
Abstract
Purpose:
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) is an established treatment predominantly for malignancies. Chronic graft-versus-host disease (cGVHD) is the leading long-term complication after allo-HSCT, but knowledge on cGVHD and health-related quality of life (HRQOL) in long-term survivors of allo-HSCT performed in childhood, adolescence, and young adulthood (CAYA) is scarce.
Therefore, we aimed to (1) assess prevalence and risk factors of active cGVHD using the 2014 National Institutes of Health-Consensus criteria, (2) investigate associations between cGVHD severity, patient-reported symptom burden, and HRQOL, and (3) compare HRQOL of survivors to population norms.
Methods:
We conducted a nationwide cross-sectional study in long-term survivors of CAYA allo-HSCT combining clinical examinations and patient-reported outcome measures.
Results:
We included 103 survivors, 55 (53%) females, median age of 19.6 years [range 0.3–29.9] at HSCT, 16.8 years [6.0–32.0] from HSCT, and 77 (75%) with underlying malignancy. Overall, 32 (31%) survivors were diagnosed with active cGVHD. The risk of active cGVHD was increased with prior acute GVHD and reduced with in vivo T cell depletion. cGVHD severity was associated with increased symptom burden, but not with adverse HRQOL. Compared to Norwegian population norms, allo-HSCT survivors reported significantly lower HRQOL.
Conclusion:
These results indicate a high prevalence of cGVHD in long-term survivors of CAYA allo-HSCT. Although we did not find an association between cGVHD severity and HRQOL, survivors reported significantly poorer HRQOL compared to population norms. Knowledge on the long-term consequences of cGVHD will be important for optimizing treatment and long-term follow-up care after CAYA allo-HSCT.
Introduction
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) is an established treatment option for various conditions, including hematological diseases, congenital metabolic disorders, and immune deficiencies. The most common indication is malignant hematological diseases.
Chronic graft-versus-host-disease (cGVHD) is a major cause of morbidity and mortality after allo-HSCT and the leading long-term complication in transplant survivors.1–5 It is a multisystem allo-immune disorder that can cause irreversible organ damage, impaired functional status, and reduced health-related quality of life (HRQOL).6–8 Between 20% and 50% of allograft recipients develop cGVHD.9–11 Most patients are diagnosed within the first year of allo-HSCT, but 5%–10% are diagnosed later. 12 Among those who require systemic treatment for cGVHD, one third are still on immunosuppressants after 5 years. This emphasizes the long-term nature of cGVHD.13,14
In 2005, the National Institutes of Health (NIH) Consensus Conference proposed new criteria and standardized tools for diagnosing, grading, and reporting on cGVHD. 15 Clinical manifestations, rather than time of onset, were used as criteria for cGVHD. 16 The NIH-Consensus Criteria (NIH-criteria) were revised in 2014 to provide greater specificity and more accurate measures of the global burden of diseases attributed to cGVHD. 17 The changes included modification of diagnostic criteria for involvement of mouth, eyes, genitals, and lungs, as well as adjustments of organ severity score.
Despite the advances in transplant practices (i.e., improved supportive care, donor matching, alternative stem cell source, conditioning regimens, and GVHD-prophylaxis) over the last decades, cGVHD remains an important challenge.9,14 With an increasing population of survivors,18,19 focus on the long-term impact of cGVHD is important for optimizing the outcome and care of survivors.
The patients' own perceptions of their health may differ from the evaluations by clinicians.20,21 Therefore, it is essential to include patient-reported outcome measures (PROMs) as they provide valuable information on the patients' perspective.7,14,22–24 A common strategy when choosing among different PROMs is to include both a disease-specific and a generic measure. A disease-specific measure captures symptoms and functions especially relevant for the population at stake. In contrast, a generic measure is not specific for a particular population or disease and allows for comparison with the general population.
There is growing literature on cGVHD in adult HSCT recipients, but studies on those who were treated during childhood, adolescence, and young adulthood (CAYA) are limited. To our knowledge, few investigators have combined the 2014 NIH-criteria and PROMs when evaluating long-term survivors of CAYA allo-HSCT. This group of young survivors is of particular interest as they underwent treatment at a vulnerable time of growth and development. Given their potentially long life expectancy, the consequences of cGVHD and other late-effects could be of great concern.
