
Abstract
Purpose:
The demand for fertility preservation continues to grow as cancer treatment outcomes improve. The specimen storage period is longer for fertility preservation than for conventional fertility treatment; therefore, a robust management system for stored specimens is required. We conducted the first national survey in Japan on the management of cryopreserved specimens in fertility preservation facilities.
Methods:
Questionnaires were mailed to 130 fertility preservation facilities. Primary outcomes included the official position of the storage manager, support system in case of facility closure, disaster countermeasures, management and operating system for liquid nitrogen storage containers, preservation costs, and method to confirm the intention to continue storage.
Results:
The response rate was 63.8%. The facility director most commonly functioned as the storage manager (59.0%). In case of facility closure, 20.5% had an approved transfer site; 59.0% had not made any decisions. In the management of liquid nitrogen containers, 83.1% regularly replenished the liquid nitrogen, 65.1% regularly checked the amount, and 16.9% had alarm monitoring systems. Regarding disaster countermeasures, 70.9% had taken measures to protect specimens.
Conclusion:
This survey revealed issues such as disparities among facilities regarding long-term specimen storage systems. Accordingly, management standards for fertility preservation facilities should be established.
Introduction
The survival rate of childhood, adolescents, and young adults (CAYA) with cancer is over 80% due to recent improvements in cancer treatment outcomes.1,2 However, radiation therapy and some chemotherapies may cause gonadal dysfunction, and patients who do not undergo fertility preservation may be infertile in the future. Therefore, CAYA with cancer may cryopreserve sperm, oocytes, embryos, or ovaries before undergoing cancer treatments that cause infertility. 3
Cryopreservation is an essential technique for preserving fertility. Ovarian tissue cryopreservation has been widely practiced in Japan since the first live birth obtained by frozen-thawed ovarian tissue transplantation reported in 2004. 4 Oocyte cryopreservation and embryo cryopreservation have become easier with the widespread use of the vitrification method,5–9 and the survival rate after freezing and thawing has increased to >90%.7–10 Ovarian tissue cryopreservation performed overseas often uses the slow freezing method,11,12 which is the standard method. In recent years, the vitrification method has been reported for ovarian tissue cryopreservation, and it has been adopted in some facilities.13–15 As of 2016, 96.0% of Japanese facilities have performed ovarian tissue cryopreservation using the vitrification method. 16
Cryopreserved fertility preservation specimens are not used until the patient wishes to have a child, after the cancer treatment is completed. Therefore, specimens are often stored for prolonged periods. Especially, as ovarian tissue cryopreservation is applicable to pediatric cancers, it is not uncommon for ovarian tissue to be stored for several decades, until the patient becomes an adult, gets married, and wishes to have a child. 17 The European Society for Reproductive Medicine (ESHRE) and American Society for Reproductive Medicine (ASRM) have provided guidelines for specimen storage systems;18–20 however, the Japan Society for Reproductive Medicine and Japan Society of Obstetrics and Gynecology (JSOG) have not yet provided detailed guidelines.
Fertility preservation for cancer patients has begun in various institutions; however, most of these institutions may have envisioned the short-term preservation of gametes and/or zygotes for infertile patients, and whether these institutions have adopted adequate systems for long-term preservation is unknown. Moreover, the management and storage systems for fertility preservation specimens in Japan have not yet been investigated.
Therefore, we conducted a survey on the current status of management and storage systems of cryopreserved specimens for oncofertility in fertility preservation facilities in Japan.
Materials and Methods
Ethical considerations
This study was approved by the Ethics Committee of the Mie University School of Medicine (Approval No. H2020-183).
Data collection
In Japan, it is necessary to apply to the JSOG for approval to perform fertility preservation in patients with cancer. In December 2020, we sent a questionnaire to 130 facilities approved by the JSOG as fertility preservation facilities for oncofertility (as of October 2020). The response deadline was March 2021.
The questionnaire comprised 36 items, and the primary outcomes were the official position of the storage manager at the facility, support system in case of facility closure, disaster countermeasures, management and operating systems for liquid nitrogen storage containers, storage costs, and method used to ensure continued storage. Answered items were adopted as data. For items that allowed multiple responses, the percentages of respondents that selected each option in that item among all respondents were calculated.
Results
Survey response rate
The response rate was 63.8% (83/130). The facilities that responded comprised university hospitals (38.6%, 32/83), general hospitals (21.7%, 18/83), and private clinics (39.8%, 33/83). The response rate to the survey by facility was 71.1% (32/45) for university hospitals, 54.5% (18/33) for general hospitals, and 63.5% (33/52) for private clinics.
