
Abstract
Background:
Computer-based cognitive rehabilitation programs may help adolescent and young adult (AYA) patients with cancer-related cognitive impairment. This pilot study investigated the feasibility of cognitive rehabilitation as a preventive intervention for AYA patients receiving chemotherapy. Explorative objectives included the correlation of cognitive performance with serum brain-derived neurotrophic factor (BDNF).
Methods:
This pilot prospective study included English-speaking patients 12–25 years of age with a fist diagnosis of cancer requiring chemotherapy. Participants enrolled in the intervention arm participated in a computer-based neurocognitive training program for 20–30 minutes daily for 16 weeks. Outcome measures, including engagement with and completion of computerized neurocognitive testing and serum BDNF levels, were obtained within the first month following diagnosis, ∼16 and 24 weeks from enrollment.
Results:
Fourteen of 18 eligible patients provided consent, with 7 patients assigned to each the intervention arm and nonintervention arm. Seventy-one percent of the patients in the intervention arm completed at least 80% of the required activities. Compared to baseline, patients in the nonintervention arm demonstrated higher prevalence of impairment in four of the six cognitive domains (processing speed, visual attention, attention/working memory, and executive function) at the end of the study period. There was a nonstatistically significant reduction of serum BDNF levels over time, which was observed in both intervention and nonintervention arms.
Conclusion:
This pilot study provides some evidence that it is feasible for AYAs with new cancer diagnoses to receive standardized cognitive rehabilitation. Patients receiving cognitive activities experienced less impairment in numerous cognitive domains.
Introduction
In the United States, ∼90,000 adolescent and young adult (AYA) individuals between the ages of 15 and 39 years are diagnosed with cancer each year.1,2 Five-year survival now approaches 85% in this population, resulting in a steady growth of AYA cancer survivors (AYACS). 2 Among AYA cancer patients, cancer-related cognitive impairment (CRCI) was previously self-reported at least once within 12 months after cancer diagnosis.3,4 This may result in problems with memory, task efficiency, and organization. 5 CRCI can lead to decreased quality of life (QOL), difficulty with job attainment, and poor psychosocial outcomes in survivors.6,7 Many survivors report forgetfulness and trouble with attention in school or work.8,9 The multifactorial effects of cancer and chemotherapy on cognition also include acute and sustained insult to neuronal structures essential for learning and memory.10,11 Dewar and colleagues, utilizing a large database from the National Health interview Survey between 2010 and 2018, found higher rates of psychological distress and cognitive dysfunction among AYACS diagnosed after the age of 10. 12 Despite growing awareness of these unique needs in AYACS, there is paucity in the literature addressing neuropsychological performance or identifying biomarkers and possible interventions specific for this population.13,14
Environmental enrichment causes changes in neural signaling and plasticity that potentially slow or reduce this cognitive impairment.15,16 The impact of cognitive rehabilitation includes restoration of impaired function and/or induction of compensation for an area of deficit. 17 Computer-based cognitive rehabilitation programs are accessible and effective interventional tools for patients with known cognitive deficits. 18 While researchers have shown that cognitive rehabilitation improves outcomes in patients with known deficits, the utility of cognitive training as a preventative tool for CRCI has not been well studied, especially in AYACS.17,19,20
A variety of neurocognitive testing measures have been used to define cognitive abilities in cancer patients.13,21,22 Computer-based neurocognitive testing is an accessible, objective, and validated measure of cognition that, when trended prospectively and longitudinally, can detect and define acute and subacute cognitive changes.18,23,24 In addition to neurocognitive testing, biomarkers such as brain-derived neurotrophic factor (BDNF), which previously was demonstrated to correlate with cognitive impairment in studies of breast cancer patients, can be useful in monitoring the impact of cognitive rehabilitation in patients diagnosed with cancer.25,26
We designed this study to investigate the feasibility of cognitive rehabilitation as a preventative intervention for AYA patients receiving chemotherapy. We hypothesized that it is feasible for newly diagnosed patients, who were undergoing treatment, to successfully engage in a computer-based cognitive training program at least 80% of the goal training time, starting as early as 1 month after the initiation of chemotherapy. As an exploratory aim, we sought to determine whether cognitive performance of the treatment group will surpass that of the control group, both acutely and over time after completion of the cognitive training. This is an effort to enhance environmental enrichment to the brain by providing stimulation early on to slow down cognitive decline. Furthermore, we evaluated for correlation between changes in cognitive performance and serum levels of BDNF. By trending serum BDNF levels over the course of chemotherapy treatment and comparing them to performance on cognitive tests, we will assess whether computer-based cognitive training can enhance BDNF levels in AYA cancer patients.
