
Abstract
Purpose:
Improved symptom management is a critical although unmet post-treatment need for young adult (YA) cancer survivors (aged 18–39 at diagnosis). This study aimed to develop and refine a behavioral symptom management intervention for YA survivors.
Methods:
Phase I: YA survivors (N = 21) and oncology providers (N = 11) completed individual interviews and an online, self-report assessment to examine symptom experiences, the need for a behavioral symptom management intervention for YAs, and perceptions about potential intervention components, structure, and format. Phase II: YA survivors (N = 10) completed user testing sessions, providing feedback on the prototype intervention materials (paper manual and mobile application), and completed an online assessment. Quantitative data were examined using descriptive statistics. Rapid qualitative analysis, a methodologically rigorous standardized approach, was used.
Results:
Pain, fatigue, and distress were ranked as top concerns by most YAs and providers. Phase I interviews underscored the need for a symptom management intervention for YAs. YAs and providers highlighted potential coping strategies and program format/structure suggestions (e.g., small group format) to best meet YAs' needs. A prototype intervention was developed combining the following: traditional behavioral symptom coping skills; home-based physical activity; strategies from Acceptance and Commitment Therapy and Meaning-Centered Psychotherapy; and strategies to foster self-compassion. Phase II user testing sessions highlighted strengths and suggestions for refining the prototype materials.
Conclusion:
Post-treatment symptoms are common for YAs. A tailored behavioral symptom management program was developed and refined with input from YAs and providers and will be examined for feasibility and acceptability in a pilot randomized controlled trial.
Clinical Trial:
Clinicaltrials.gov identifier NCT04035447
Introduction
In the United States, there are >600,000 survivors of young adult (YA) cancer, aged 18–39 at diagnosis. 1 Treatments for YA survivors can result in persistent2–4 physical symptoms (e.g., pain, fatigue)5–7 and emotional distress (e.g., anxiety, depression).7–11 YA survivors are diagnosed during a critical developmental period when they are working to achieve complex, age-related goals (e.g., educational, career, relationships, family building).12–15 Physical symptoms and emotional distress disrupt YAs' abilities to achieve life goals and plan for the future2,5,16–21 and contribute to significant social, economic, and health care burden.22–25
Symptom management is rated by YA survivors as a critical although unmet health care need5,26,27 and is a significant issue in their transition to survivorship.28,29 YAs often lack confidence in managing physical symptoms and distress and have more difficulty coping with these challenges than older or younger survivors.30,31 The National Cancer Institute32,33 and the National Academy of Medicine (formerly Institute of Medicine) 34 have highlighted the critical need for interventions to reduce symptom burden and promote self-efficacy and self-management of symptoms for YA survivors. However, there remains a paucity of evidence-based symptom management interventions for YAs.
The majority of symptom management interventions for YAs with cancer target symptoms experienced in the context of adjuvant treatment.35–37 Interventions developed for YA survivors post-treatment have focused on reducing psychological symptoms;38–40 yet physical symptoms often co-occur, are interrelated with psychological symptoms,5,41 and these co-occurring symptoms are associated with greater symptom intensity and interference.42,43 Meta-analytic data and reviews of studies conducted with primarily older (M > 40 years) cancer survivors suggest that behavioral symptom management interventions result in significant reductions in physical and psychological symptoms, improved self-efficacy for symptom management, and decreased symptom interference.44–49 However, YAs represent a small portion of the overall study samples49–52 ; consequently, the efficacy of these interventions for YA survivors is largely unknown. In addition, symptoms often impact valued life areas for YA survivors that may be unique to their developmental stage and activities consistent with their life phase (e.g., education, career, parenting). The approaches needed to promote symptom management and address symptom interference that have been evaluated among older cancer survivors may not consider and/or address the unique needs associated with YAs' developmental stage.
