
Abstract
Purpose:
Adolescent and young adult (AYA) oncology patients experience unique biological, behavioral, and socioeconomic challenges, for which provision of care must be tailored. AYAs with central nervous system (CNS) tumors and sarcomas represent a vulnerable population with worse outcomes and potential for serious sequelae from intense multimodal therapy. Comorbidity burden impacts treatment tolerance, adherence, and efficacy, yet has been understudied among these high-risk AYA patients.
Methods:
Utilizing a validated AYA oncology comorbidity index, we (1) measured comorbid conditions present at diagnosis in AYA-aged patients with CNS tumors and sarcomas and (2) compared baseline comorbidity burden across ascending AYA age groups (15–19, 20–29, and 30–39 years) and with pediatric patients (10–14 years).
Results:
The cohort included 131 AYAs and 50 pediatric patients. Mean comorbidity score significantly differed between pediatric (0.8) and AYA (1.7) patients, and across ascending age subgroups (0.8 [10–14] < 1.2 [15–19] < 1.7 [20–29] < 2.5 [30–39]). AYAs were significantly more likely than pediatric patients to have ≥2 or ≥3 comorbidities (47% vs. 18%, 24% vs. 6%), with increasing prevalence across ascending age subgroups. Frequency of overweight/obese status, smoking/substance use, obstetric/gynecologic conditions, and cardiovascular comorbidities increased with age. In multivariate analyses adjusting for sex, tumor type, and race, age remained a significant predictor of comorbidity score.
Conclusions:
AYAs with CNS tumors or sarcomas have a high burden of baseline comorbidities, which increase with age at diagnosis, conferring susceptibility to treatment-related toxicity and mortality. Improving the prognosis for AYAs requires appropriate identification of pre-existing comorbidities and tailoring therapeutic and supportive care accordingly.
Introduction
Adolescents and young adults (AYAs) account for >70,000 new cancer diagnoses annually in the United States1,2 and represent a distinct patient group with unique medical, developmental, and psychosocial needs.3,4 Despite advances in oncology treatments over recent decades, AYA-aged patients continue to experience slower improvement in outcome than pediatric or later adult counterparts.5,6 Inferior survival has been demonstrated among AYAs compared with younger children and/or older adults for several cancer types, including central nervous system (CNS) tumors7–9 and sarcomas.10,11 There is growing recognition of biological, behavioral, and socioeconomic challenges inherent to AYA oncology, for which provision of care must be tailored.3,6,12,13
Comorbidity burden at diagnosis has been shown to be associated with poorer quality of life and higher mortality risk among adults with cancer and other diseases.14–16 Oncology patients with greater comorbidities are more susceptible to therapy-related toxicity, with resultant decreased treatment tolerance and adherence, increased need for hospitalizations, and higher health care costs.15,16 Although studies have assessed the prevalence of chronic comorbidities among survivors of AYA cancers,17,18 data regarding baseline health conditions at initial oncologic diagnosis are lacking. Consistently higher rates of cardiovascular disease,17,19,20 respiratory conditions,17,19,21,22 and psychiatric disorders17,23–27 were observed in AYA survivors compared to age-matched healthy controls. However, much less is known about the presence of underlying comorbidities among AYA patients before beginning cancer therapy.
Parsons et al. and Wu et al. assessed relevant medical conditions at diagnosis within a cohort of AYA survivors of primarily hematologic malignancies and extraneural germ cell tumors.28–30 Using a comprehensive comorbidity index developed specifically for the AYA oncology population (AYA Health Outcomes & Patient Experience [HOPE]), the authors identified that baseline comorbid conditions increased with age. 28 The number of comorbidities at diagnosis also correlated with subsequent mental health service needs, poorer overall self-reported health status, and decreased likelihood of returning to work or school following cancer treatment.29,30 While comorbid conditions varied by age within AYA cohorts, no comparison was made to younger patients, although children and AYAs are increasingly treated together at pediatric oncology centers.31–34
In addition, while these studies provide valuable insight into the prevalence and negative impact of baseline comorbidity burden among AYAs with more common cancer types,28–30 they excluded patients with CNS tumors and included relatively few patients with sarcomas. AYAs diagnosed with CNS tumors and sarcomas comprise a vulnerable patient population, given the aforementioned poorer outcomes as well as need for intense, multimodal treatment (surgery, radiation, and/or chemotherapy) with risk of serious sequalae. Despite their contribution to cancer-related morbidity and mortality among AYA patients, CNS tumors and sarcomas have remained relatively understudied and underrepresented within AYA research to date.9,35
Utilizing a representative cohort of AYA-aged patients with primary CNS tumors or sarcomas, we sought to (1) quantify and characterize comorbid conditions present at the time of initial oncologic diagnosis and (2) compare baseline comorbidity burden across ascending AYA age groups, as well as with younger pediatric counterparts.