Our main aim was to assess the prevalence and risk factors of active cGVHD diagnosed by the 2014 NIH-criteria in a population of Norwegian long-term survivors of CAYA allo-HSCT. In addition, we aimed to investigate the associations between cGVHD severity (diagnosed by the 2014 NIH-criteria) and patient-reported symptom burden and HRQOL, and finally, to compare the HRQOL of HSCT survivors to the Norwegian population norms.
We hypothesized that the prevalence of active cGVHD is high in long-term survivors of CAYA allo-HSCT, and that the severity of cGVHD is associated with increased symptom burden and adverse HRQOL.
Patients and Methods
Study population
The study was conducted as a population-based cross-sectional, multidisciplinary study (The Norwegian Allo Survivorship Study in long-term survivors after HSCT) at Oslo University Hospital (OUH), the principal transplant center in Norway. The overall aim was to assess the prevalence of active cGVHD and other late effects in long-term survivors of CAYA allo-HSCT.
We used the hospital HSCT registries to identify transplanted patients. Eligible survivors were those who underwent allo-HSCT <30 years of age, >16 years of age at inclusion, and >5 years beyond HSCT (Fig. 1). We included all diagnoses, except mucopolysaccharidosis type 1 since these patients, due to their primary disease, may have multiorgan pathology that could affect the outcomes of interest. 25 The study was approved by the Data Protection Officer at OUH and the Regional Committee for Medical and Health Research Ethics South-East Norway. All participants provided signed informed consent.
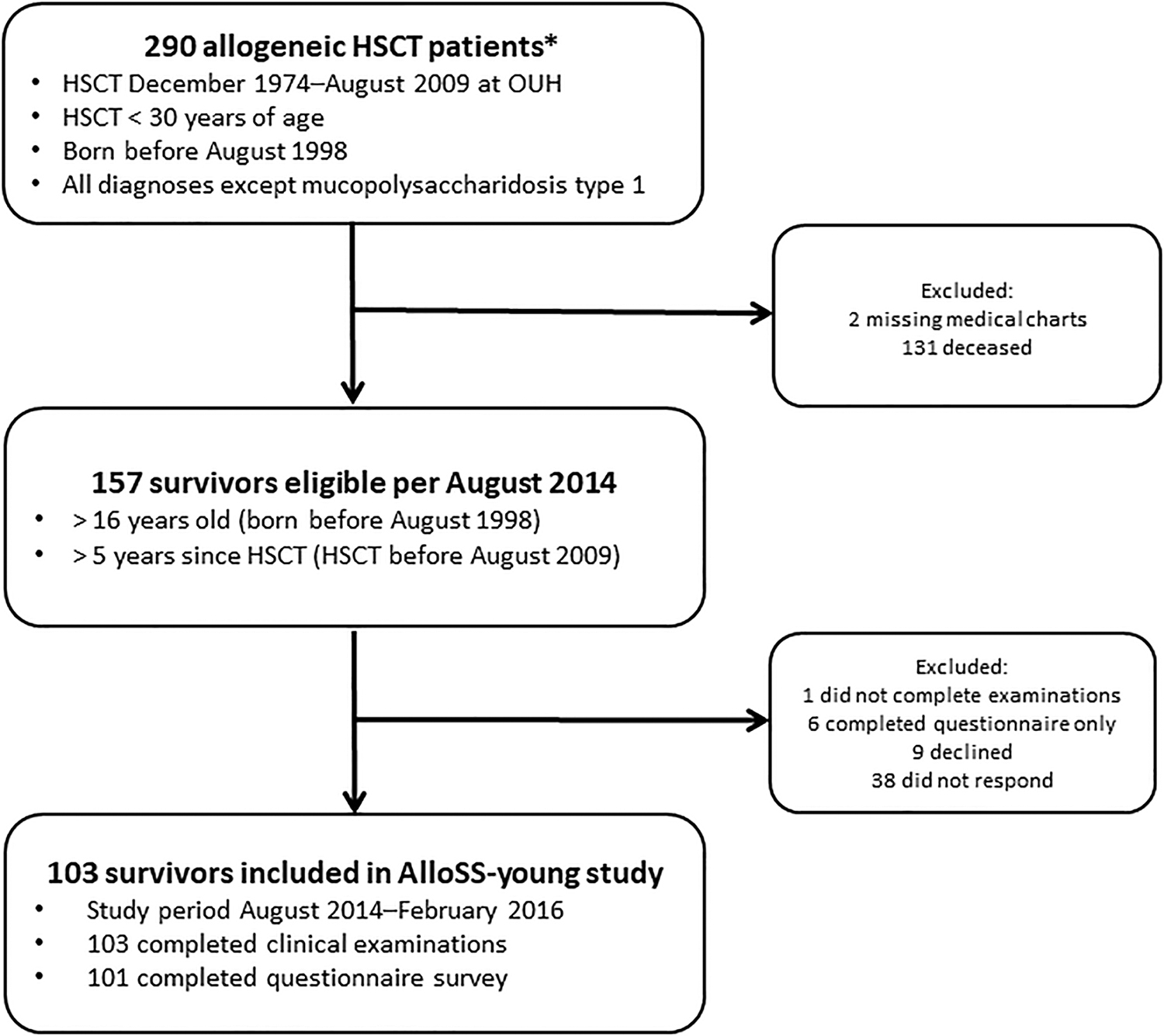
Flowchart of participants included in the cross-sectional study. *Identified through HSCT registries at OUH. HSCT, hematopoietic stem cell transplantation; OUH, Oslo University Hospital.
