
Abstract
Purpose:
We conducted a questionnaire survey in 15 pediatric oncology hospitals in Japan to better understand the current status of fertility preservation in childhood and adolescents.
Methods:
The survey period was from September 2020 to December 2020. We mailed questionnaires to 64 departments involved in pediatric cancer treatments at the 15 hospitals. The primary outcomes were the timing of providing explanations on fertility preservation, presence of health care provider while providing explanations, cooperation between medical staff, and cooperation between hospitals.
Results:
The response rate was 100% (64/64). Regarding the time at which this information was provided, 79.6% of patients (43/54) received it before cancer treatment; 5.6% (3/54), after remission; and 14.8% (8/54), both time points. Nurses were mostly in attendance (70%) when oncologists provided information to patients. Nine (60%) hospitals did not have a reproductive department. Among these, 28.6% of the respondents referred patients to a reproductive facility that performed fertility preservation. Providing information about fertility preservation was challenging owing to the shortage of specific explanatory materials (35.1%) and the lack of cooperation between pediatric oncologists and reproductive endocrinologists (24.6%).
Conclusion:
Based on this survey, educational activities regarding fertility preservation centered on pediatric oncologists and nurses are needed. Furthermore, a system for providing explanatory materials for fertility preservation and encouraging cooperation at the physician and hospital levels is also needed (IRB No. H2020-111).
Introduction
With recent advances in cancer treatment, the prognosis of cancer patients aged <20 years (childhood and adolescents) has improved. 1 However, cancer treatments (chemotherapy and radiation-therapy) administered in childhood negatively affect gonadal tissues,2–4 and many pediatric cancer patients experience infertility in adulthood. Childhood cancer survivors have a 1.48-fold higher risk of infertility than their siblings. 5 Therefore, fertility preservation techniques such as sperm cryopreservation in male adolescents after puberty and cryopreservation of oocytes and ovarian tissue in female adolescents are performed worldwide. 6 However, pediatric fertility preservation is difficult to explain to children considering their cognitive development and comprehension level. Therefore, a collaboration between pediatric oncologists and reproductive endocrinologists is important.
In Japan, the Ministry of Health, Labor, and Welfare has established 15 government-designated core hospitals for pediatric cancer treatment (Children's cancer core hospital) in 7 regional blocks to provide pediatric cancer treatment and established a system wherein these hospitals cooperate with other pediatric cancer treatment hospitals. 7 However, there are disparities in the provision system for fertility preservation at these hospitals. There are also differences in the services of fertility preservation provided between blocks. 8 Information and medical opportunities for fertility preservation should be provided equally to pediatric cancer patients, and a system for this purpose is needed. In Japan, public financial support for fertility preservation began in 2021, providing significant backing from the government. Therefore, we need to identify and solve issues to address these disparities.
This survey aimed to understand the current status of fertility preservation among pediatric cancer patients in Japan. This study was funded by a Health Labor Sciences Research Grant. The primary outcomes were the time at which fertility preservation was explained to the guardians, the presence of a health care provider while providing explanations, and the status of cooperation between medical staff and between hospitals. Our study results will help establish systems for solving issues regarding pediatric oncofertility in Japan, thereby improving the practice of pediatric fertility preservation.
Materials and Methods
Data collection method
This study was conducted with the approval of the Clinical Research Ethics Review Committee of Mie University Hospital (No. H2020-111). The survey was conducted in 64 clinical departments involved in pediatric cancer treatments at 15 Children's cancer core hospitals in Japan. The departments included pediatrics, obstetrics and gynecology, hematology, urology, orthopedics, and neurosurgery. In some facilities, only one department oversaw chemotherapy; in such cases, we obtained only one reply. We mailed the questionnaire to the department chairs in September 2020, and the deadline for receiving the responses was December 2020.
Questionnaire
The questionnaire was designed after consulting our group of oncologists, pediatricians, and gynecologists, including reproductive endocrinologists. The questionnaire included 22 items (some were multiple-choice items) to assess the timing of explaining the impact of cancer treatment on fertility and fertility preservation for the patients and their guardians (before, during, or after cancer treatment), the physician in charge of explaining, the types of health care provider attendants, the point of difficulty in explaining, and the place and timing of consultation with the reproductive endocrinologist (within the same hospital or in another facility) (Supplementary Data). For pediatric patients, we assessed whether the pediatric oncologists would provide an explanation to the patient, depending on whether the patient was old enough to understand. The main outcomes were the time to explain the fertility preservation to the patient, health care provider presence at the explanation, and the status of cooperation among the medical staff and among the hospitals. As some children's cancer core hospitals did not perform fertility preservation, the items in the latter half of the questionnaire were answered separately according to whether the hospital had a reproductive department. For multiple-choice responses, the percentage was the number of selections per number of respondents.
Data analysis
The analysis of the raw questionnaire data included the following steps.