Official position of the storage manager at the facility
The official position of the storage manager was the facility director in 59.0% (49/83) of facilities, the departmental head of Obstetrics and Gynecology in 24.1% (20/83), the manager of a Center for Reproductive Medicine in 18.1% (15/83), and the departmental heads of both Obstetrics and Gynecology and Urology were co-responsible in 1.2% (1/83) (Fig. 1). Of the facilities with a facility director as the responsible person, 26.5% (13/49), 8.2% (4/49), and 65.3% (32/49) were in university hospitals, general hospitals, and clinics, respectively (Fig. 1).
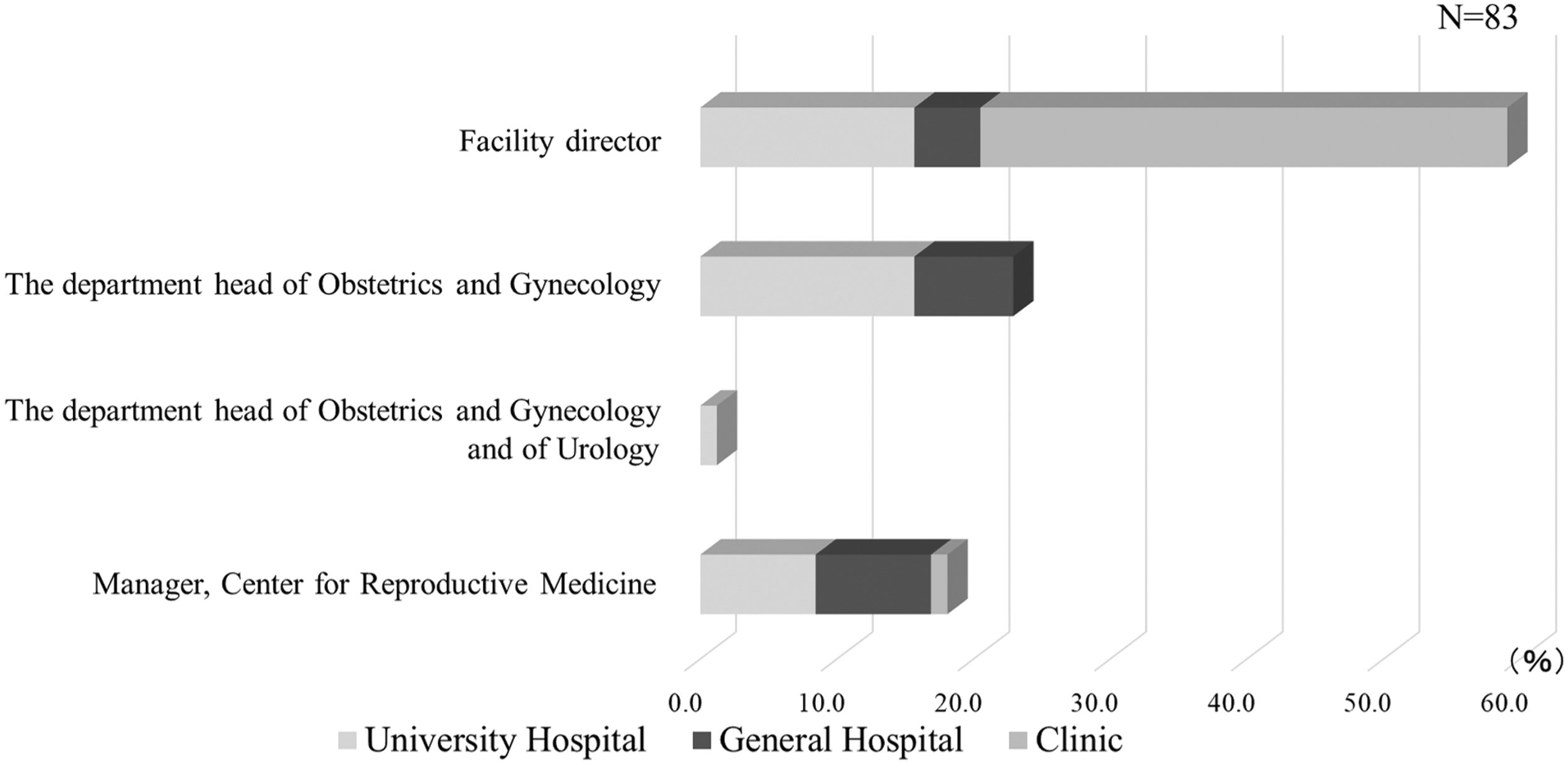
Storage manager. The person responsible for the storage of fertility preservation specimens is often the facility director.