Methods
Population
This retrospective study was performed at Cincinnati Children's Hospital Medical Center (CCHMC), an academic pediatric center with a large AYA oncology program. IRB approval was obtained before study initiation. Patients were included if they were diagnosed between 10 and 39 years of age with a (1) primary CNS tumor or (2) sarcoma or related mesenchymal solid tumor with similar multimodal treatment and morbidity risk (hereafter termed sarcoma), and received care between 2014 and 2019. All AYAs ≥30 years, who met these criteria, were included. As the number of eligible younger patients was much greater (not feasible to manually review all), subjects were selected for inclusion to ensure a representative distribution of ages, gender, and diagnoses; selection was blinded to comorbidity status. Patients with a previous cancer history or insufficient records were excluded.
Comorbidity identification and scoring
Electronic medical records were manually reviewed to collect clinical data and identify baseline comorbidities at the time of oncologic diagnosis, before treatment initiation. Comorbidities were classified and scored according to the AYA HOPE comorbidity index,28–30 which includes diagnoses across 14 organ system/disease groups (cardiovascular, diabetes, endocrine, gastrointestinal, HIV/AIDS, hypertension, liver, mental health, neurological, obesity/overweight, renal, asthma/respiratory, rheumatologic/autoimmune, and hematologic), with one point assigned for each comorbidity. Distinct, unrelated comorbidities within the same category, each, received a point, such that there is no maximum score.
In addition to these 14 categories, for most analyses, we also included comorbidities related to (1) substance use (current or previous tobacco or marijuana use, excessive alcohol consumption [≥15 drinks/week], and illicit drug use) and (2) obstetric/gynecologic conditions (e.g., pregnancy complications, polycystic ovarian syndrome), given their potential to impact health and treatment tolerance. Conditions that were acute, self-limited, and/or related to the patient's cancer diagnosis (e.g., seizures in a patient with a CNS tumor of epileptogenic location) were excluded. Only chronic, significant, and nontumor-related comorbidities were included. Patients with body mass index (BMI) ≥25.0 (overweight or obese) before starting therapy received a point, as previously described.28–30 In addition, to ensure all patients with suspected hypertension were captured, patient's blood pressures (BPs) over at least three separate visits, close in time to initial oncologic diagnosis, were recorded, excluding measurements from encounters where values may be situationally elevated.
Patients with persistent systolic BP (SBP) ≥130 (or above respective 95th percentile for age, gender, and height 36 ) across multiple visits without known causes received a point; patients with pre-existing known hypertension received a point regardless of SBP measurements. Comorbid conditions were summed (all weighted equally) to determine a total comorbidity index score for each patient. Electronic medical record review and comorbidity data abstraction were consistently performed by a single oncology reviewer (M.A.L.), with de-identified data saved in password-protected files, from which analysis results could be regularly reviewed by the study team.
For a secondary analysis exploring the development of mental health comorbidities during and/or after oncologic treatment, data regarding psychiatric diagnoses (anxiety disorder, depression or other mood disorder, and attention-deficit/hyperactivity disorder) and corresponding medication management needs were manually abstracted.
Statistical analysis
Baseline comorbidities were compared between pediatric patients (10–14 years) and AYAs (15–39 years), and across the four age groups (pediatric plus AYA subgroups [15–19, 20–29, and 30–39 years]). 29 Chi-square and Fisher's exact probability tests were performed to compare prevalence of comorbidities (1) between pediatric and AYA patients and (2) across all four age groups, respectively. Multivariate linear regression analysis was performed to evaluate the significance of age (continuous variable), sex, tumor category (CNS or sarcoma), and race (non-Hispanic white, non-Hispanic black, other) to predict comorbidity score. Comparisons of mean baseline comorbidity score and BMI were each performed using t-tests and one-way analysis of variance.