Procedures
Background information on all participants was obtained through chart review, including history of acute and chronic GVHD diagnosed by the Glucksberg and the Seattle criteria, respectively.16,26
All participants underwent standardized interviews and comprehensive multidisciplinary clinical, radiological, and laboratory assessments performed by a limited number of specialists. All organ examinations were standardized to capture the “diagnostic,” “distinctive,” “other,” and “common” features of cGVHD as defined by the 2014 NIH-criteria, 17 in addition to other late effects. Organ-specific severity was graded on a 0–3 scale, with 0 representing no involvement/no symptom and higher scores reflecting more severe impairment. Global severity was classified as mild, moderate, or severe based on the number and severity of the involved organs. Abnormalities due to non-cGVHD causes were excluded.
Patient-reported outcome measures
All participants were mailed a questionnaire covering sociodemographic and clinical status, as well as several PROMs.
We used the Lee Chronic GVHD Symptom Scale (LSS), a disease-specific instrument, to measure the symptom burden of cGVHD. The LSS contains seven subscales (skin, eye, mouth, lung, nutritional status, energy, and psychological functioning) and one summary score, range 0–100 (higher scores indicate greater symptom burden). A difference of 5–6 points on the summary score was considered clinically meaningful. 27
We assessed HRQOL using the Norwegian version of the generic instrument, the Short Form-36 (SF-36) version 1.28,29 The SF-36 includes eight subscales (physical functioning, role limitation due to physical problems, bodily pain, general health, vitality, social functioning, role limitation due to emotional problems, and mental health), range 0–100 (higher scores indicate better HRQOL). A five-point difference was considered clinically meaningful.29,30 (Detailed description of the PROMS is provided in Supplementary Data), Two survivors did not complete the LSS and SF-36 and were excluded from analyses that included these instruments (n = 101).
Norm data for HRQOL
We chose the 1996 Norwegian normative data for comparison rather than the more recent norm data from 2015.28,31 The surveys yielded similar results, but the response rates were lower in the 2015 survey, especially among the youngest age group (18–29 years). 31 Due to the young participants in our study, we considered the 1996 norm data as most suited. Only participants of the same age range as survivors were included from the norm population.
Statistical analyses
We compared participants and nonparticipants using chi-square statistics for categorical variables and Student's t-test (parametric) and Mann–Whitney U-test (nonparametric) for continuous variables.
To investigate risk factors associated with persistent active cGVHD, we performed univariable logistic regression models with active cGVHD (NIH global severity grade 1–3 vs. grade 0) as the dependent variable and patient and transplant characteristics (gender, age at diagnosis, primary diagnosis, donor type, donor-recipient gender mismatch, conditioning regimen, GVHD prophylaxis, and stem cell source) as explanatory variables. Explanatory variables with a p-value ≤0.1 in univariable models, gender, and age at HSCT were included in a multivariable logistic regression model.
Multivariable linear regression models adjusted for gender and age at the time of the study were used to examine the association between cGVHD global severity and the subscale scores of LSS and SF-36. We compared the HRQOL of survivors to that of the Norwegian population norms using multivariable linear regression models for each SF-36 subscale, adjusting for gender and age. We reported the marginal means and confidence intervals (95% CIs) from the multivariable regression models.
Two-tailed p-values <0.05 were considered statistically significant. All analyses were performed using Stata 15 (StataCorp, College Station, TX).