Of the facilities with the departmental head of Obstetrics and Gynecology as the responsible person, 68.4% (13/19) and 31.6% (6/19) were in university and general hospitals, respectively (Fig. 1). Of the facilities with the manager of a Center of Reproductive Medicine as the responsible person, 46.7% (7/15), 46.7% (7/15), and 6.7% (1/15) were in university hospitals, general hospitals, and clinics, respectively (Fig. 1). The facility with the departmental heads of both Obstetrics and Gynecology and Urology as jointly responsible was in a general hospital (Fig. 1).
Support system in case of facility closure
A total of 20.5% (17/83) of the facilities had established a transport destination, should the facility be closed, and 59.0% (49/83) had not made any decisions (Fig. 2). The remaining 20.5% (17/83) indicated that the specimens would be transferred, but did not yet have approval from the intended recipient public hospital (Fig. 2). Of the facilities with a pre-established support system, 5.9% (1/17), 11.8% (2/17), and 82.4% (14/17) were in university hospitals, general hospitals, and clinics, respectively (Fig. 2). Of the facilities that had not made any decision, 59.2% (29/49), 18.4% (9/49), and 22.4% (11/49) were in university hospitals, general hospitals, and clinics, respectively (Fig. 2). Among the facilities indicating that the specimens would be transferred to a public hospital, but did not yet have approval, 17.6% (3/17), 35.3% (6/17), and 47.1% (8/17) were in university hospitals, general hospitals, and clinics, respectively (Fig. 2).
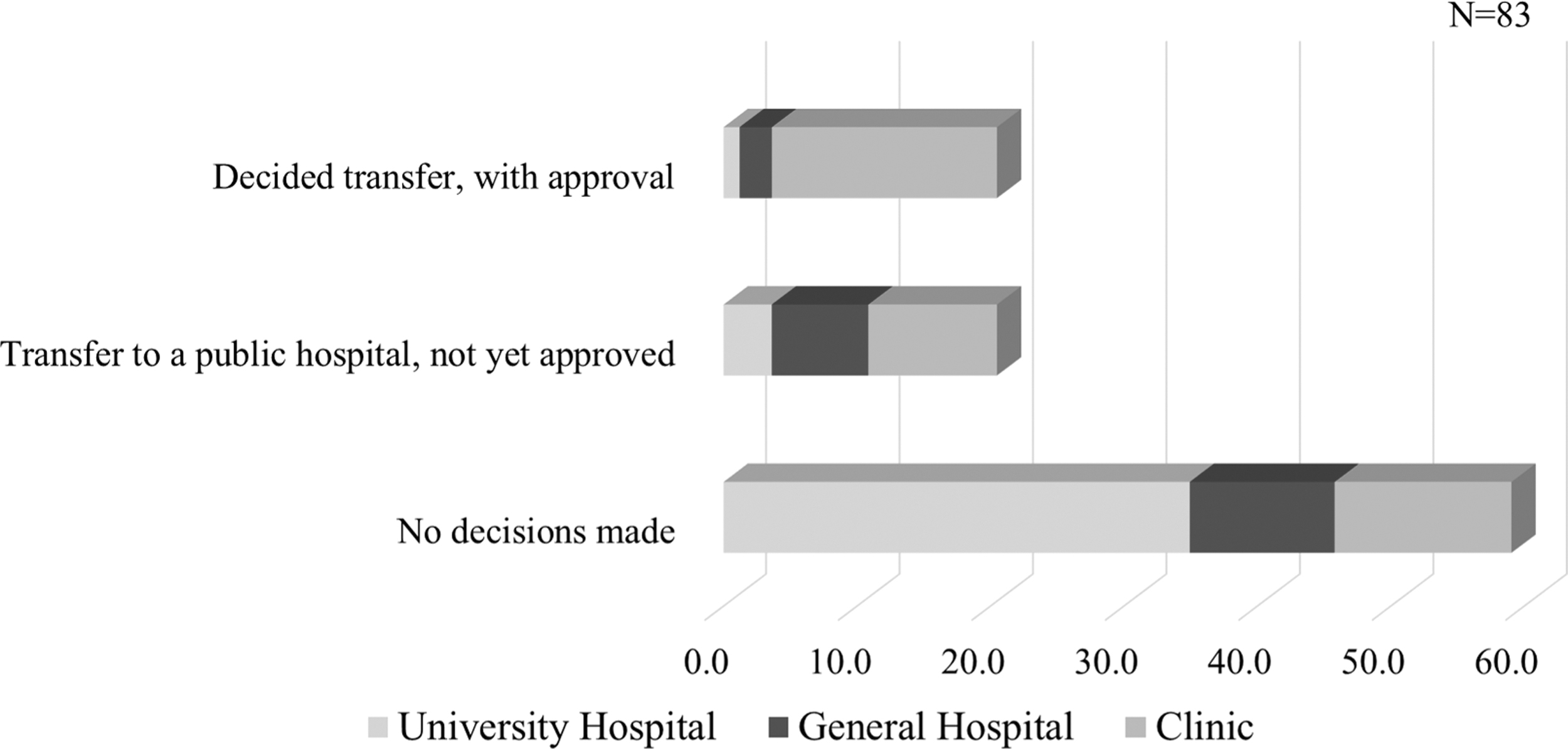
Measures to be taken in case of facility closure. In total, 20% of the facilities established measures to be taken in the event that it became difficult to maintain the storage system due to facility closure, and most of these facilities were clinics. University hospitals accounted for the largest percentage (59.2%) of facilities that had not made any decision.