Of the raw data that we were able to collect, we adopted items that had corresponding responses to the questionnaire. The percentage of the questionnaire was the number of items for which that option was selected among the respondents for that item. Items that allowed multiple answers were defined by the percentage of respondents who selected that option out of those who answered the questionnaire for that item. The denominator indicates the number of respondents who responded to a particular question because the respondents did not respond to all items.
Results
Survey response rates
We were able to collect the questionnaires from all clinical departments at all hospitals (64/64). The percentages of respondents from various departments were as follows: 14.1% (9/64) in pediatrics; 12.5% (8/64), obstetrics and gynecology (including reproductive endocrinology); 14.1% (9/64), orthopedics; 12.5% (8/64), urology; 14.1% (9/64), neurosurgery; 7.8% (5/64), hematology; 6.3% (4/64), oncology; 12.5% (8/64), hematology/oncology; 4.7% (3/64), gastroenterology; and 1.6% (1/64), pediatric surgery.
Explanation and information of fertility preservation for pediatric cancer patients
The guidelines of the Japan Society of Clinical Oncology recommend the provision of information on fertility preservation. 9 However, not all pediatric cancer patients and their guardians are provided with information about fertility preservation before aggressive chemotherapy. Therefore, we evaluated whether they had been provided information on fertility preservation. Regarding when this information was provided, 79.6% (43/54) of patients and their guardians received it before cancer treatment (10 missing); 5.6% (3/54), after remission; and 14.8% (8/54), both time points (Fig. 1).

Bar graph showing when patients and guardians are informed of the effects of chemotherapy on fertility. Patients and guardians are typically informed of the effects of chemotherapy on fertility before treatments that have effects on gonadal function (11 missing).
Differences depending on patient age