Guided, in part, by the ORBIT Model of behavioral intervention development for chronic diseases,53–55 our objective was to develop and refine a novel behavioral symptom management intervention targeting both physical and psychological symptoms to meet the needs of YA survivors.
Methods
Setting and participants
Study procedures received institutional review board approval (Pro00103249). Eligible survivor participants had: (1) received a cancer diagnosis between ages 18 and 39; (2) received a diagnosis of hematologic, breast, endocrine, or gastrointestinal cancer, melanoma, or germ cell tumor; and (3) completed curative treatment involving multimodal therapy within the last 5 years. Additional eligibility criteria included the ability to speak/read English and provide informed consent. Exclusion criteria included major or untreated/uncontrolled mental illness. Eligible oncology providers were involved in the care of YAs.
Participants were recruited between January 2020 and April 2021. Survivor participants were identified using electronic medical records. A letter was then sent to the survivors, and they were subsequently contacted through telephone. Provider participants were contacted through email. All participants provided written informed consent and were compensated $30.
Phase I: intervention development
During the Discovery Phase of the ORBIT Model, the primary goal is to identify a significant clinical problem. 55 We aimed to achieve this goal during Phase I by obtaining feedback from providers and YA survivors about YAs' symptom experiences, the need for a behavioral symptom management intervention for YAs, and participants' perceptions about potential intervention components, structure, and format.
Recruitment letters were sent to 42 survivors; 69% (n = 29) were able to be screened for eligibility. Of these, 76% (N = 22) consented. Twenty-one interviews were completed; one survivor was lost to follow-up after consent. Participants declined due to time (n = 2) or lack of interest (n = 2). Three interested participants were lost to follow-up before consent. Fourteen oncology providers were approached; N = 11 (79%) consented and participated.
Individual survivor interviews (N = 21) were ∼60 minutes and completed through telephone. Provider interviews were completed in-person (n = 10) or through Zoom (n = 1; due to COVID-19). Interviews were conducted by the study PI (C.S.D.), informed by semistructured interview guides (Supplementary Materials), and audio recorded. Survivors and providers were asked about survivors' physical and psychological symptom concerns after cancer, symptom interference with life goals and relationships, communication with health care providers about symptoms, and strategies/interventions to address symptoms and their efficacy. Survivors and providers commented on the need for and benefit of a behavioral symptom management intervention targeting YAs and provided input on potential intervention components and the proposed intervention structure/format.
Phase II: intervention refinement
During the Design Phase of the ORBIT model, the focus is on defining and refining acceptable and feasible components of a behavioral intervention.53–55 The use of qualitative research methods with small sample sizes has been suggested to gather feedback on an intervention's components and their feasibility and acceptability53,55 while also further refining the intervention to move toward subsequent iterative steps of the ORBIT model.
Recruitment letters were sent to a new pool of 27 YA survivors, and 70% (n = 19) were screened for eligibility. Fifty-eight percent (n = 11) of eligible survivors consented and completed online questionnaires. One consenting survivor was lost to follow-up before the user testing session. The remaining individuals were lost to follow-up before consent (n = 6) or declined (n = 2; lack of time).
The developed intervention included printed intervention materials and a mobile application, both of which would be used by YAs during their participation in the symptom management program. User testers reviewed the prototype intervention materials over Zoom with a member of the study team (C.S.D. or J.M.S.), with half (n = 5) reviewing the printed materials and half (n = 5) reviewing the intervention-specific mobile application. Structured session guides were used to direct YAs' review and discussion of the study materials (Supplementary Materials). User testing sessions were ∼60 minutes and audio/video recorded.
Survivors reviewing the printed intervention materials provided input on the layout, content, and length of materials. Survivors reviewing the application commented on its layout and functionality/usability. User testers were asked about the applicability of the images, examples, and intervention strategies to YA survivors' experiences and to provide suggestions for improving relevance.
Study measures
All study participants completing either phase I or phase II completed a brief online assessment.