Methods
Study design
We conducted a pilot prospective controlled study to show the feasibility of integrating an intensive computer-based cognitive rehabilitation program into the supportive therapy for AYA patients with newly diagnosed cancer requiring treatment with chemotherapy. This study was approved by the Children's Health care of Orange County (CHOC) Institutional Review Board (150535) before initiation.
Inclusion and exclusion criteria
The study included English-speaking patients 12–25 years old with a first diagnosis of cancer, necessitating treatment with chemotherapy. Participants may have required CNS-directed therapy in the form of lumbar punctures with chemotherapy or surgery as part of their treatment course. Exclusion criteria included previous diagnosis of developmental delay or cognitive deficits, prior exposure to chemotherapy or radiation, necessity of transplant, or a diagnosis of a brain tumor or presence of brain metastases.
Study procedures
Potential participants were initially contacted at the time of their first admission for chemotherapy related to their new cancer diagnosis. Enrollment in the study was allowed anytime up to 3 months from diagnosis. This was to provide time for patients and their families to adjust to a new diagnosis, recover from immediate side effects, improve their ability to focus on tasks, and be able to discuss enrollment and learn about potential benefits of the study in a more relaxed, outpatient setting. Once enrolled, participants were alternately assigned to the intervention or nonintervention arm through an odd/even method, in which participants enrolled with an odd number were placed in the intervention arm (Fig. 1).
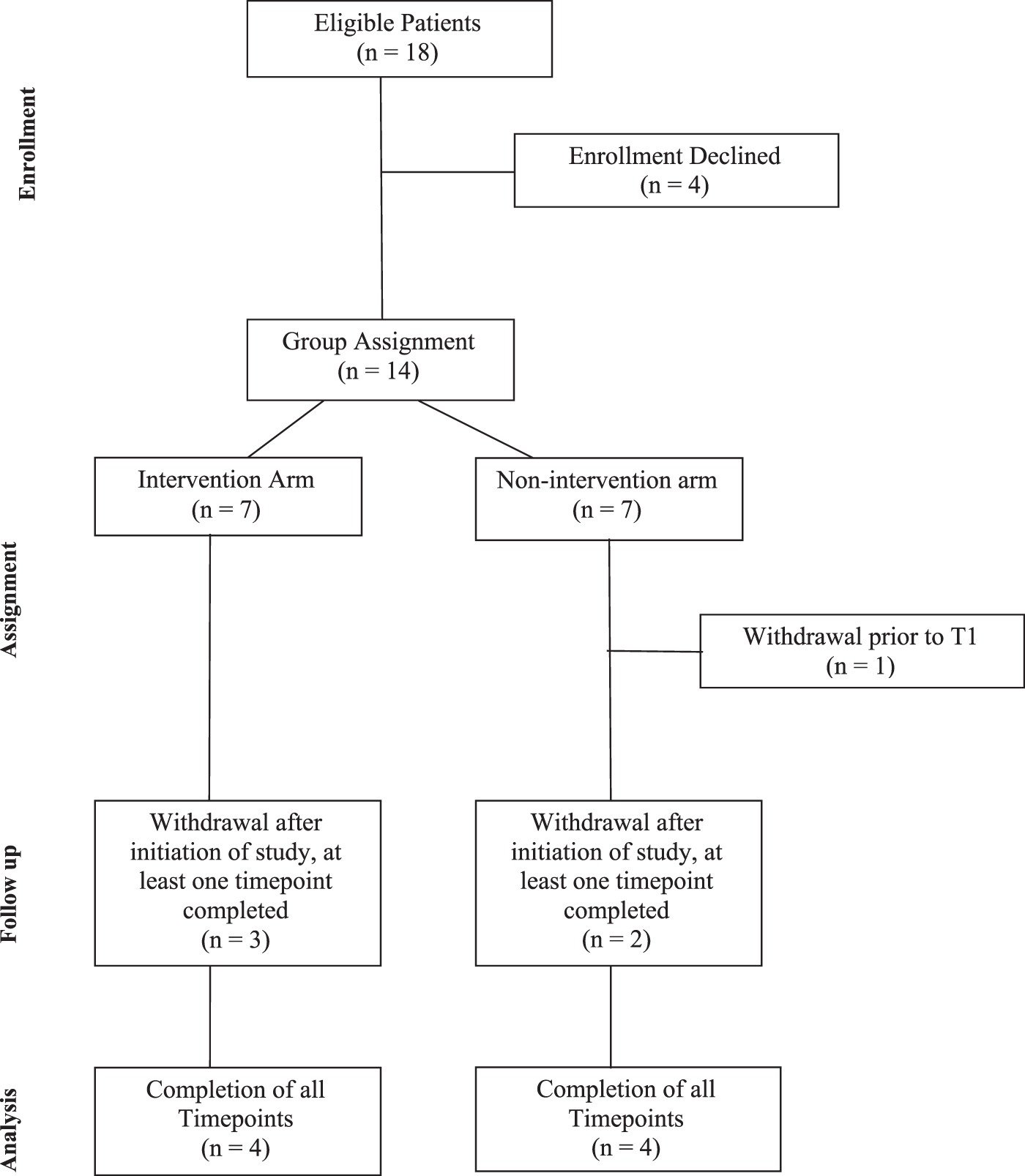
Consort diagram.