It is necessary to optimize the content of explanations considering the cognitive development and understanding level of the patient 10 and improve the explanations provided to the guardians. As we believed that patients might be able to understand starting from the age at which primary education begins, the questionnaire was divided by the age of the pediatric patients as follows: 6–9, 9–12, and >12 years old. For patients who were 6–9 years old, the percentages of patients receiving no explanation, explanation to guardians only, and explanation to pediatric patients and their guardians were 24.5% (12/49), 51.0% (25/49), and 24.5% (12/49), respectively (15 missing). For patients who were 9–12 years old, the percentages were 20.4% (10/49), 34.7% (17/49), and 44.9% (22/49), respectively (15 missing). For patients who were >12 years old, the percentages were 10.7% (6/56), 1.8% (1/56), and 87.5% (49/56), respectively (8 missing) (Fig. 2).
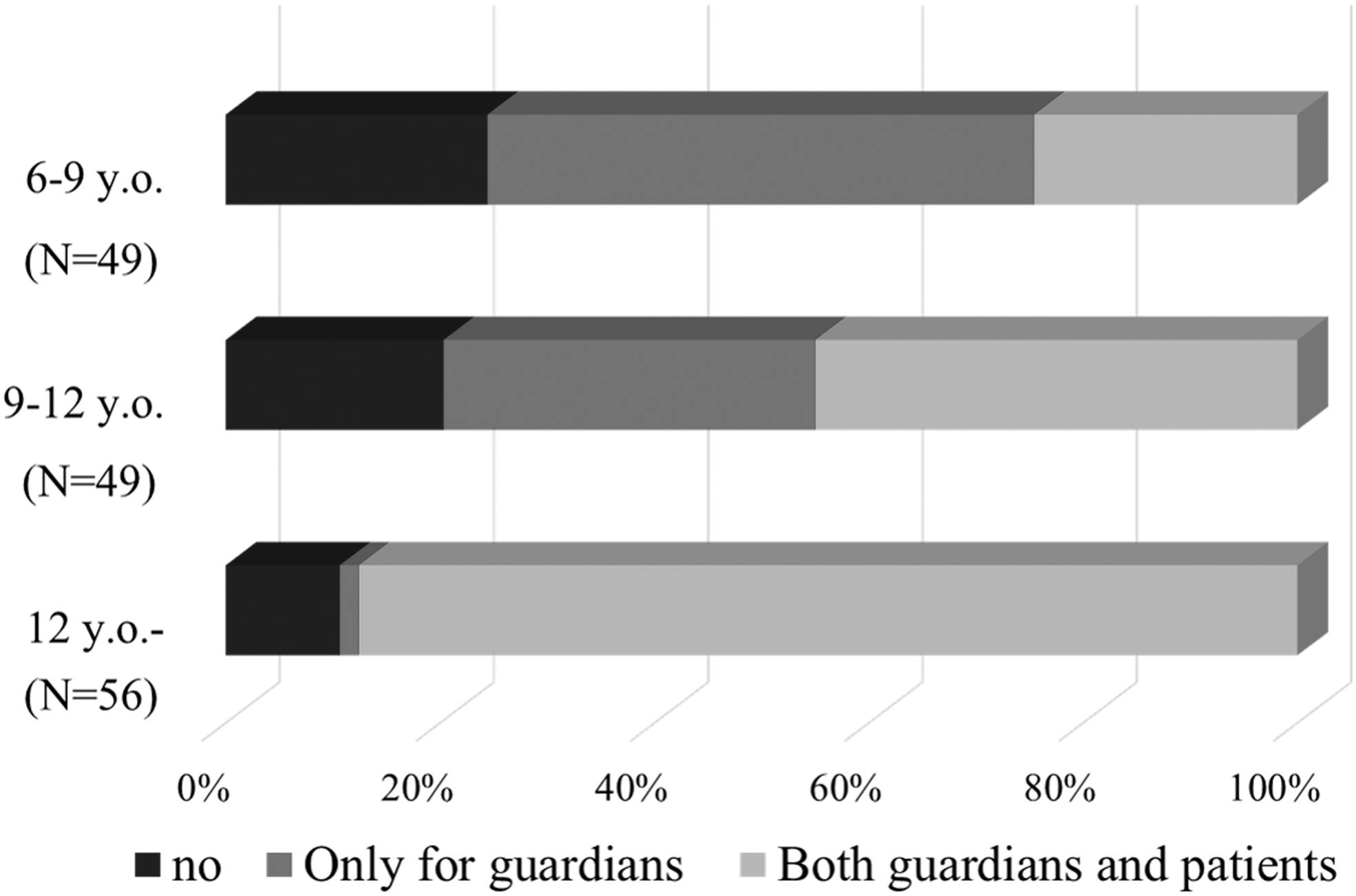
Bar graph showing whether doctors explain the effects of cancer treatment on fertility to patients and their guardians. As the age of the patient increases, the opportunity to explain to the patient himself increases. (6-9 y.o. age group, 15 missing responses; 9-12 y.o., 15 missing responses; >12 y.o., 8 missing responses). y.o., year-old.
Type of departments that provided explanations to patients and their guardians, and health care providers who were present during this process
The first physician who explained to male patients was the oncologist in 87.0% (47/54) of cases; reproductive endocrinologist, 5.6% (3/54); and others, 7.4% (4/54; 10 missing). The oncologist was the first physician to explain to female patients in 83.3% (50/60) of cases; reproductive endocrinologist, 5.0% (3/60); and others, 11.7% (7/60; 4 missing) (Fig. 3). In addition, nurses were the most frequent attendees at the briefing, accounting for ∼70% (Fig. 4).
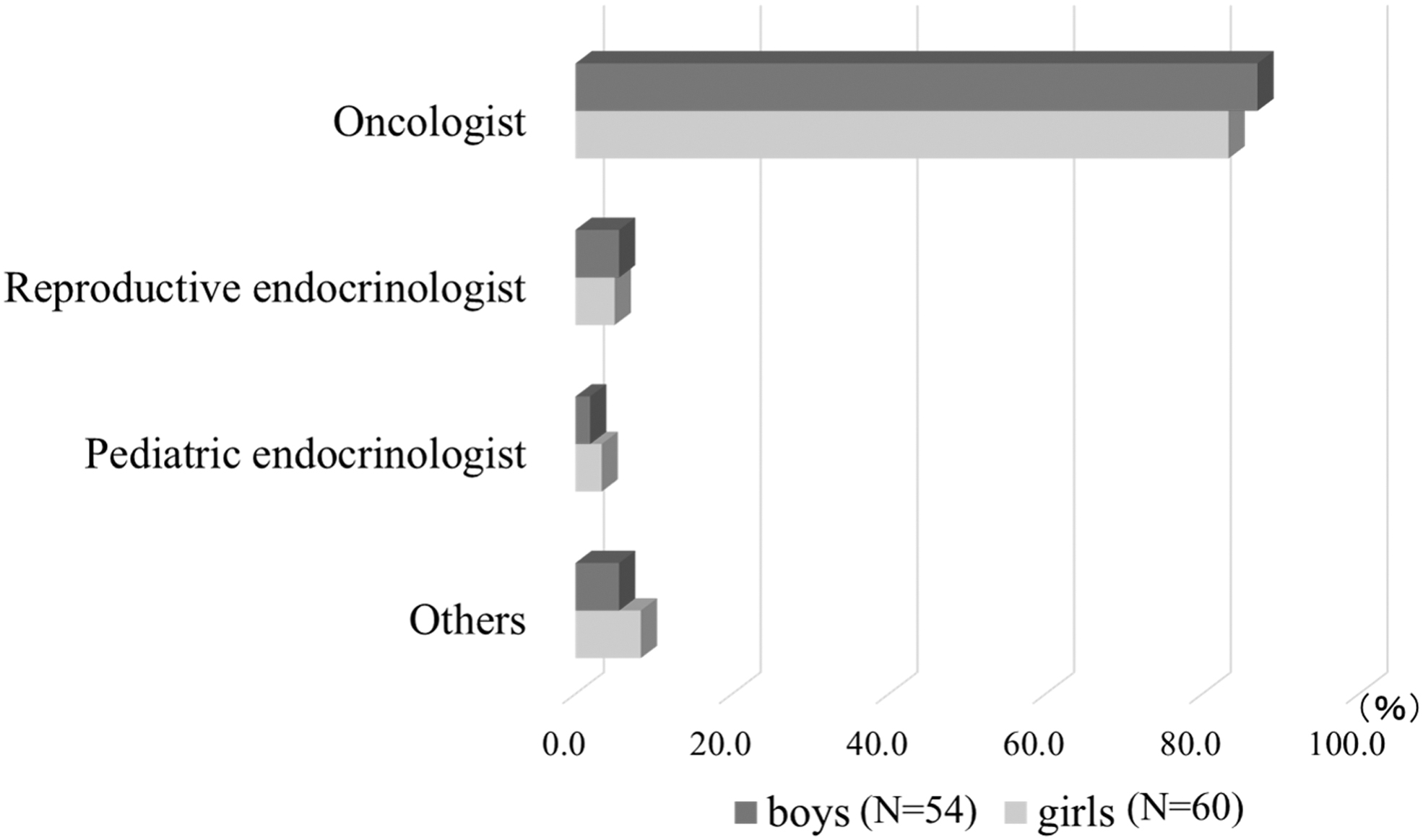
Bar graph showing the type of doctors who are first to explain fertility preservation to parents. Separate answers for boys and girls. Many oncologists are the first to explain fertility to patients (boys, 10 missing; girls, 4 missing).