Survivor assessment
Survivors provided medical (e.g., cancer diagnosis, treatment history) and sociodemographic information as well as information about their symptom experience.
Symptoms
Psychological distress in the last week was assessed using the Patient-Reported Outcomes Measurement Information System (PROMIS) Depression (eight-item) and Anxiety (eight-item) short forms. 56 Fatigue was assessed using the PROMIS Fatigue (eight-item) short form. Each had good internal consistency reliability across study phases (Depression: α = 0.82–0.93; Anxiety: α = 0.70–0.94; and Fatigue: α = 0.94–0.97). The Brief Pain Inventory 57 assessed pain severity (α = 0.83–0.91) and interference (α = 0.93–0.98) in the last week.
Self-efficacy for managing symptoms
Participants completed the six-item Self-Efficacy for Managing Chronic Disease Scale,58,59 rating their confidence in their ability to keep symptoms from interfering with their life and health (α = 0.88–0.89). Participants also completed the PROMIS Self-Efficacy for Managing Chronic Conditions-Managing Symptoms (four item) short form, 60 rating their confidence in their ability to manage symptoms during daily activities, in relationships, in public places, and in working with their doctor to manage symptoms (α = 0.79–0.89).
Concerns
Survivors rank ordered their top 5 post-treatment concerns from a list, which included pain, fatigue, emotional stress/distress, cognitive problems, sleep problems, sexual problems, fertility, peer relationships, family relationships, finances, and return to work/school. Survivors could also specify other concerns.
Medical provider assessment
Medical providers completed items asking about their demographics, medical training (e.g., degree, years of practice), and training in adolescent and young adult oncology.
Concerns
Providers rank ordered the top 5 concerns endorsed by their patients following treatment from the same list of concerns ranked by survivors, described above (see Concerns section).
Analytic strategy
Data from online assessments were examined using descriptive statistics. Pearson or Spearman correlations were used to examine the relationships between self-report measures completed by survivors.
Interviews and user testing sessions were transcribed verbatim. Rapid qualitative analysis, a methodologically rigorous, standardized approach recommended for intervention development, was used.61–63 Rapid qualitative analysis provides a timely systematic method for analyzing qualitative data without compromising the validity of results.64,65 It allows for the identification of intervention elements as well as barriers and facilitators of a program. 63 Interviews were summarized using a structured template that mapped on to the interview guides. Interview summaries were transferred into a matrix (respondent × interview domain) to summarize key information and interview themes to then identify trends in responses. 66 The use of direct quotes in rapid qualitative analysis is minimal 67 as the goal is to create a brief, although thorough, organized summary of the data. Information obtained from participants was used to develop and refine the prototype intervention and study procedures.
Results
Participants
Survivors (N = 32) were M = 31.9 years old and primarily female (53.1%) (Table 1). The majority of participants were white (71.9%) and non-Hispanic (96.9%), which is consistent with the racial/ethnic breakdown of YA cancer survivors treated at our institution. Survivors had been diagnosed with breast (18.8%), endocrine (i.e., thyroid; 12.5%), gastrointestinal (35.0%), hematologic (21.9%), or germ cell (testicular; 15.6%) cancers or melanoma (6.3%). Survivors were M = 41.9 and M = 28.4 months since diagnosis and treatment completion, respectively.
Sociodemographic and Medical Characteristics and Symptoms Experienced by Young Adult Survivor Participants (N = 32)
Indicated by patient in addition to employer insurance.
CHIP, Children's Health Insurance Program; Dx, diagnosis; PROMIS, Patient-Reported Outcomes Measurement Information System; SD, standard deviation; Tx, treatment.
Providers (N = 11) were M = 42.6 years old and primarily white (90.9%), non-Hispanic (100%), and female (81.8%). Most were medical doctors (90.9%) and had been practicing for M = 12.2 years. Providers treated cancers matching those of survivor participants: breast (18.2%), endocrine (e.g., thyroid: 9.1%), gastrointestinal (18.2%), hematologic (9.1%), germ cell (i.e., testicular: 9.1%; ovarian: 18.2%) cancers or melanoma (18.2%). M = 15.2% (range 4%–30%) of their patient population was aged 18–39.