Results
Cohort
A total of 181 patients were analyzed, with clinical and demographic features summarized in Table 1. This cohort included 131 AYA-aged patients (15–19 years [n = 55], 20–29 years [n = 50], and 30–39 years [n = 26]) and 50 pediatric patients (10–14 years).
Clinical and Demographic Characteristics of the Pediatric and Adolescent and Young Adult Patients in the Cohort
AYA, adolescent and young adult; CNS, central nervous system; DIPG, diffuse intrinsic pontine glioma; DNET, dysembryoplastic neuroepithelial tumor; NOS, not otherwise specified; SD, standard deviation.
Baseline comorbidities
Total baseline comorbidity score
Total comorbidity scores ranged from 0 to 3 among pediatric patients and 0 to 6 among AYAs. There were significant differences in mean total comorbidity score between pediatric (0.8) and AYA (1.6) patients, and across the four ascending age subgroups (0.8 < 1.2 < 1.7 < 2.5; p < 0.001) (Table 2 and Fig. 1). Findings were similar between patients with CNS tumors and sarcomas (Fig. 1B, C). AYA patients were more likely than pediatric patients to have ≥1 comorbidity (77% vs. 52%, p < 0.001), with increasing frequency of comorbidity prevalence as age increased (69% [15–19], 80% [20–29], and 88% [30–39]; p < 0.01).
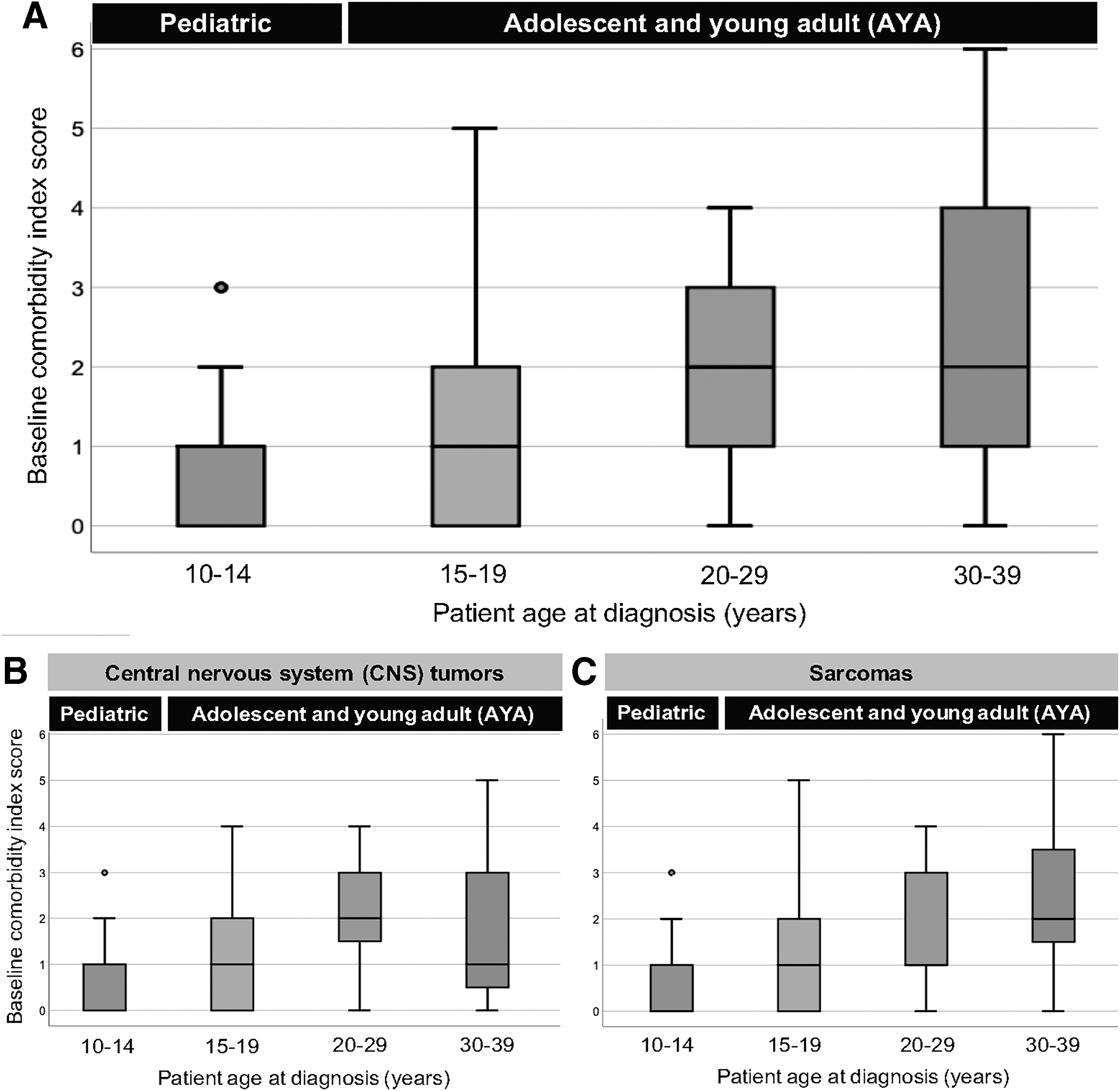
Baseline comorbidity index scores for pediatric and AYA patients, with median and range illustrated.