Bar graph showing who is present during explanations of fertility preservation to guardians and patients. Nurses are most likely to be present when explaining fertility preservation to patients and guardians (11 missing).
Timing of explanation on fertility preservation and specific recipients of information
We assessed the specific recipients of information according to the time point of provision. Explanations were provided before treatment to guardians only in 77.4% (41/53) of cases, and to patients and their guardians in 69.8% (37/53) of cases (11 missing). Explanations were provided during treatment (information was not given for initial treatment with less impact on fertility but before changing to aggressive treatment) to guardians only in 34.0% (18/53) of cases and to patients and their guardians in 39.6% (21/53) of cases. Explanations were provided after treatment (when the disease had subsided, regardless of the effects of treatment on fertility) to guardians only in 3.8% (2/53) of cases and to patients and their guardians in 17.0% (9/53) of cases. It was considered appropriate to provide the information either before starting or during cancer treatment. However, it is worth noting that 17.0% (9/53) of patients received the explanation only after treatment (Fig. 5).
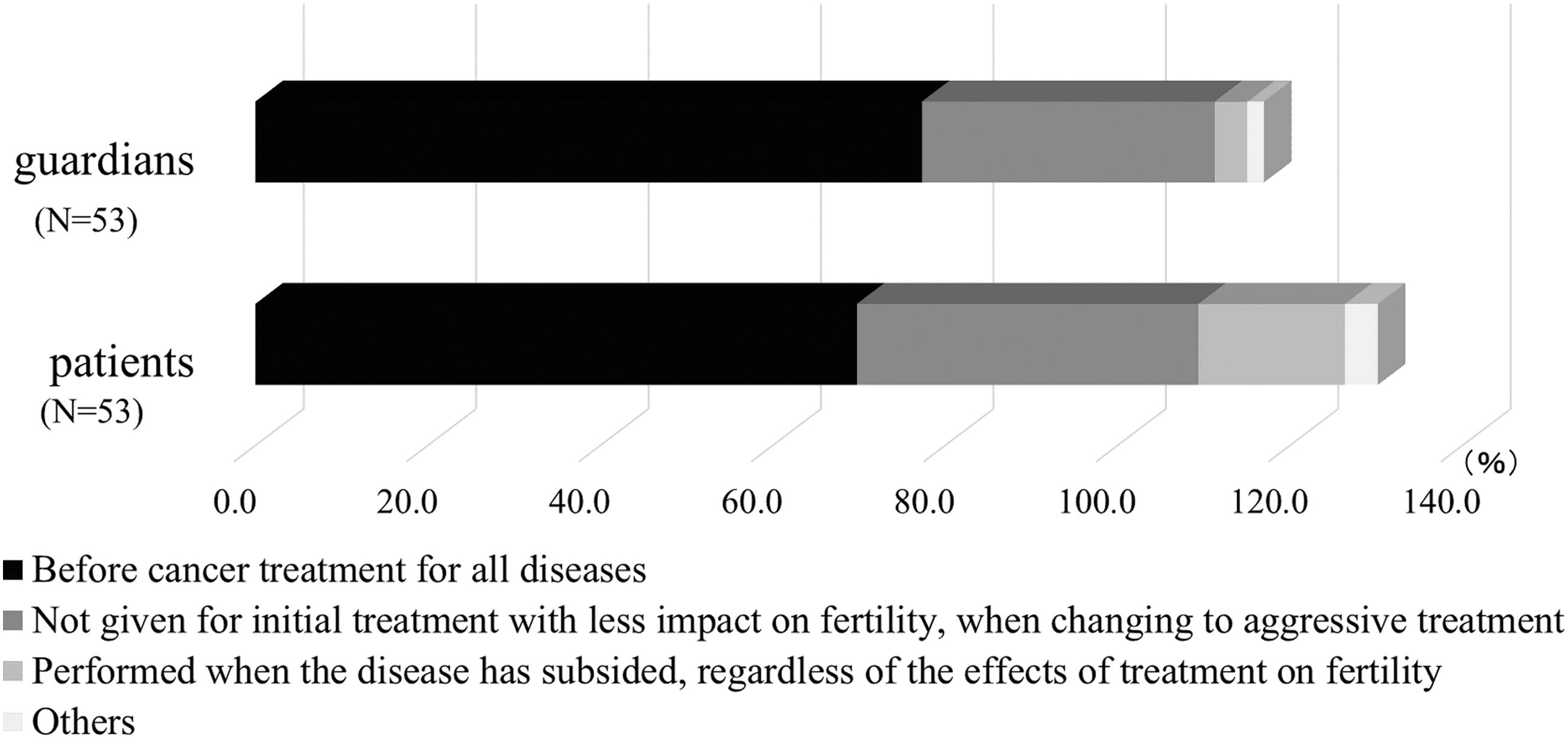
Bar graph showing when fertility preservation is explained to guardians and patients. Most patients and their guardians receive aggressive pre-treatment explanation of fertility preservation, but 17.0% have a doctor who explains it to them when they are settled into treatment (11 missing).
Differences in collaboration with reproductive endocrinologists depending on whether there was a reproductive department in the hospital
Fertility preservation is mainly performed by reproductive endocrinologists, but some children's cancer core hospitals may not have reproductive departments that perform fertility preservation. Among all children's cancer core hospitals in Japan, six had reproductive departments and nine did not have them. In hospitals that do not have a reproductive department, collaboration with reproductive endocrinologists at other hospitals is necessary. Therefore, we evaluated the collaboration between pediatric oncologists and reproductive endocrinologists depending on whether their hospitals had reproductive departments or not (11 missing). The percentages of