivalent Italian version of the three original Scales.
Discussion
CAYA survivors' transition from pediatric to adult centers is a critical phase that must be carefully organized and personalized to the needs of each survivor, which are identified using transition tools. 29
Researchers in Canada have developed and psychometrically evaluated three scales that cover constructs through which you can evaluate each survivor's readiness for transition. These constructs identify CAYA distress in relation to their past cancer diagnosis, which is examined through a biopsychosocial framework (e.g., physical, cognitive, sexual) since the cancer experience could lead to problems in numerous life spheres of youth development. 30 A further construct concerns the ability of survivors to take care of their own health. A cancer diagnosis that occurred during childhood may make it more difficult to develop such self-management skills since, as can be seen from clinical practice. In fact, patients have become accustomed to relying more on their parents given their cancer diagnosis at a young age. Therefore it is important that during the transition phase the ability of survivors to take care of their own health be examined and, if necessary, supported. In addition, it is also fundamental that clinicians know the expectations that CAYA survivors have concerning their transition from pediatric center to adult center for a successful transition to take place. For this reason, 3 scales were chosen to be translated into Italian (CDS-AYA, TRANSITION-Q, CCS Expectations). These scales have already shown themselves to be adapted in other CAYA survivor populations both from a clinically meaningful (content covering AYA transition constructs) and scientifically sound (valid, reliable, and responsive to change) perspective. An Italian version of the three scales was achieved. The scales will constitute the transition protocol survey that will be applied within the transition process in Italian oncology centers.
The transition process, explained in Figure 2, aims to purpose a successful transition that takes care of the needs of survivors in a biopsychosocial perspective.
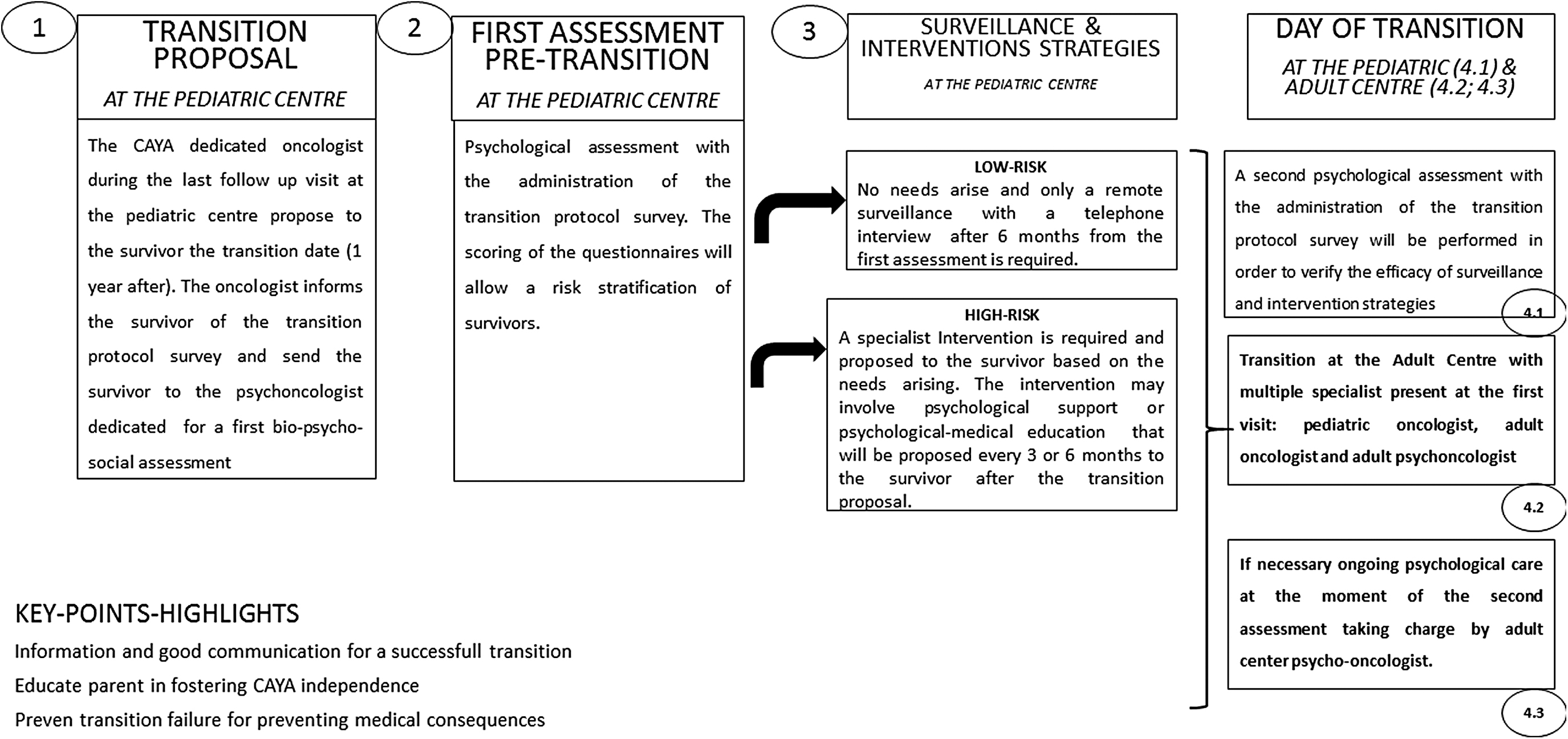
Model of CAYA survivors transition protocol survey. Transition: Promoting individualized transition adapted to the needs of each CAYA survivors. CAYA, childhood, adolescent, and young adult.
The model foresees that about a year before the oncologist of the pediatric center proposes the date of the transition to the adult center (phase I), the oncologist sends the patient to the psycho-oncologist for biopsychosocial assessment (phase II). During this first meeting, the transition protocol survey is administered. The obtained scores will allow to stratify the risk of survivors (phase III): low risk and high risk. For the first one, the assessment did not show significant needs, so the psycho-oncologist purposed a remote surveillance with a telephone interview after 6 months. For the second one, high-risk