Participants in the intervention arm were asked to participate in computer-based cognitive activities (Lumosity, Inc.) for 20–30 minutes daily for 16 weeks following enrollment. 17 This program has been successfully utilized in prior studies to improve executive function skills in breast cancer survivors and pediatric patients with acquired brain injuries.27,28 Training included graded exercises focused on improving memory and attention. Once a task is mastered, exercise type and difficulty change to promote learning. Completion rates and a composite score were tracked by the program and available for researcher review. Participants who were assigned to the nonintervention arm continued with their daily activities such as playing video or computerized games.
Analysis
Completion rate of the neurocognitive training program, time spent training by each patient, and completion of study follow-up were considered measures of feasibility. Outcome measures of computerized neurocognitive testing and serum BDNF levels were obtained within the first month following diagnosis before cognitive rehabilitation (T1), as well as at ∼16 weeks (T2) and 24 weeks (T3) from enrollment and initiation of any intervention. Serum BDNF levels were quantified using the Human BDNF ELISA Kit (Proteintech, KE00096) according to the manufacturer's instructions, at a 1:25 dilution. Each sample was run in triplicate and all samples from a given patient were analyzed in the same plate to minimize run-to-run variability. At the end of the study, participants in the intervention arm and their parents filled out surveys regarding the feasibility of complying with these daily cognitive tasks.
Cognitive performance was objectively measured using a brief, well-published, and validated computerized neurocognitive test battery (CogState Ltd.), 24 which was previously utilized to conduct neuropsychological assessments in chemotherapy-related cognitive impairment clinical studies. 23 A customized battery of tests was completed in a quiet room with minimal distractions during a previously scheduled appointment, with testing duration lasting ∼20–30 minutes. The CogState tasks (cognitive domains assessed) in the customized battery include the following: (1) Keyboard Learning Tasks (warm up, to familiarize the patient with the testing environment), (2) Detection test (processing speed), (3) Identification test (visual attention), (4) One Card learning Test (visual learning), (5) One Back Test (working memory), and (6) Groton Maze Learning Test (executive function). There are two measures reported for the One Back Test, but the speed of performance is used for measuring the change over time. For any task for which a lower score indicates an improvement in performance, the difference from the mean baseline has been reversed (multiplied by −1) so that all outcome variables are uniformly directed. The primary outcome measure used in each respective CogState task was then standardized according to their age-specific normative data to create Z-scores for analysis. In this study, cognitive impairment is defined as having a z-score that was below 1.5 standard deviation from the normative mean at any assessed study time point (at T1, T2, or T3). This analytical approach was recommended by the International Cognition and Cancer Task Force, which has provided specific recommendations on the criteria to assess cognitive impairment in cancer studies. 29
Statistical analysis
Descriptive statistics were utilized to describe the demographic and clinical data. The proportions of cognitive impairment between the nonintervention and intervention arm were compared for each of the cognitive domains assessed by the respective CogState tasks. Intergroup comparisons of BDNF levels at each time point between intervention and nonintervention arms were conducted using Mann–Whitney U test, whereas comparison of BDNF levels across all time points for each individual arm was conducted using Friedman test. Post hoc analysis of BDNF levels between T1 and T2, T2 and T3, and T1 and T3 were conducted using Wilcoxon signed-ranked test. A p-value of <0.05 was considered statistically significant. Statistical analyses were conducted with the Stata version 16 software (StataCorp., College Station, TX).
Results
Demographics and clinical characteristics
A total of 18 eligible patients were approached, with 14 of those patients consenting to enroll in the study and 4 patients declining enrollment. Seven patients were assigned to the intervention arm and seven to the nonintervention arm (Table 1). One patient from the nonintervention arm was emotionally unable to participate and thus withdrew from the study before any data collection. The median age was similar between the two arms (16.5 years for the nonintervention arm vs. 15 years for the intervention arm, p = 0.38). Gender distribution was similar between the two arms (p = 0.85).