Results
Study population
Between August 2014 and February 2016, 103 allo-HSCT survivors (66% inclusion rate) were enrolled in the study (Table 1). The participants comprised 55 (53%) females, median age of 19.6 years [range 0.3–29.9] at transplant, at median 16.9 years [6.0–32.0] after HSCT, and 77 (75%) with underlying malignancy. Sibling donors were used in 65 (63%) cases and bone marrow was the stem cell source in 87 (84%) cases. A history of GVHD was found in 66 (64%) survivors.
Participant and Transplant Characteristics
Histiocytic lymphohistiocytosis, hyper-IgM, alpha-mannosidosis.
ATG® 2–3 mg/(kg·d) for 3 days or ATGAM® 30 mg/(kg·d) for 3 days.
Parents with 0–1 antigen mismatch on the not shared haplotype or HLA-identical uncles/aunts.
Information on 102 patients only.
ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; CML, chronic myeloid leukemia; GVHD, graft-versus-host disease; HLA, human leukocyte antigen; HSCT, hematopoietic stem cell transplantation; MDS, myelodysplastic syndrome; MMF, mycophenolate mofetil; Mtx, methotrexate; NHL, non-Hodgkin lymphoma; SAA, severe aplastic anemia; TBI, total body irradiation.
At the time of the study, 58 survivors (56%) had a full-time job. The majority of the survivors [67 (65%)] reported their health as good or very good (Table 2).
Participant Status at AlloSS-Young Cross-Sectional Study
aGVHD, acute graft-versus-host disease; cGVHD, chronic graft-versus-host disease; GI, gastrointestinal; NIH, National Institutes of Health.
Compared to the 54 (34%) nonparticipants (Fig. 1), the 103 (66%) participants were more likely to be female (53% vs. 31%, p = 0.009), older both at time of HSCT (mean difference [MD] 3.3 years, p = 0.013) and at enrollment (MD 6.9 years, p < 0.001), and they also had longer follow-up from HSCT (MD 3.6 years, p < 0.001). There was no difference regarding the underlying diagnosis (malignant vs. nonmalignant, p = 0.123; Supplementary Table S1).
Chronic graft-versus-host disease
Overall, 32 (31%) survivors were diagnosed with active cGVHD by the 2014 NIH-criteria (Table 2). The global severity was mild in 13 (41%), moderate in 8 (25%), and severe in 11 (34%) survivors. The median number of organs involved were two (range 1–6), and the most frequently involved organs were eyes [18 (17%)] and mouth [13 (13%)] (Table 2). Two survivors (2%) were on systemic immunosuppressive therapy due to cGVHD at the time of enrollment. None of the survivors was diagnosed with late-onset acute GVHD (aGVHD).
The history of cGVHD (diagnosed by the Seattle criteria) at the time of enrollment was identified through chart review (Table 2). Among those diagnosed with active cGVHD according to the NIH-criteria, 12 (38%) survivors had chart information of historically defined active cGVHD, 12 (38%) survivors had resolved cGVHD, 6 (18%) survivors had resolved aGVHD, but no history of cGVHD, and 2 (6%) survivors had no history of aGVHD or cGVHD. Of the 71 (69%) survivors without active cGVHD according to the NIH-criteria, 38 (54%) had resolved cGVHD and 33 (46%) had no history of cGVHD.
In multivariable analyses, two factors were associated with active cGVHD (Table 3). The probability of persistent active cGVHD was increased with prior acute GVHD grade II–IV [odds ratio (OR) 4.15, 95% CI: 1.22–14.09, p = 0.022] and reduced with in vivo T cell depletion (OR 0.07, 95% CI: 0.01–0.87, p = 0.040). Gender, age at diagnosis, primary diagnosis, donor type, donor-recipient gender mismatch, conditioning regimens, GVHD prophylaxis, and stem cell source were not associated with cGVHD in long-term survivors.
Factors Associated with Chronic Graft-Versus-Host Disease by the National Institutes of Health-Criteria (Global Severity Grade 1–3)
Bold values indicate p < 0.05.
Male donor-female recipient and same sex donor-recipient.
ATG® or ATGAM®.
CI, confidence interval; CyA, cyclosporine A; MA, myeloablative; Mtx, methotrexate; OR, odds ratio; TBI, total body irradiation.