Management and operating system for liquid nitrogen storage containers
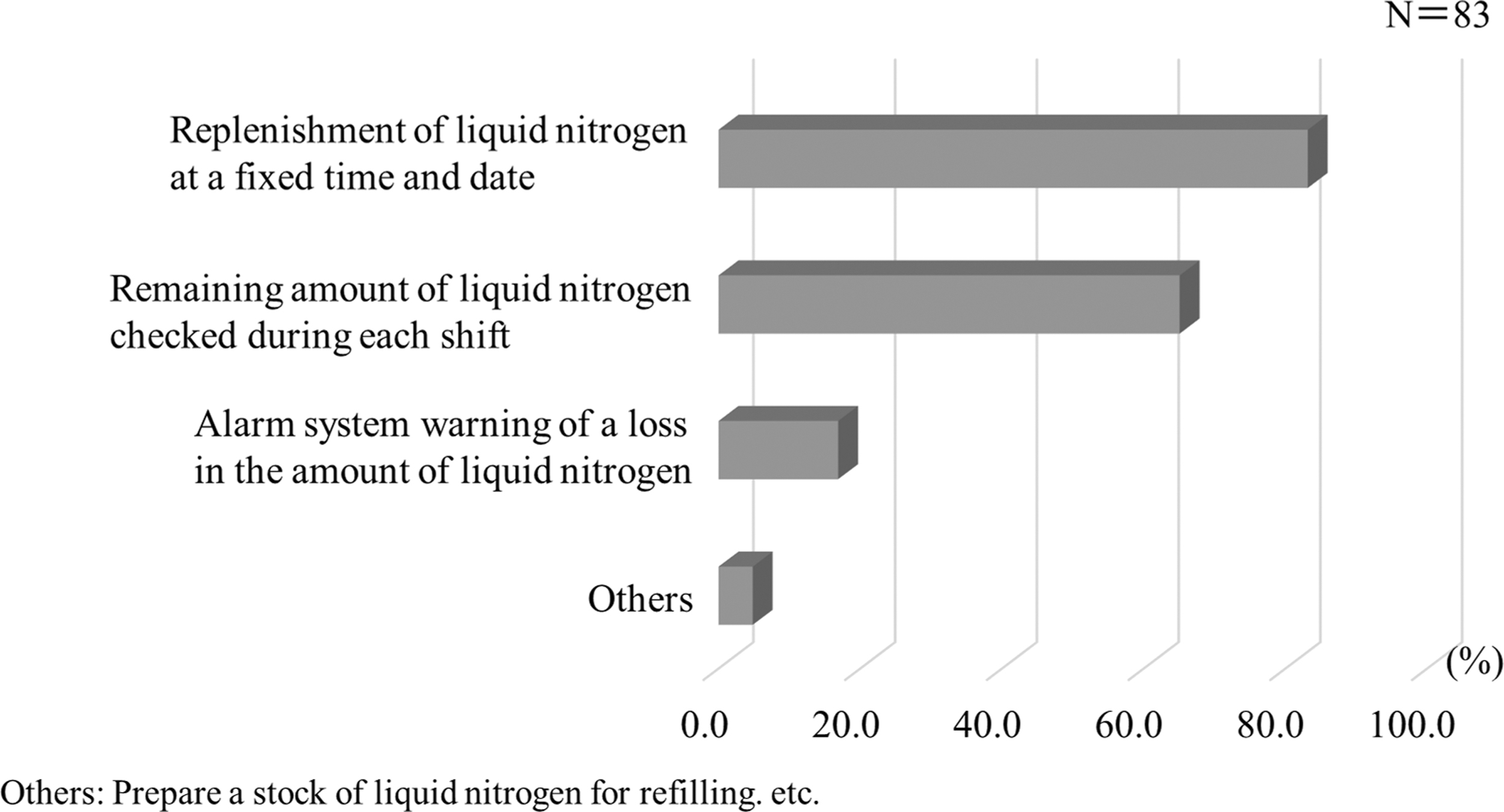
In total, 83.1% (69/83) of facilities regularly replenished the liquid nitrogen, 65.1% (54/83) regularly checked the remaining amount of liquid nitrogen directly, and 16.9% (14/83) used an alarm monitoring system. Other responses were provided in 4.8% (4/83) of facilities, including one facility that maintained a spare storage container filled with liquid nitrogen (Fig. 3).