Summary of Comorbidity Scores and Association with Patient Age Group
Comparisons of mean comorbidity score were performed using t-tests and one-way ANOVA. Chi-square and Fisher's exact probability tests were performed to compare prevalence of comorbidities (1) between pediatric and AYA patients and (2) across all four age groups, respectively.
Significant p -values (<0.05).
ANOVA, analysis of variance; HOPE, Health Outcomes & Patient Experience.
When patients were categorized by comorbidity scores of 0, 1, ≥2, or ≥3, there were significant differences between pediatric and AYA patients, and across all age groups (Table 2). AYA patients were more likely than pediatric patients to have ≥2 or ≥3 comorbidities (47% vs. 18%, and 24% vs. 6%; p < 0.01), and these rates increased across the four ascending age subgroups (p < 0.001, Table 2 and Fig. 2A). In multivariate linear regression analysis adjusting for sex, tumor type, and race, age remained a significant predictor of comorbidity score (p < 0.001). Finally, when only assessing comorbidities included in the AYA HOPE index (excluding substance use and obstetric/gynecologic conditions), similar findings of increasing comorbidity burden with ascending age group were observed (Table 2).
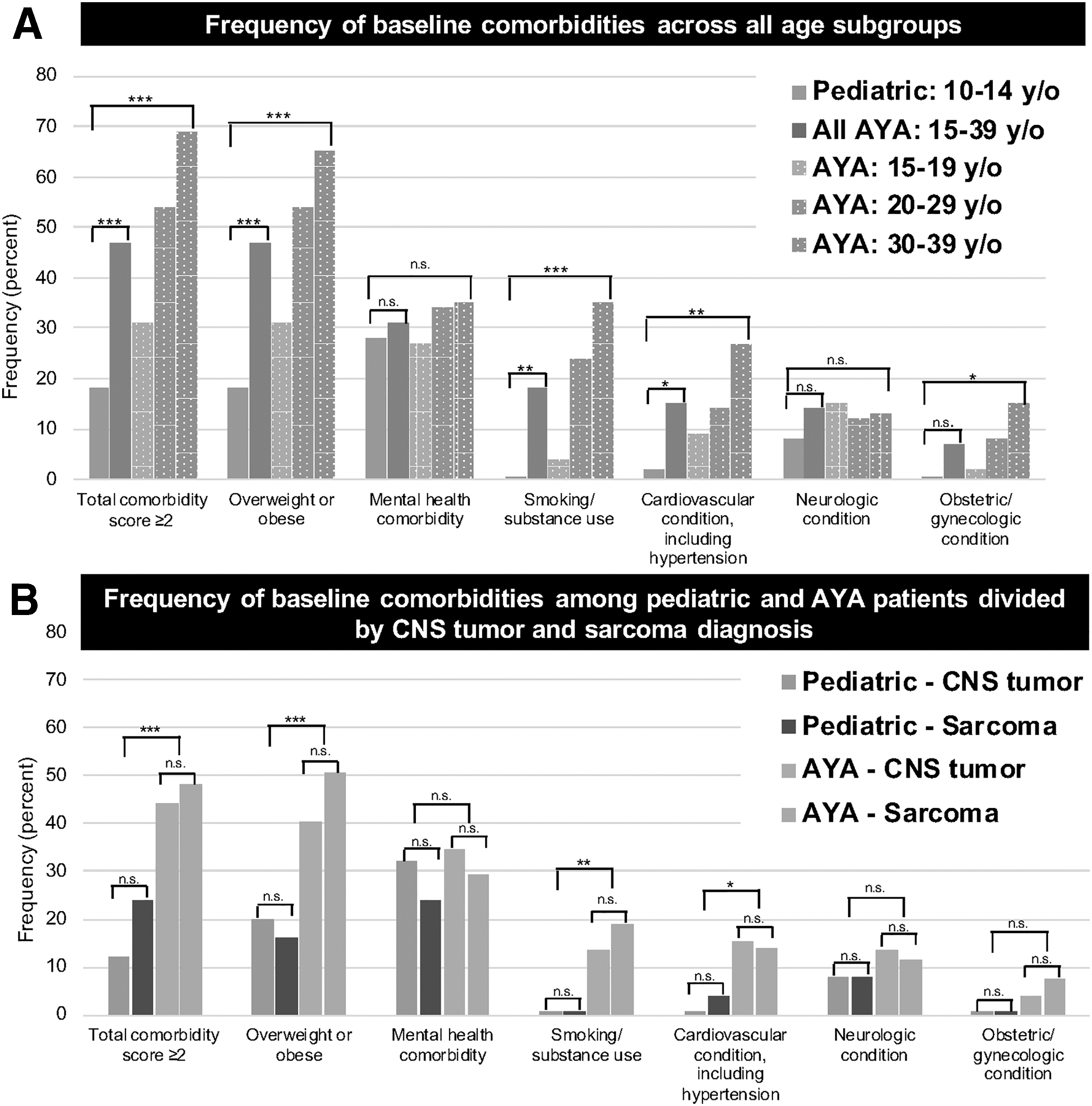
Bar graphs illustrating frequency (percentage) of total baseline comorbidity score ≥2, as well as specific disease-focused baseline comorbidities between pediatric and AYA patients, across all age subgroups
Specific baseline comorbidities
The most prevalent baseline comorbidity categories among all AYAs were overweight/obese status (47%), mental health (31%), smoking/substance use (18%), cardiovascular, including hypertension (15%), and neurologic (14%) (Table 3 and Fig. 2). AYA patients had significantly higher rates of overweight/obese status, smoking/substance use, and cardiovascular comorbidities than pediatric patients (as well as a trend toward more prevalent obstetric/gynecologic conditions), with increasing frequencies across ascending age groups (p < 0.05, Table 3 and Fig. 2).
Summary of More Prevalent Comorbidity Categories and Association with Patient Age