Baseline Demographics of Participants
Patient diagnoses included acute lymphoblastic leukemia (n = 3), Hodgkin's lymphoma (n = 2), germ cell tumor (n = 3), Ewing sarcoma (n = 1), colon cancer (n = 1), osteosarcoma (n = 3), and hepatocellular carcinoma (n = 1). Eight of the 13 enrolled patients were able to complete all the study points for follow-up, yielding a retention rate of 61.5%. Five patients withdrew, three of whom transferred to another institution, while two were too sick or felt unfit to comply with study procedures. Completion of all three time points was similar for both arms, with four patients completing all study follow-up time points in each arm.
Feasibility
Of the seven patients enrolled in the interventional arm, five completed the required activities (71%), that is, completion of at least 80% of the required activities. Two patients were not compliant. Patients were better able to engage in activities in between phases of chemotherapy compared to the times they were receiving treatment. The most common reason for not completing tasks noted by participants on both arms was because of not feeling well enough to stay focused. One participant on the intervention arm did not have reliable computer access at home, which posed difficulties with compliance.
Comparison of BDNF levels between intervention and nonintervention arms
There was a reduction of serum BDNF levels over time, and such reduction was observed in both intervention and nonintervention arms. The reduction was not statistically significant (Table 2). Of the eight patients who had all three time points measured, six patients demonstrated a decrease in BDNF levels over time. On average, there was a 33% decrease in BDNF levels from T1 to T3. All six patients who exhibited a decline in serum BDNF levels had solid tumors and had received significant amounts of aggressive chemotherapy by T3. The patients who showed an improvement in serum BDNF levels had diagnoses of Hodgkin's lymphoma (intervention arm) and hepatocellular carcinoma (nonintervention arm).
Comparison of Brain-Derived Neurotrophic Factor Levels Between Nonintervention and Intervention Group
No reliable reference range has been established for BDNF levels in the AYA population; however, studies in healthy adults have suggested various ranges of 32.69 ± 8.33 ng/mL, 25.5 ± 4.5 ng/mL, and 18.2 ± 4 ng/mL.33,34
AYA, adolescent and young adult; BDNF, brain-derived neurotrophic factor.
Comparison of cognitive impairment between intervention and nonintervention arms
A total of five domains were assessed for cognitive impairment, in comparison with the normal population (Table 3). Comparing the proportion of patients experiencing cognitive impairment, patients in the nonintervention arm demonstrated higher prevalence of impairment in three of the six cognitive domains (processing speed, visual attention, and working memory). The prevalence of impairment for the two cognitive domains (visual learning and executive function) was equal for both arms.
Proportion of Impairment by Each Individual CogState Test Scores Between Nonintervention and Intervention Group
LMN: measures the speed of performance by the mean of the log10 transformed reaction times for corrected responses.
ACC: measures the accuracy of performance by the arcsine square root of proportion correct.
For One Back Test, speed of performance should be used for measuring change over time.
For any test for which a negative difference score indicates an improvement in performance, the difference from mean baseline score has been reversed (multiplied by −1) to ensure all outcome variables are in a uniform direction.
ACC, accuracy of performance; LMN, speed of performance.
Discussion
This feasibility study was conducted to assess whether AYA patients were able to comply with completing computer-based tasks and games that are intended to prevent CRCI. Results from this pilot study provide some evidence that intensive online cognitive rehabilitation using computerized modules may be feasible. A reasonable number of newly diagnosed patients (71%) who were undergoing treatment were engaged in our cognitive rehabilitation for at least 80% of the goal training time. We also collected biomarker (BDNF) data from this feasibility study. While we hypothesize that this biomarker could serve as a future diagnostic tool for cancer survivors with cognitive impairment, we were unable to correlate the biomarker finding with the neuropsychiatric tests due to small sample size. Nonetheless, the results are encouraging, and the effectiveness of the intervention is worth evaluating in a larger study.
AYA survivors face unique challenges with identity, body image, and emotional well-being as diagnosis and treatment interrupt a key phase of psychosocial growth and development, profoundly affecting their QOL.6,30 The neurocognitive late effects among childhood cancer survivors have been well documented. 13 However, there is limited research examining the neurocognitive effects of cancer diagnosed in AYACS. 4 In our study, patients in the nonintervention arm demonstrated higher prevalence of impairment in three of the six cognitive domains (processing speed, visual attention, and working memory). Similarly, previous reports show that adaptive functioning in AYA patients depends on intelligence, processing speed, and executive functions. 7 Others have found that the AYA survivors may be at risk for executive function deficits, which can affect psychological adjustment and academic performance. 14
Despite the impact of cancer diagnosis and treatment, AYACS may demonstrate greater resilience to cognitive deficits than adult cancer survivors as a function of greater reserve (compensatory ability in which performance on cognitive tests is better than would be expected on the basis of degree of brain pathology) and neuroplasticity (the brain's ability to form new neural connections).6,31 Neuroplasticity is higher during critical periods of brain development, which may facilitate the establishment of compensatory pathways in AYAs. 32 These concepts are speculative and require validation.