oncologists who consulted a reproductive endocrinologist before explaining to patients and their guardians were 25.0% (8/32) and 19.0% (4/21) in hospitals with and without reproductive departments, respectively (Fig. 6). The percentages of respondents who consulted a reproductive endocrinologist after explaining cancer treatment to patients and their guardians were 50.0% (16/32) and 61.9% (13/21) in hospitals with and without reproductive departments, respectively. Those who consulted reproductive endocrinologists both before and after explaining accounted for 25.0% (8/32) and 19.0% (4/21) of the respondents with and without reproductive departments, respectively. Finally, 6.3% (2/32) and 28.6% of respondents from hospitals with and without a reproductive department, respectively, consulted a reproductive endocrinologist after the cancer treatment plan was finalized (Fig. 6).

Bar graph showing when reproductive endocrinologists are consulted about fertility preservation. In facilities with reproductive departments, 12.5% (2/16) of oncologists consult with reproductive endocrinologists after explaining fertility preservation to the patient, compared with 38.5% (5/13) of oncologists in facilities without reproductive departments. As many as 28.6% (6/21) of the oncologists in facilities without reproductive department consult reproductive endocrinologists after deciding on fertility preservation (11 missing).
Issues in explanation
Although awareness of fertility preservation in Japan has increased since the publication of specific Japanese guidelines in 2017, 9 it is still far from optimal. Additionally, providing information on fertility preservation for pediatric cancer patients requires dedicated materials. Since this material is intended for children, it is necessary to optimize the explanatory content for each age group. Therefore, we assessed the issues regarding the delivery of information. Lack of materials was the most common difficulty experienced by pediatric oncologists who delivered information (35.1%; 20/57), followed by lack of cooperation among pediatric oncologist and reproductive endocrinologist (24.6%; 14/57; 7 missing). Lack of awareness among oncologists was reported by 14.0% of respondents (8/57); lack of time for explanation due to oncologists' busy schedules, 12.3% (7/57); and oncologists' lack of knowledge about fertility preservation, 8.8% (5/57) (Fig. 7).