Chi-square and Fisher's exact probability tests were performed to compare prevalence of comorbidities (1) between pediatric and AYA patients and (2) across all four age groups, respectively.
Significant p values (<0.05).
There were significant increases in mean BMI when comparing pediatric (20.9) and AYA (25.9) patients, and across the four ascending age groups (20.9 < 23.7 < 27.4 < 27.6, p < 0.001). Mental health diagnoses were prevalent in both pediatric (28%) and AYA (31%) patients, without significant differences (Table 3). The prevalence of neurologic, gastrointestinal, or respiratory comorbidities did not differ by age, although lower frequencies. No significant difference in prevalence of specific comorbidities was observed between patients with CNS tumors and sarcomas, assessed across both pediatric and AYA cohorts (Fig. 2B).
Chronic and/or acquired mental health conditions after oncologic diagnosis
Given the aforementioned high prevalence of mental health comorbidities at initial diagnosis across all pediatric and AYA age groups, we explored rates of subsequent chronic and/or acquired mental health conditions between the time of oncology diagnosis and last follow-up. Among patients with sufficient follow-up records (n = 171), mental health diagnosis rates more than doubled in all pediatric and AYA age groups (Table 4). There was no significant difference in frequency of subsequent chronic and/or acquired mental health comorbidities when comparing pediatric and AYA patients, although a trend toward higher rates in older patients was observed (p = 0.063). When evaluating the use of scheduled medications for mental health comorbidities (i.e., selective serotonin reuptake inhibitors) following the time of oncology diagnosis, there were similarly high rates between pediatric (41%) and AYA patients (49%), although significant differences were identified across ascending AYA subgroups (Table 4).
Summary of Chronic and/or Acquired Mental Health Diagnoses Among Pediatric and Adolescent and Young Adult Patients with Sufficient Follow-Up Records
Chi-square and Fisher's exact probability tests were performed to compare prevalence of comorbidities (1) between pediatric and AYA patients and (2) across all four age groups, respectively.