In the intervention arm, computerized intervention improved scores in five of six variables tested. However, due to small sample size, we could neither ascertain if the improvement was limited to visual memory and processing alone nor could we conclude that the improvement resulted from the cognitive intervention. Reductions in cognitive impairment did not correlate with increased serum BDNF levels. Although the improvement in scores may be partially attributable to the repetitive nature of the intervention, some patients found this repetition nonstimulating, which may have resulted in boredom and lower scores. In addition, the observed improvement may reflect the decrease in disease burden as each patient progressed through treatment. The heterogeneity of diagnoses of enrolled participants meant that certain patients enrolled in the study had lower stage disease or diagnoses that required less intensive and shorter duration of therapy, with some having already completed treatment at the time of final evaluation. Others were still receiving intensive chemotherapy at the third time point, further affecting their ability to participate in cognitive rehabilitation. In addition, patients may require longer and persistent periods of active intervention over time to show meaningful changes and/or recovery. Future studies may aim to isolate these variables. Finally, as the computerized intervention was given to patients over a period of 16 weeks, it is unclear whether the benefits would last beyond the interventional period.
One of our planned aims was to trend serum BDNF with cognitive function to understand the potential use of BDNF as a biomarker for cognitive recovery. BDNF levels may be reflective of synaptic plasticity and neuroprotection in the young and developing brain.25,26 Interestingly, serum BDNF levels decreased in six of the eight patients for whom measurements were obtained at all three time points. As noted earlier, these six patients had solid tumors requiring intensive chemotherapy. Due to the small sample size, the existence of a correlation between BDNF levels and results on CogState testing could not be conclusively determined. Nonetheless, this preliminary finding may suggest that serum BDNF levels may be affected by the type, dose, and intensity of chemotherapy, and may take several months to years to recover. Notably, some of the study participants were symptomatic during the study period, requiring medications such as narcotics, antiemetics, and sedatives, which slow cognition. They may have also required additional medications that could affect BDNF levels, including antiepileptics, mood stabilizers, and selective serotonin reuptake inhibitors. Furthermore, it is difficult to know what degree of change in BDNF levels would correlate with an improvement in cognitive function. Therefore, it would be interesting to continue to trend BDNF levels as patients progress further through their treatment course and after treatment has completed, and consider external factors that may affect the levels. We postulate that as patients are further out from treatment, serum BDNF levels would begin to recover to pretreatment values. Serum BDNF needs to be further validated as a biomarker to indicate cognitive impairment and further studies exploring its properties and timing of recovery need to be undertaken.
This study has several limitations. Attrition and the study's small sample size pose significant challenges. Initially, patients were enrolled within the first 4 weeks of treatment in an attempt to obtain early assessment of baseline cognitive function, as well as to provide neurocognitive stimulation as early as possible. However, we found that due to the enormous challenges that patients faced at the commencement of treatment, even brief periods of cognitive intervention were difficult to implement as patients were often too sick to participate. Individual variability in psychosocial development, maturity, mental health issues, and education likewise presented challenges to attrition and engagement with cognitive rehabilitation. A patient's clinical status may have also affected the ability to collect data at specific times in therapy. Furthermore, during the first few weeks after diagnosis, patients and families were still coping with the physical and emotional burden of a life-threatening condition. This finding shows that to achieve better compliance, there is a need to balance the requirements of the intervention with other competing concerns, such as post-treatment symptoms, time demands, and motivational support from family.
Conclusion
In conclusion, this study provides some evidence that it may be feasible to implement cognitive intervention early in treatment for newly diagnosed cancer. Understanding goal-related processes relevant to AYAs may encourage engagement and participation. In the future, we plan to evaluate cognitive stimulation practices over 12 months or more after the initiation of intensive chemotherapy based on the findings of this study. We also plan to investigate how serum BDNF levels change throughout treatment, including effects of the type/dose of chemotherapy administered and the patient's clinical condition.
Footnotes
Acknowledgment
We would like to thank the CHOC-UCI Child Health Research Pilot Collaborative Grant for support of this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Funding provided by a pilot award from Children's Healthcare of Orange County-University of California Irvine Child Health Research Strategic Plan Steering Committee.