Patient-reported outcome measures
Figures 2 and 3 present the LSS subscales and summary scores and SF-36 subscale scores, respectively, by cGVHD global severity grade (adjusted for gender and age). We found an association between increasing global severity and higher LSS subscale scores for the subscales eyes (p < 0.001), mouth (p = 0.037), nutritional status (p < 0.001), and summary score (p < 0.001). This reflects a higher symptom burden in these subscales with more severe active cGVHD (Fig. 2). The difference was clinically meaningful for the LSS summary score with a higher score of 13 points (indicating a higher symptom burden) in those with severe compared to those with no active cGVHD.
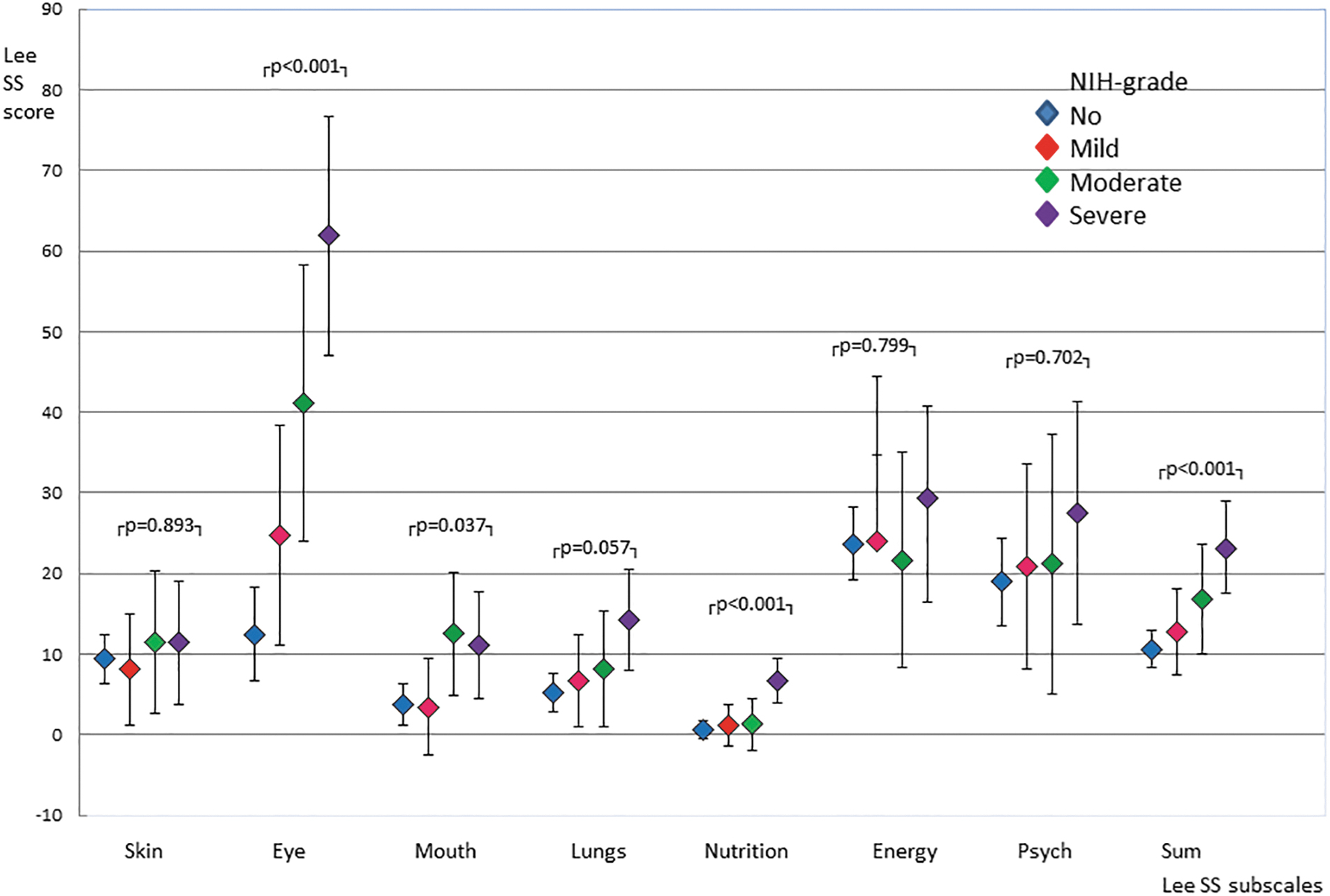
Lee cGVHD symptom scale subscales and summary score by cGVHD global severity grade (n = 101). The figure shows means with 95% confidence intervals from multivariable regression analyses adjusted for age and gender. cGVHD, chronic graft-versus-host disease; NIH, National Institutes of Health; Psych, psychology.