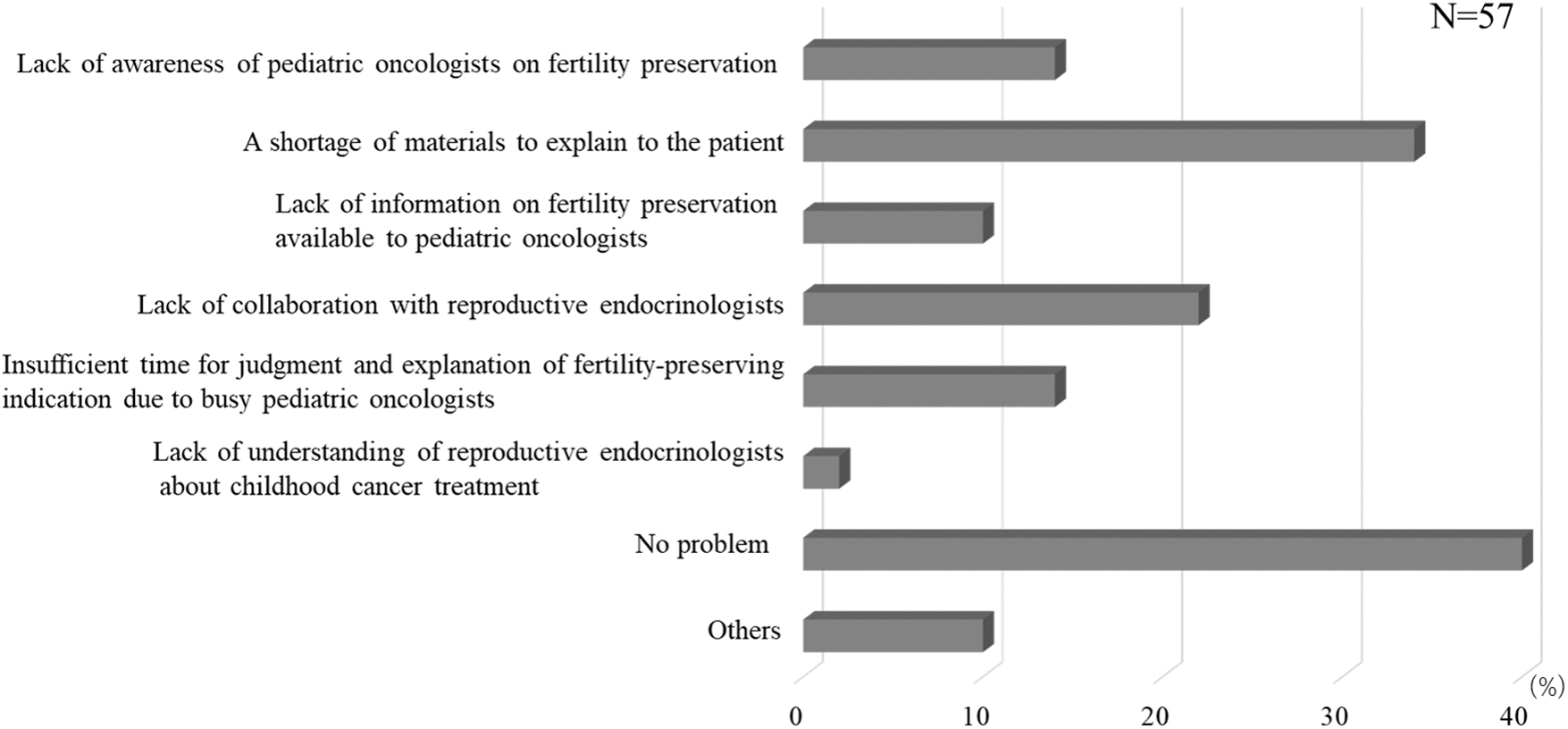
Bar graph showing the barriers to the explanation of fertility preservation. Lack of materials to explain to patients has become a major problem (7 missing).
Materials for fertility preservation
The lack of materials to explain fertility preservation to pediatric cancer patients was a concern, and we thought it was important to solve this issue to spread fertility preservation in Japan. Therefore, we assessed which materials were used for explaining fertility preservation. Use of no explanatory materials was reported by 18.2% (6/33) and 40.9% (9/22) of respondents from hospitals with and without reproductive departments, respectively (9 missing). Having their own materials was reported by 33.3% (11/33) and 18.2% (4/22) of facilities with and without reproductive departments, respectively; 36.4% (8/22) of facilities without reproductive departments that provided explanations about fertility preservation used materials prepared by academic societies or other facilities. Additionally, 33.3% (11/33) and 4.5% (4/22) of respondents from hospitals with and without reproductive departments, respectively, were unable to confirm or were unsure of the materials used (Fig. 8).