Significant p values (<0.05).
Discussion
Despite growing recognition of the biologically, molecularly, and socioeconomically distinct challenges of treating AYA cancers, the needs of AYA oncology patients continue to be inadequately addressed.1–4 Improving outcomes for AYAs requires expanded awareness and education of underlying health conditions that impact treatment tolerance, adherence, and efficacy.28–30,37 AYAs diagnosed with CNS tumors and sarcomas represent a vulnerable population with historically worse outcomes than pediatric or older adult counterparts and frequent need for intense, multimodal therapy, yet remain underserved in AYA oncology research.9,35 To our knowledge, this is the first comprehensive assessment of baseline comorbidity burden among AYAs with CNS tumors and sarcomas; this study also provides the first comparison of comorbidity prevalence between AYA and pediatric patients. Utilizing a validated comorbidity index tailored for the AYA oncology population,28–30 we measured and characterized comorbid conditions present before beginning cancer treatment, with important clinical implications.
In our neuro-oncology and sarcoma cohort, baseline comorbidities increased with ascending age among AYA patients and were greater in AYAs than younger children. This positive correlation between comorbidity burden and age at diagnosis remained significant in multivariate analyses after accounting for patient sex, tumor type, and race. Prior research similarly demonstrated increasing number of comorbid illnesses with increasing age in older adult cancer patients.38–40 Parsons et al. described a higher prevalence of comorbidities in older AYAs than younger AYAs within a large sample of primarily hematologic malignancy and extraneural germ cell cancer patients. 28 Our study expands upon this earlier work by applying similar analyses to AYAs with CNS tumors and sarcomas, revealing that baseline comorbidity burden also increases along the age continuum of both these high-risk diseases.
Appropriately identifying pre-existing comorbidities and tailoring therapeutic and supportive care accordingly will be critical to improving the prognosis for AYAs. Comorbidity number and breadth have been shown to be inversely correlated with treatment tolerance, survival outcomes, and health-related quality of life in adult cancer patients.14–16 In our cohort, at least two baseline comorbid conditions were present in approximately half of AYAs and nearly 70% of patients 30–39 years of age.
Furthermore, the most prevalent categories include diseases with potential to increase therapy-related morbidity and mortality. First, almost half of AYAs were overweight or obese at initial diagnosis, which has been associated with poorer survival and greater risk of treatment complications in oncology patients.41,42 Mental health disorders were the second most prevalent comorbidity among AYAs, pre-existing in almost one-third of patients. In adult oncology populations, underlying psychiatric conditions are independently correlated with cancer-specific and all-cause mortality.43,44 Third, baseline smoking or substance use was observed in 18% of AYAs and 35% of AYAs 30–39 years of age.
Across many cancers, smoking status is predictive of less favorable response, worse outcomes, and therapy-related toxicity (including pulmonary complications).21,45 Use of substances and illicit drugs further complicates oncology care due to potential interactions with prescribed medications, increased exposure to blood-borne illnesses, and/or concurrent psychiatric disorders.46,47 Finally, in contrast to the near absence of hypertension in children, 11% of AYAs (23% of patients 30–39 years of age) had pre-existing hypertension, which increases the likelihood of chemotherapy-induced cardiovascular toxicity, especially ventricular dysfunction. 48
Due to their high burden of baseline comorbidities, AYA patients with CNS tumors and sarcomas have increased susceptibility to treatment-induced toxicity and mortality, which requires targeted interventions. Whenever possible, efforts should be undertaken to reduce the severity of comorbidities and mitigate their potential adverse effects. For example, to address obesity and substance use concerns, AYA patients should be offered lifestyle counseling services that promote healthy dieting, regular physical activity, and smoking/illicit drug cessation.21,47,49,50 Closer monitoring for potential therapy-related complications should also be performed in AYA patients. Decisions about treatment paths and dosing should incorporate risk/benefit algorithms that account for the heightened toxicity risk AYAs experience due to pre-existing comorbidities. Moreover, as AYAs are increasingly being treated at pediatric cancer centers,31–34 it is imperative that pediatric oncologists receive adequate training regarding management and modification of their comorbid conditions. 37
Mental health disorders were prevalent in AYA and pediatric patients alike, representing one of the few comorbidity categories with similar frequencies across all age subgroups (∼30% throughout). High rates of psychosocial distress and adverse mental health outcomes have consistently been demonstrated in survivors of AYA cancers, increased compared to healthy peers.17,23–27 However, less has been studied about underlying psychiatric comorbidity burden in AYAs at the time of initial oncologic diagnosis, despite an identified association with inferior survival among older adult cancer patients.43,44,51,52
A high prevalence of mental health comorbidities was seen at baseline among AYA (and pediatric) patients with CNS tumors and sarcomas, which more than doubled following oncology therapy in all age groups. Approximately half of the cohort's AYA (and pediatric) patients were treated with a scheduled medication for psychiatric conditions during and/or after completing cancer therapy. These findings suggest that patients of all ages may have mental health needs at diagnosis, which have the potential to significantly worsen over time, serving as an alarm call for early recognition and routine monitoring of psychiatric distress in both AYA and pediatric patients throughout their oncology journey.