Innovations in the management of liquid nitrogen. In total, 16.9% of the facilities had alarms to warn of low liquid nitrogen levels.
Disaster countermeasures
Of the facilities, 70.9% (56/81) had taken disaster countermeasures, whereas 31.6% (25/81) had not (Fig. 4). Respondents were asked to freely describe the measures taken. Most responses were general, such as “tying tanks with bands to prevent them from tipping over,” “installing seismic isolation platforms,” “attaching casters to tanks,” and “placing cushions between tanks.” More specific responses included an “automatic liquid nitrogen replenishment system,” “automatic detection system of the remaining amount of liquid nitrogen that notifies the cell phone of the person in charge,” and “contract for priority delivery of liquid nitrogen in case of disaster.”
Decision taken on measures to protect cryopreservation specimens against disasters. Even among facilities that responded that they were taking such measures, most were general in nature.
Preservation costs (oocyte/embryo cryopreservation and renewal cost comparisons)
Cryopreservation is more expensive for embryos than for oocytes in most facilities because fertilization and culturing of fertilized embryos are required. However, there was no difference in renewal costs between oocytes and embryos (Fig. 5).
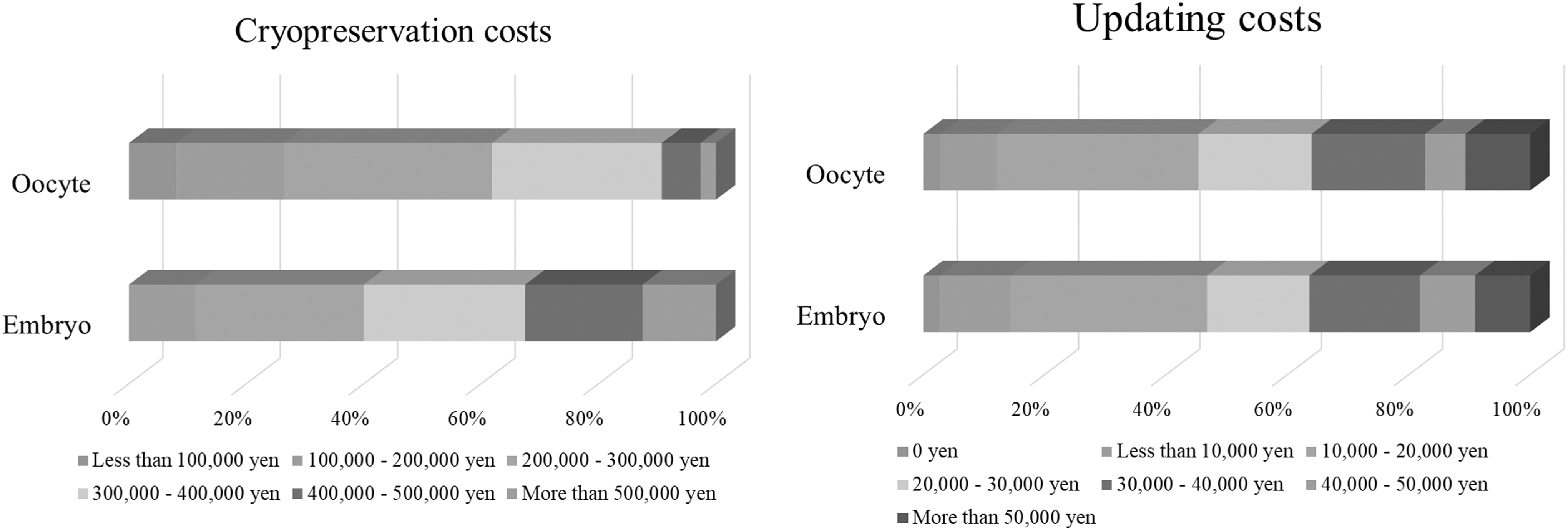
Comparisons in cryopreservation and updating costs between embryos and oocytes.
Confirmation of the intention to continue storage (person in charge of renewal and the method and frequency of confirmation)
Doctors, embryologists, and clerical staff confirmed the patient's intention to renew in 61.4% (51/83), 42.2% (35/83), and 19.3% (16/83) of facilities, respectively. Confirmation was performed in an in-person consultation with a doctor and by mail in 62.7% (52/83) and 48.2% (40/83) of facilities, respectively. In total, 80.7% (67/83) of facilities indicated that the renewal interval was once a year (Fig. 6).