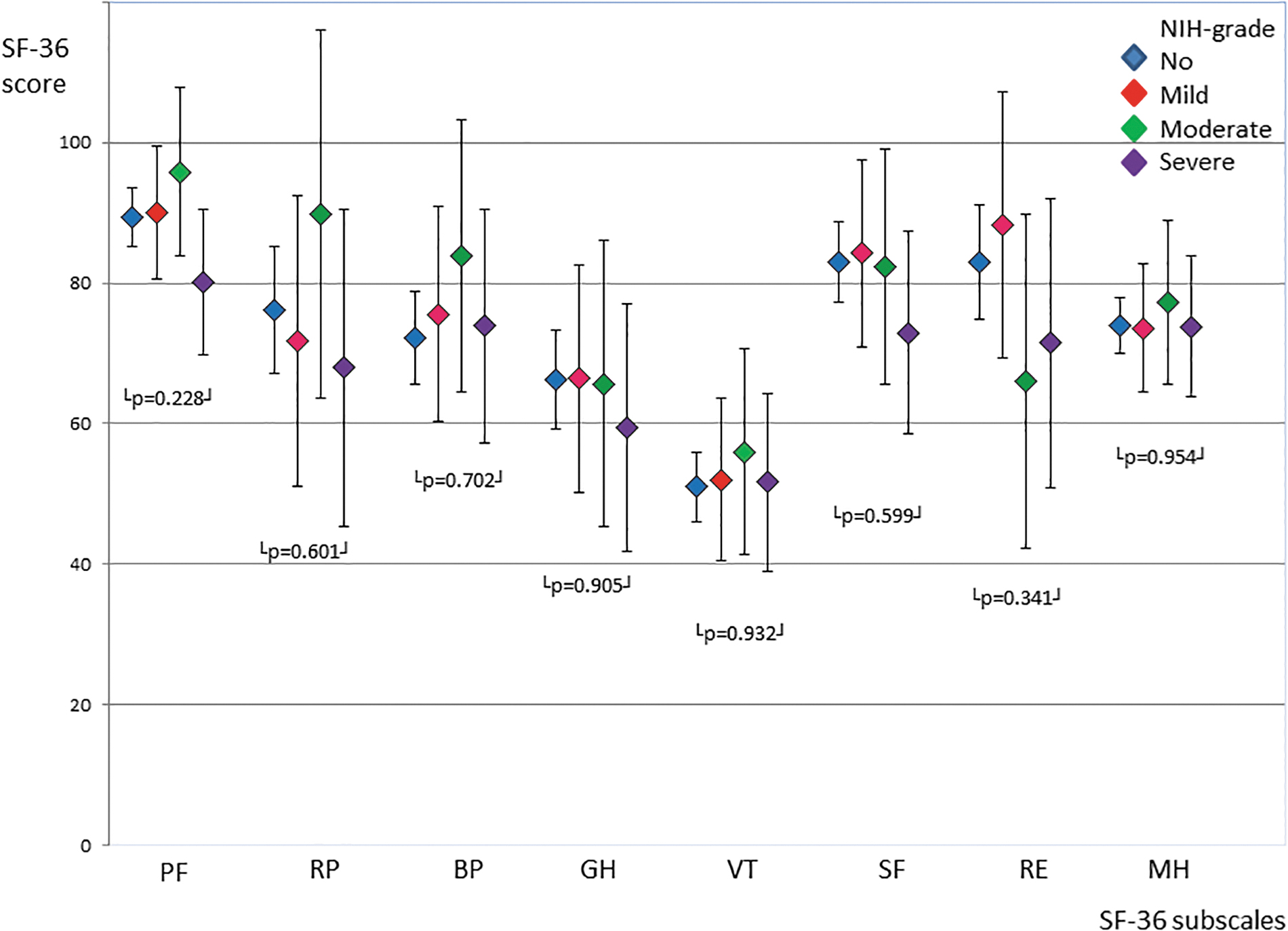
SF-36 subscale scores by cGVHD global severity grade (n = 101). The figure shows means with 95% confidence intervals from multivariable regression analyses adjusted for age and gender. BP, bodily pain; GH, general health; MH, mental health; PF, physical functioning; RE, role limitations due to emotional problems; RP, role limitation due to physical problems; SF-36, Short Form-36; SF, social functioning; VT, vitality.