We observed a higher prevalence of baseline comorbid conditions among AYA patients than previously reported by Parsons et al. and Wu et al.28–30 Seventy-nine percent of AYAs in our cohort had at least one comorbidity at the time of oncologic diagnosis, compared with rates of 30%–35% in these prior studies.28–30 Although we used the same comorbidity index with similar scoring methodology, our evaluation incorporated two additional categories: (1) smoking and substance use and (2) obstetric/gynecologic conditions, given their aforementioned relevance to overall health and oncology therapy-related toxicity.21,45,53 Comorbidities within either and/or both categories were identified in 28% of our AYA cohort, which may partially explain the differences noted and provide further support for including these conditions in future research.
In addition, a much greater proportion of AYA patients in this study were classified as overweight or obese (47%) compared to earlier reports (3%–6%), using identical BMI definitions.28,29 Geographic, temporal, and/or selection factors may account for differences in the presence of obesity and other comorbidities. On average, our cohort included AYAs diagnosed 10 years later than previous studies, so the higher overweight/obesity rates likely reflect their known increasing prevalence over time; furthermore, the frequency of obese pediatric and AYA patients in our study is similar to that reported among corresponding age groups within the general U.S. population.54,55 Underlying mental health diagnoses were also more common among AYAs evaluated in this work compared to earlier reports (7%–8%).28,29
Results of prior AYA research exploring baseline comorbid conditions may have been partially skewed by only including survivors who consented to completing surveys about subsequent health care needs.29,30 Nearly all AYA patients with CNS tumors or sarcomas with sufficient medical records were eligible for this study, thereby minimizing sampling bias. Taken together, our findings not only provide new information about comorbid conditions in AYAs with CNS tumors and sarcomas specifically but also potentially a more accurate, relevant, and contemporary understanding of baseline AYA comorbidity burden overall.
This study was limited by the modest sample size and retrospective, single-institutional approach, which may decrease generalizability of results. It was not possible to analyze all AYA and pediatric patients <30 years of age, and selection of these younger subjects was performed manually, which has the potential to confer bias; however, selection was blinded to comorbidity status and conducted to ensure a representative distribution of ages, gender, and specific diagnoses. Future research performed in a larger, comprehensive cohort across several sites will be important to corroborate findings. In addition, while this report offers a useful cross-sectional view of underlying comorbidities in AYAs that can guide clinical practice, we did not assess correlation with subsequent treatment-related morbidity, survival, or other health outcomes, which will be essential to explore further.
In conclusion, this work provides valuable insight regarding baseline comorbid conditions present in AYA patients with CNS tumors and sarcomas, a previously understudied population. Comorbidity burden at diagnosis increased with ascending AYA patient age and was greater in AYAs compared to younger, pediatric counterparts, with similar results within both diseases. There was a high prevalence of pre-existing mental health disorders across age groups, with consistent worsening of psychologic distress during and following treatment. Given potential for therapy-related toxicity and mortality, targeted interventions to decrease comorbidity severity and mitigate adverse effects among AYA oncology patients are critically needed.
Footnotes
Authors' Contributions
Conception and design: M.A.L., R.S., and J.G.P. Data acquisition: M.A.L. Data analysis and interpretation: M.A.L., R.S., and J.G.P. Drafting and revising critically for important intellectual content: M.A.L., R.S., and J.G.P. Final approval of submission: M.A.L., R.S., and J.G.P.
Author Disclosure Statement
The authors have no conflicts of interest.
Funding Information
No funding was received for this article.