Type, method, and frequency of confirming the patient's intention to renew cryopreservation. Confirmation at the time of renewal is most often performed in person with a doctor. The most common renewal interval was once per year.
Collaboration between reproductive specialists and oncologists at the time of renewal
In total, 54.2% (45/83) of facilities collaborated with an oncologist at the time of renewal. The collaboration mostly involved obtaining information from the patients in 60.0% (27/45) of facilities, followed by communications in writing in 37.8% (17/45) and by telephone in 33.3% (15/45) (Fig. 7).

Collaboration between reproductive specialists and oncologists at the time of renewal. About half of the respondents collaborate with oncologists at the time of renewal.
Countermeasures against renewal expiration, patient death, and loss of patient tracking
As measures against an inability to contact the patient at the time of renewal, 68.7% (57/83) of the facilities reminded the patient of the renewal by phone, and 45.8% (38/83) reminded the patient by mail. In addition, 42.2% (35/83) of facilities reported that they would continue to keep the specimens frozen if they could not contact the patient, whereas 12.0% (10/83) unconditionally destroyed the specimens if they could not contact the patient within a certain period of time. In 24.1% (20/83) of facilities, the oncologist of the primary disease was contacted to confirm survival (Fig. 8).
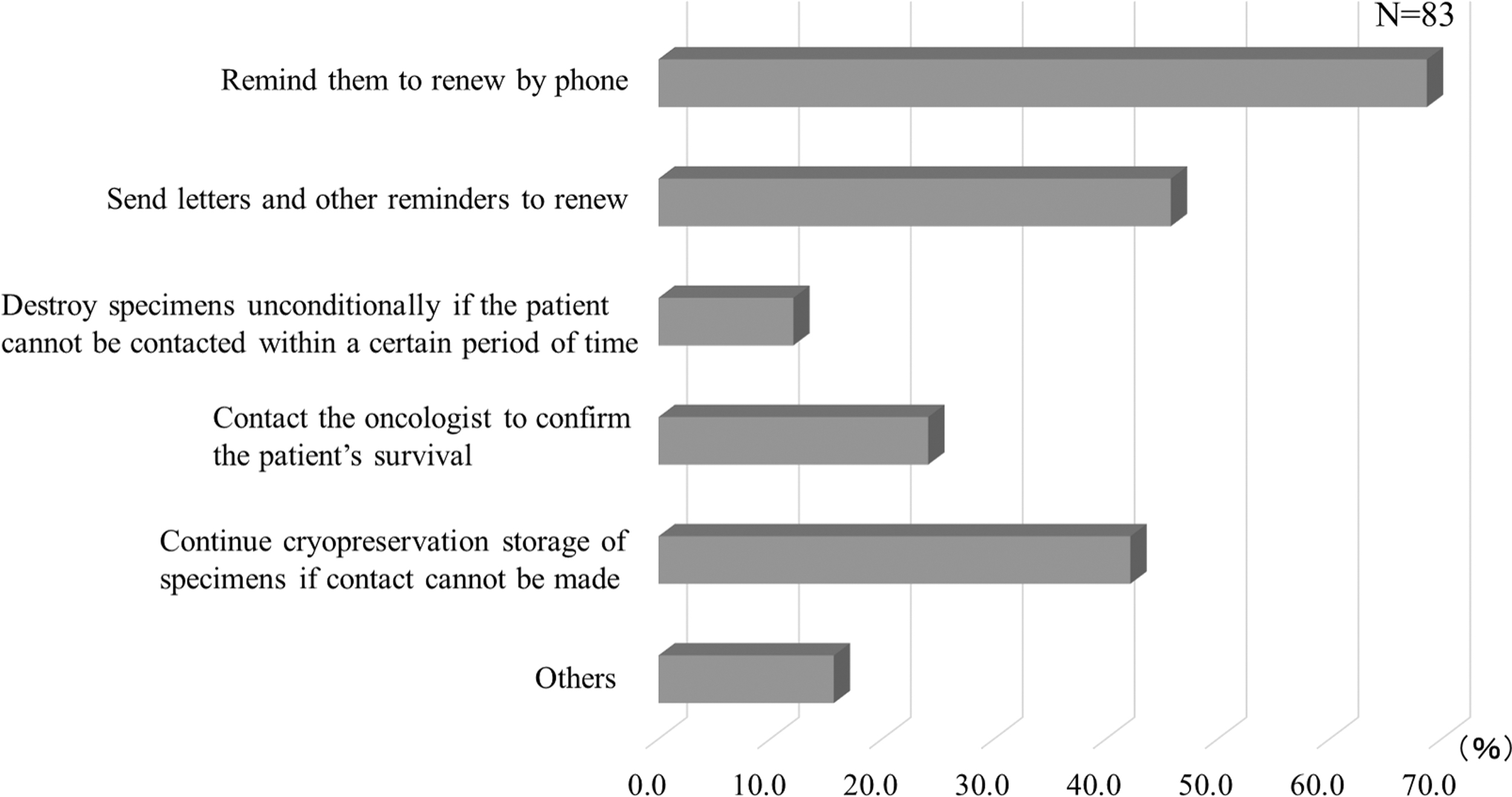
Countermeasures against forgetting to renew, death, and loss of communication. In total, 42.1% of facilities extend the storage period if a patient cannot be contacted.