The survivors with severe active cGVHD reported lower scores in several SF-36 subscales. In contrast to those with no cGVHD, survivors with severe active cGVHD had lower scores in several subscales. The difference was 9 points in physical functioning, 8 points in role limitations due to physical problems, 7 points in general health, 10 points in social functioning, and 11 points in role limitation due to emotional problems. The differences were clinically meaningful, indicating reduced HRQOL in survivors with severe compared to those with no active cGVHD, but the associations were not statistically significant (Fig. 3).
Compared to the Norwegian population norms, the survivors scored significantly lower in all SF-36 subscales, except for bodily pain (p = 0.072) and role limitations due to emotional problems (p = 0.355) (Supplementary Table S2). The differences were clinically meaningful in the subscale role limitations due to physical problems (mean score 75.2 [AlloSS-participants] vs. 91.5 [Norwegian norms], p = 0.004), general health (64.9 vs. 79.9, p < 0.001), and vitality (52 vs. 60.5, p < 0.001). Although not clinically meaningful, the survivors had significantly lower scores in physical functioning (88.4 vs. 91.5, p = 0.031), social functioning (82.0 vs. 86.6, p = 0.035), and mental health (74.4 vs. 78.6, p = 0.012).
Discussion
This study on cGVHD and HRQOL in a national cohort of long-term survivors of CAYA allo-HSCT demonstrates that, at a median of 17 years after transplant, one-third of the patient cohort was diagnosed with active cGVHD by the 2014 NIH-criteria. To the best of our knowledge, few other studies have assessed active cGVHD in long-term survivors of CAYA allo-HSCT using the 2014 NIH-criteria. In our study, the proportion with mild disease was higher compared to two previous studies on cGVHD using the 2005 NIH-criteria in pediatric HSCT survivors.13,32
In the study by Cuvelier at al. 32 with 12 months of follow-up, the reported incidence of cGVHD was 21%. The global severity was mild, moderate, and severe in 15%, 37%, and 49%, respectively. We investigated HSCT survivors at a median of 17 years post-HSCT. It is possible that the survivors were beyond their peak severity of cGVHD as the condition usually resolves within 5–7 years.13,33,34 Inagaki et al. 13 also reported a higher incidence of severe cGVHD in pediatric HSCT recipients who were retrospectively diagnosed with cGVHD using the 2005 NIH-criteria.
This study included exclusively patients with active cGVHD, which might reflect a more severely affected population. Although the NIH-criteria did not change much between 2005 and 2014,14,17 a study comparing the two versions showed that the 2014 NIH-criteria resulted in a downgrading of global severity. 22 The downgrading was primarily caused by changes in the NIH lung and liver criteria. This could explain the observed differences in global severity scoring since we used the 2014 NIH-criteria and not the 2005 NIH-criteria used by Inagaki et al. and Cuvelier et al.13,32
Organs commonly affected in studies using the NIH-criteria have been skin, mouth, and eyes followed by lungs and liver.13,32,35–37 In our study, frequently involved organs were eyes, mouth, lungs, genitals, and skin, in descending order. All participants were examined by an ophthalmologist, and all female participants were examined by a gynecologist. This can explain why we observed a higher occurrence of ocular and genital cGVHD compared to other studies that did not include these examinations.35–38 We did not observe any case of liver cGVHD. This could be due to the revision of the NIH-criteria in 2014.
The new criteria included reduced cutoff levels for liver enzyme values and removal of aspartate aminotransferase from the scoring system.15,17,39 These changes have been reported to cause a shift in the organ-specific severity for liver resulting in fewer cases of moderate or severe liver cGVHD and more cases of no or mild organ involvement. 22
In multivariable analyses, the probability of persistent active cGVHD was increased with prior aGVHD grade II–IV and reduced with in vivo T cell depletion. Our findings are in accordance with the most consistent risk factors for historically defined cGVHD22,34,35,40 and NIH cGVHD32,35,36 in studies on children and adults. There was no association between persisting active cGVHD and other reported risk factors such as older patient/donor age, gender disparity (female donor to male recipient), peripheral blood as stem cell source, human leukocyte antigen mismatch or unrelated donors, conditioning regimens, including total body irradiation, or underlying malignancy.32,35,40–42
This could be due to differences in study population, transplantation protocols, and length of follow-up post-HSCT. The risk factors for developing cGVHD in the early post-transplant course as evaluated in these studies may also differ from those associated with persisting cGVHD as in our study. Nevertheless, we do recognize that the size and heterogeneity of our cohort could affect the power to identify possible significant associations.