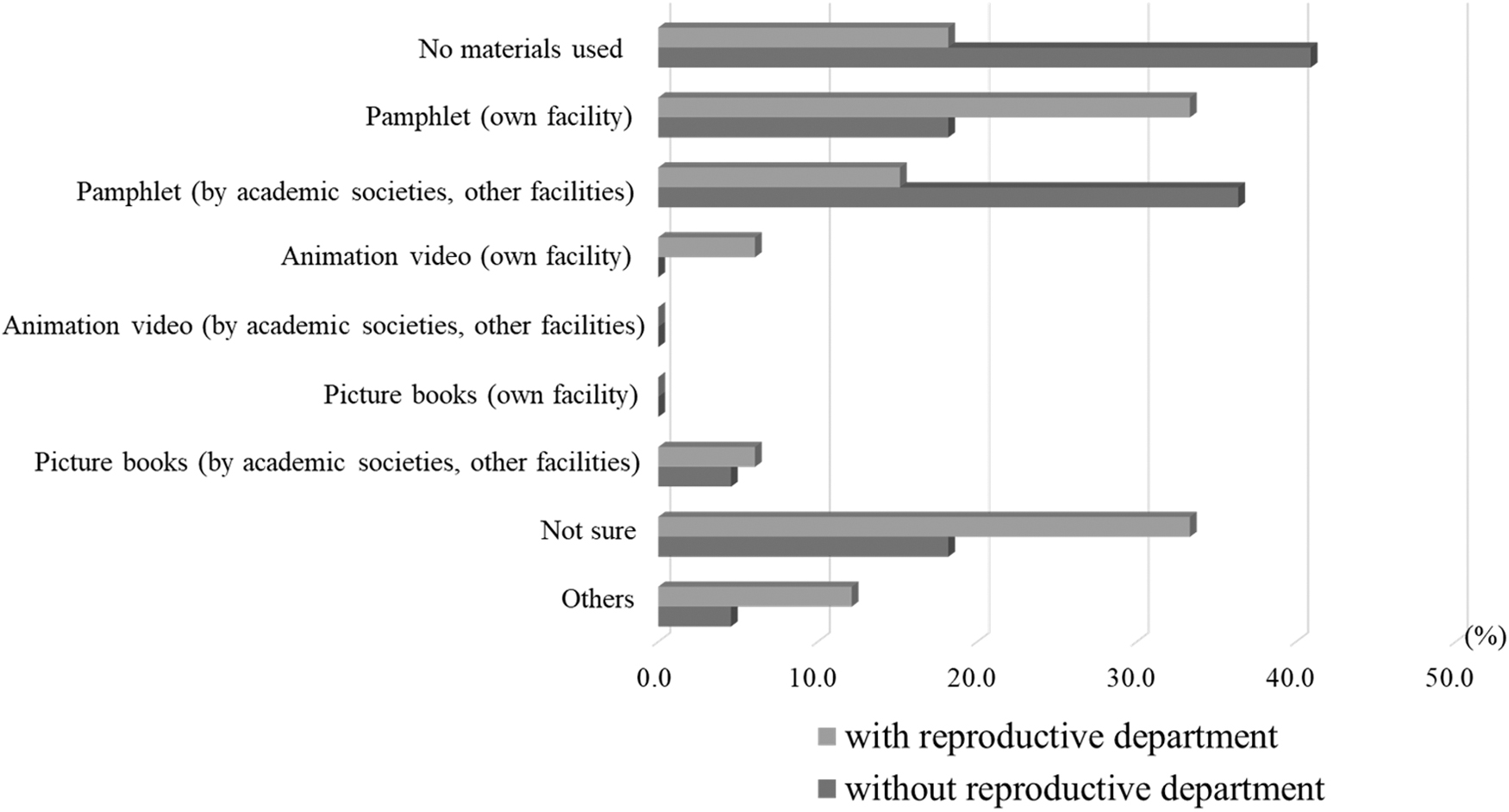
Bar graph showing the type of materials that are used to explain fertility preservation in detail. In facilities without fertility preservation facilities, there are no explanatory materials or explanatory materials issued by academic societies are used (9 missing).
Discussion
Regarding fertility preservation for pediatric cancer patients, sperm cryopreservation is selected after puberty for boys, while ovarian tissue and oocyte cryopreservation is selected for girls. 11 However, many issues are associated with fertility preservation for pediatric cancer patients, such as age-dependent lack of understanding, importance of providing explanations to guardians, lack of knowledge about fertility preservation among oncologists, and lack of collaboration with reproductive endocrinologists. Additionally, for pediatric patients, cancer treatment may be conducted at a specialized pediatric hospital without a reproductive department, requiring patient transfer to a different hospital for fertility preservation. Guardians of pediatric cancer patients were provided information on the impact of cancer treatment on gonadal function, but 17% of the explanations to patients were provided only after remission (Fig. 1). Oncologists commonly provide information about fertility preservation according to the patient's condition. However, because aggressive cancer treatments are likely to affect gonadal function, 12 it is important to disseminate correct information and aim for early fertility preservation in such cases. In a 2016 survey involving pediatric oncologists in Japan, only about 60% of respondents explained the impact of treatment on fertility before cancer treatment, 13 indicating an improvement in awareness. One reason is the rising awareness among oncologists and patients due to the release of the guidelines in 2017. 9 However, there are issues to be resolved to improve the awareness further.
In explaining fertility preservation to pediatric cancer patients, the proportion of patients receiving information increased with patient age (Fig. 2). These results suggest that pediatric oncologists often perceive that only cancer patients aged ≥12 years are able to understand disease- and fertility preservation-related information. Generally, the age at which children can fully understand informed consent is reported to be ≥11.2 years. 14 Moreover, it is important for younger pediatric cancer patients to consent to fertility preservation,15–17 suggesting the need for improvements in terms of the explanation provided.