patients, a specialist intervention is required and proposed to the survivor based on the needs arising. The intervention may involve psychological support or psychological-medical education that will be proposed every 3 or 6 months to the survivor after the transition proposal. On the day of transition for each survivor a second psychological assessment is administered to verify the efficacy of surveillance and intervention strategies (4.1). Patients pass through the Adult Center for a first visit (4.2) and if necessary ongoing psychological care taken charge by adult center psycho-oncologist (4.3). The protocol is already in place in some Italian centers, and the efficiency data are being collected.
This is a protocol that creates a communication channel between the pediatric center and the follow-up center and that allows the center to act in a preventive manner by promoting the well-being of patients from a biopsychosocial and QOL perspective. It will also be important to measure the effectiveness of the protocol by evaluating the satisfaction and the QOL of survivors after about 6 months from their follow-up care transfer in adult health care system.
Nevertheless, we acknowledge that our study has some limitations. Our sample was recruited from the Centers of pediatric oncology of the North-West of Italy. Therefore, the inclusion of more centers might have increased the heterogeneity of the sample. However, the objective of our study was to search in the literature for the scales that best represent the constructs involved in the transition process with the aim of translating them and creating a protocol for CAYA cancer survivors in Italy. The translated scales are scales developed to examine the major constructs involved in the transition process that have already been validated in other countries and that are therefore potentially generalizable to other populations.
Our future objective will be to share this protocol with other oncology centers in Italy and to integrate it into transition practices, which to date in many European centers provides for the delivery of the Survivorship Passport (SurPass), an electronic document which summarizes the clinical history of the childhood or adolescent cancer survivor. The protocol and the SurPass will be able to contribute together at empowering the survivor to be conscious and responsible for their own well-being and at preventing adverse events whenever possible.
Footnotes
Acknowledgments
The authors are grateful to Unione Genitori Italiani (UGI), ADISCO Sezione Piemonte for the ongoing support to clinical and research activities and to all volunteers. The authors are also grateful to Elena Tsangaris, Department of Pediatrics, McMaster University, Hamilton, Canada, and Trisia Breitkopf and Anne Klassen, McMaster University, Hamilton, Ontario, Canada for permission to use and translate the instrument.
Author Disclosure Statement
All authors have nothing to declare.
Funding Information
No funding was received for this article.