Discussion
Improvement in treatment outcomes for CAYA patients with cancer and recent advances in vitro fertilization technology have increased the selection of fertility preservation before cancer treatment. Specimens of patients with cancer are stored for longer periods of time than specimens of typical patients with infertility, and for pediatric patients, they are stored for decades. In Japan, public subsidies have been provided by the government to patients who undergo fertility preservation since April 2021. Accordingly, strict continuity and stability of the storage and management system are required. Therefore, we investigated the current status of storage systems for fertility preservation specimens.
The official position of the storage manager was the facility director in most facilities, including most private clinics. However, the departmental head of Obstetrics and Gynecology was the most common storage manager in university hospitals and was frequently the storage manager in general hospitals (Fig. 1). Thus, the responsible person at Japanese clinics is often clearly defined as a facility director; in contrast, at hospitals, the hospital director was also responsible for the implementation of fertility preservation, indicating that responsibility is unclear in these institutions.
Approximately 20% of respondents had decided on measures to be taken in case it became difficult to continue cryopreservation storage at their facility, and the majority of these were clinics. Since clinics are often run by a small number of doctors, they may consider situations in which the clinic is closed due to retirement, accident, or sudden death of the facility director.
Approximately 60% of facilities indicated that they had not made any decisions regarding such measures; about 20% of these were clinics and the remainder were university or general hospitals. These clinics need to be encouraged to be prepared to respond to unforeseen circumstances. As university and general hospitals are considered to be the last resort for specimen storage facilities, they may not take any such measures. Therefore, university and general hospitals need to establish stricter long-term storage systems (Fig. 2). In European countries, university and public hospitals are taking the lead in centralizing the cryopreservation of fertility preservation specimens, which are stored at centers immediately after collection. 21
The management of liquid nitrogen storage containers is the most critical issue in specimen management. Dozens to hundreds of specimens are stored in a single liquid nitrogen storage container; hence, damage to a single tank can deprive the future fertility of many patients. To maintain the appropriate amount of liquid nitrogen, it is crucial to replenish and periodically check the remaining amount. In this survey, ∼80% of facilities regularly replenished liquid nitrogen reserves, whereas ∼60% regularly checked the remaining amount of liquid nitrogen directly (Fig. 3); as these percentages do not match, some facilities may not be able to adequately manage liquid nitrogen within normal operations. However, even with regular replenishment and management of liquid nitrogen, damage remains possible due to tank deterioration.
If an accident occurs during a holiday or at night, the response may be delayed. If the vacuum in the space between the inside and outside of the tank is lost because of tank damage, the lower internal temperature cannot be maintained, and the liquid nitrogen evaporates rapidly. 22 If the damage is minimal, there is a grace period of a few hours between the occurrence of the accident and depletion of liquid nitrogen, and a serious accident can be avoided by a timely response.
However, if the discovery is delayed, the accident can lead to an irreversible situation. There are several types of alarm systems, including those that detect a drop in tank temperature, a loss of liquid nitrogen by a change in the weight of the tank, changes in the amount of liquid nitrogen by the height of the liquid surface, and temperature changes on the tank surface. In this survey, only 15% of facilities had warning systems with alarms (Fig. 3). Only one facility stored an extra tank containing liquid nitrogen as a response to emergencies. The preparation of an extra tank is crucial because if a tank is damaged, the specimens must be immediately transferred to another tank.
We found a significant difference in emergency preparedness between facilities. Although tanks may be damaged by a disaster or accident, only 70% of the facilities had taken measures against disasters. Most of these were general measures, such as installing casters on the tanks, securing tanks with bands, and installing seismic isolators; few facilities took special measures for long-term specimen storage (Fig. 4). Overseas, many specimens were lost as a result of several incidents involving specimen storage containers in 2018.23–25 In one case, human error was involved, as an alarm indicating an abnormality in the remaining amount of liquid nitrogen had been switched off, and the depletion of liquid nitrogen was noticed too late. 23
Furthermore, there are problems with the daily management system of the tanks and their service life. 26 Therefore, in addition to the installation of alarms for the remaining amount of liquid nitrogen, a management system should be established. The ESHRE and ASRM provide guidelines18–20 for the implementation of reproductive medicine, which refer to details such as staffing, necessary competencies of the personnel, management standards for culture rooms, management of liquid nitrogen tanks, and installation of alarms and backup power supplies. However, the Institutional Standards of the Japan Society for Reproductive Medicine 27 state only that “the implementing facility shall not only establish safe and reliable storage facilities and management systems for the cryopreservation of unfertilized oocytes and ovarian tissue, but shall also store detailed records of the client and frozen unfertilized oocytes and ovarian tissue for a considerable period of time.