PROMs have become an important tool in clinical trials as they mirror the patients' perception of their health. 43 As recommended by the NIH-criteria, we included both a disease-specific instrument (LSS) and a generic instrument (SF-36). As expected, survivors with more severe active cGVHD reported higher scores on several LSS subscales and summary scale. The association was both statistically significant and clinically meaningful (>5–6 points difference), and particularly evident for the eye subscale. These findings are in line with previous studies. 44,45,36,,46
To our knowledge, there are no published studies on the impact of cGVHD by the NIH-criteria on HRQOL in very long-term survivors of CAYA-HSCT. 47
Studies on adults have shown that the severity of cGVHD is negatively associated with HRQOL.6,48 Contradictory to these results, we did not find significant associations between the severity of cGVHD and HRQOL. There could be several reasons for this discrepancy. First, only two of the survivors were on systemic immunosuppressive therapy at study entry. Inamoto et al. 49 have shown that daily treatment with prednisolone was associated with adverse HRQOL as measured by the SF-36. The effect of systemic immunosuppression could be additive to the effect of severe cGVHD on HRQOL. Second, studies investigating the effect of organ involvement on HRQOL have reported that severe cGVHD in skin, gastrointestinal tract, lungs, joint, and fascia are negatively associated with the SF-36 component scores.7,36
In a study of adults at a median of 7 years after allo-HSCT, Kurosawa et al. reported that mild cGVHD in the lungs, gastrointestinal (GI) tract, and joints and fascia were associated with cGVHD severity. 48 In our study, the only organs with severe cGVHD were the lungs, eyes, and genitals, and only three survivors were diagnosed with cGVHD in the GI tract or joints and fascia. Furthermore, our cohort of long-term survivors of CAYA allo-HSCT might not be comparable to adult HSCT recipients evaluated by Kurosawa et al., at an earlier time point post-HSCT. 48 Third, the lack of association could be due to a response shift, 50 a phenomenon in which the survivors with time adapt to a chronic disease or a life-threatening situation by changing their internal standards and values, and thereby the conceptualization of HRQOL.
Compared to the Norwegian population norms, HSCT survivors reported significantly lower HRQOL on nearly all SF-36 subscales. These findings are similar to the results from the few published studies on HRQOL after childhood HSCT. In these studies, HSCT childhood cancer survivors (mean 5–17 years from cancer diagnosis) had impaired HRQOL compared to population norms.39,51–53
While earlier studies have noted an improvement in HRQOL 12–24 months post-transplant, 54 a more recent study showed that more time elapsed after HSCT was associated with reduced HRQOL. 53 This advocates for long-term follow-up of CAYA allo-HSCT recipients as it might take many years to recognize the impact of late effects on HRQOL.
The main strengths of this study are the nationwide inclusion of allo-HSCT survivors, long follow-up, and the combination of systematic multidisciplinary clinical examination and PROMs. We recognize that the study is limited by the nature of the cross-sectional design and the heterogeneity of transplant-related factors that might have reduced the possibility to identify significant associations. We cannot rule out that a nonresponse bias might have affected the results. However, Lie et al. 55 reported that despite a modest response rate of nearly 40% in a nationwide study of young cancer survivors, there was little evidence for a response bias. Thus, we consider an attendance-rate of 66% to be very satisfactory in a population-based long-term follow-up study.
In conclusion, our study shows that at a median of 17 years after CAYA allo-HSCT, one third of the survivors were diagnosed with active cGVHD by the 2014 NIH-criteria. This correlated with the reported symptom burden of cGVHD. We did not find an association between the severity of cGVHD and HRQOL. However, as a group, the survivors reported significantly lower HRQOL compared to population norms. Prospective longitudinal studies combining clinical data and PROMs are needed to better recognize the risk factors and improve surveillance after CAYA allo-HSCT.
Footnotes
Acknowledgment
The authors would like to thank Elna Hamilton Larsen and Karin Sylte Hammeren, the research nurses who facilitated the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was partially financed by the Norwegian Extra Foundation for Health and Rehabilitation project no. 2013.2.230 and the South-Eastern Norway Regional Health Authority grant no. 2015084. The funding organizations had no role in the design or conduct of this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.