In most cases, oncologists were the first to explain fertility preservation to pediatric cancer patients (Fig. 3). After informing the patient of the disease name, the oncologist explained the future cancer treatment plan. Most of the oncologists explained the side effects of chemotherapy in this situation and the impact of the treatment on fertility. Furthermore, some oncologists consulted reproductive endocrinologists in this situation. Besides oncologists, the health care providers most often present at the explanation of fertility preservation were nurses (Fig. 4). Cancer patients perceive a nurse as someone who looks after them rather than as someone who advocates for their rights when making decisions about cancer treatment options, and they expect physical and psychological support related to diagnosis and treatment. 18 Contrastingly, nurses involved in oncofertility in Japan are aware of the lack of experience and knowledge about fertility preservation and lack of educational opportunities. 19 A proper educational program for nurses would allow them to develop a positive attitude and change their mindset. 20 Therefore, it was suggested that if nurses could be provided with opportunities to educate themselves about fertility preservation, they might be able to more actively support patients' decisions to preserve their fertility.
Because some chemotherapy treatments have a significant negative impact on fertility, 12 the opportunity for fertility preservation should be provided before cancer treatment is initiated. 9 Therefore, the timing of providing explanations regarding fertility preservation is important. Most patients and their guardians were informed about fertility preservation before the cancer treatment was initiated (Fig. 5). In contrast, there were a few explanations after remission, a stage at which fertility preservation might not be possible due to the progression of cancer treatment. Additionally, in Japan, there are many cases where cancer treatment departments and reproductive departments are not colocated. It is understandable that explanations differed based on consideration of each patient's condition, but our findings suggest that oncologists need to change their mindset.
Some children's cancer core hospitals in Japan are solely dedicated to pediatric oncology and do not have a reproductive department. We evaluated the difference in the timing of the explanation to patients depending on whether the hospital had a reproductive department or not (Fig. 6). The percentage of oncologists who consulted with a reproductive endocrinologist before explaining fertility preservation to their patients was higher in hospitals with reproductive departments than in those without them. This suggests that there is a difference in the collaboration between oncologists and reproductive endocrinologists depending on whether the hospital has a reproductive department or not. In Japan, there are many cases where cancer treatment and reproductive departments are not colocated, suggesting the need to establish a system for collaboration between them. Additionally, consultation with a reproductive endocrinologist was more likely to happen after the explanation of cancer treatment, regardless of whether the hospital had a reproductive department, because oncologists need to consult with reproductive endocrinologists at other institutions after determining the possibility of fertility preservation for cancer patients. Additionally, the percentage of patients who consulted a reproductive endocrinologist after deciding on a cancer treatment plan was approximately three times higher in hospitals without reproductive departments than in those with them (Fig. 6). This suggests that there may be a lack of knowledge about fertility preservation among oncologists. Therefore, oncologists working at cancer treatment facilities without reproductive departments may need to be educated about fertility preservation.
To promote fertility preservation among pediatric cancer patients, we need to address the obstacles preventing pediatric oncologists from explaining effectively (Fig. 7). We found that the most common reason cited by them was the lack of explanatory materials for fertility preservation. When we evaluated the materials used in explanations, the number of respondents who did not use any materials was about three times higher in facilities without reproductive departments than in those with them (Fig. 8). This is because hospitals with reproductive departments have materials prepared by their own hospitals, while hospitals without them use materials prepared by related societies or other facilities. Provision of appropriate materials can improve the knowledge of patients and their guardians, 21 and to promote fertility preservation in nonadjunct hospitals, there is a need for relevant academic societies to prepare materials on fertility preservation. Pediatric cancer patients should be given adequate information about fertility preservation, regardless of the institution in which they are being treated. 9 As it is difficult for children to obtain information regarding fertility on their own and since it is up to guardians and health care providers to provide this information, standardized explanatory materials could be a useful tool. The next most common comment was the lack of cooperation with reproductive endocrinologists. We suggest that the key to the future of pediatric oncofertility is the establishment of a collaborative system between oncologists and reproductive endocrinologists.
Conclusions
This survey clarified the issues regarding the explanation of fertility preservation in children's cancer core hospitals. To solve these issues, it is important to establish a system of cooperation between oncologists and reproductive endocrinologists. Additionally, our findings show the importance of related societies preparing materials for fertility preservation. It is important to provide focused educational opportunities for oncologists and nurses to facilitate the explanation and implementation of fertility preservation. In Japan, public financial support for fertility preservation began in 2021 by the Japanese government, and interest in this field is increasingly growing. However, various issues, such as those raised in this survey, need to be discussed and resolved with health care providers, related academic societies, relevant ministries and agencies, and local governments.
Footnotes
Acknowledgment
This study was conducted with the approval of the Clinical Research Ethics Review Committee of Mie University Hospital (No. H2020-111).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by MHLW Research for Promotion of Cancer Control Program Grant (19EA1015) awarded to N.S.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.