It shall develop necessary measures to disclose such records in the future upon the request of the client and/or the child.” This does not indicate a specific management system. Accordingly, the long-term storage system should be stabilized in the future, and guidelines for a proper management system should be provided. In the United States, since crises have continued to occur, countermeasures have been proposed. 28 In Japan, the national government, ministries, and agencies need to take the lead in providing guidelines for the management and maintenance of long-term storage systems.
Fertility preservation is self-funded, although it is covered by public subsidies. 29 The cost varies by facility, and patients may decline fertility preservation if the cost is too high. In addition, patients may not continue specimen storage if the cost is too high because there is no public subsidy for renewal costs. Most facilities set oocyte cryopreservation costs up to 400,000 yen, and embryo cryopreservation costs up to 500,000 yen; however, a few facilities set higher costs (Fig. 5). Most facilities set renewal costs between 10,000 and 20,000 yen, and few facilities have a large long-term patient burden of 50,000 yen or more (Fig. 5).
In Denmark, as fertility preservation is practiced almost exclusively in public hospitals, patients who are eligible can receive it free of charge. Israel and Spain likewise offer free fertility preservation, and in Belgium, it is covered by public insurance. In Germany, ovarian tissue cryopreservation is covered by public insurance, but oocyte cryopreservation is not. 29 Although there are differences among countries, efforts to reduce the burden on patients are being made in several countries.
Reproductive specialists who perform fertility preservation should follow up with patients on a regular basis. Approximately 60% of the facilities confirmed the intention to renew by medical examination, whereas other facilities sent out renewal notices by mail (Fig. 6). The embryologists and office staff performed clerical processing of the mail. For patients with cancer, the doctor should check the patient's condition as regularly as possible and provide guidance on what to do next.
Since fertility preservation specimens are stored for prolonged periods of time, they often occupy a certain amount of exclusive storage space in facilities. Therefore, it is necessary to discard specimens that are no longer used because of the death or aging of patients, so that new patients are not affected. Even in cases in which a patient has been out of contact for a long time, it is not easy to discard the specimens because they are valuable. We found that ∼40% of facilities extended the storage period if they could not confirm the patient's intention to renew by phone or mail or confirm their survival with their primary oncologist (Fig. 8). Therefore, we consider it necessary to take sufficient measures, such as obtaining multiple contacts during the cryopreservation stage.
Since fertility preservation is intended for patients with cancer, it is critical to clarify pregnancy outcomes using specimens after the cancer has resolved. 30 Even in private clinics, it is crucial to establish a system that can follow up on a patient's disease status, pregnancy, and survival. Consequently, consistent management guidelines are necessary to ensure the long-term stable management of fertility preservation specimens, such as clarifying who is responsible for the management of fertility preservation specimens, formulating guidelines for the management of liquid nitrogen, checking the status of the patient at the time of renewal, taking measures in case of loss of contact, and taking measures in case of disaster and facility closure.
The Japanese government initiated a public subsidy program in 2021 to provide financial support for fertility preservation for cancer patients, and a national registry project was initiated to identify outcomes in Japan after fertility preservation. Furthermore, the registry project will begin providing financial support to patients for assisted reproduction using fertility preservation specimens in 2022, and it is anticipated that the renewal costs will be subsidized in the future. The project aims to enable the government to centrally manage the storage status of fertility preservation specimens.
Conclusions
Facilities that perform fertility preservation should establish management protocols for their storage systems; thus, it is necessary to create standardized guidelines for the long-term storage system of cryopreserved specimens and these guidelines should be applied to facilities implementing fertility preservation throughout Japan, in cooperation with the government.
Footnotes
Authors' Contributions
T.M. conceived the project. T.M., S.T., M.T., K.O., A.H., T.S., Y.T., F.K., T.F., T.I., and N.S. designed the study. T.M. performed the research. T.M. and H.T. analyzed the data. T.M. mainly wrote the article. T.M., S.T., and N.S. drafted the article and conducted critical discussion. All authors approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by a Ministry of Health, Labour, and Welfare Research for Promotion of Cancer Control Program Grant (20EA1004) obtained by N. Su.