Quantitative data
Survivors' symptom ratings are presented in Table 1. Fifty percent of YAs endorsed clinically significant levels of pain (i.e., worst pain in the last week ≥3/10). Almost half reported elevated (i.e., t-scores ≥½ standard deviation above the mean) depressive (47%) and/or anxiety (47%) symptoms, and 34% reported elevated fatigue. Table 2 presents survivors' and providers' rankings of post-treatment concerns. Close to one-third of survivors (31.3%) ranked emotional stress/distress as their primary concern, followed by fatigue (15.6%) and pain (12.5%). Pain, fatigue, or emotional stress/distress was ranked as the primary or secondary concern by ∼91% of survivors. Just under half of providers ranked fatigue (36.4%) or pain (9.1%) as the primary post-treatment concern for their patients, with pain, fatigue, or emotional stress/distress ranked as the primary or secondary concern by ∼81% of providers.
Survivor and Provider Concerns
Due to missing data, percentages may not equal 100.
Significant positive correlations were found between depression, anxiety, fatigue, and pain severity (rs = 0.39 to 0.76; ps < 0.05; Table 3). Participants with greater self-efficacy for managing chronic disease experienced fewer symptoms of depression, anxiety, and fatigue and lower pain severity and interference (rs = −0.45 to −0.56; ps < 0.05). Those with greater self-efficacy for managing symptoms experienced fewer symptoms of depression, anxiety, and fatigue and less pain interference (rs = −0.37 to −0.62; ps < 0.05).
Bivariate Correlations Between Symptoms and Symptom Self-Efficacy for Total Sample of Survivor Participants (N = 32)
p ≤ 0.05; **p ≤ 0.01.
Results confirmed that an intervention targeting multiple symptoms that are highly correlated (i.e., pain, fatigue, and emotional distress) as well as aiming to improve participants' self-efficacy for symptom management may be particularly beneficial for YAs.
Phase I: Intervention development interviews
Need for the proposed intervention: Symptom experience of YAs
Survivors' qualitative data highlighted post-treatment pain, fatigue, and emotional distress. Symptoms served as reminders of their cancer and contributed to feelings of anger, anxiety, and low mood. Some survivors expressed resignation around the persistence of symptoms. Survivors also endorsed increased irritability and a “shorter fuse,” which impacted their relationships with friends, family, and their children. Those experiencing fatigue described it as having both a mental and physical component, with stress being associated with greater fatigue. Physical activity and adequate sleep were associated with lower fatigue. Survivors acknowledged a sense of grief/loss about life areas (e.g., biological parenthood, changing careers) that had changed or were different than they had hoped/planned.
Providers' qualitative data pointed to pain, fatigue, and distress as common post-treatment symptoms for YAs. Providers acknowledged that symptoms such as fatigue may be persistent. They reflected that post-treatment symptoms can contribute to additional distress as symptoms may last longer than survivors anticipate, interfere with important life areas (e.g., work/school, raising children, relationships), or are perceived as signs of cancer recurrence.
Figure 1 presents unique and common factors contributing to distress for YA survivors as reported by YAs and oncology providers.

Factors contributing to post-treatment distress among YA survivors as reported by survivors and providers. YA, young adult.
Symptom management strategies
YA survivors shared about strategies to cope with and manage post-treatment symptoms. Several endorsed the importance of social support, describing talking to other young cancer survivors (e.g., through chat rooms or support groups), communicating their needs for emotional and instrumental support, and receiving support from friends and family as beneficial. They also described value in communicating with their medical team about their symptoms for addressing and understanding the source and trajectory of their symptoms. Physical activity was endorsed as beneficial for coping with pain, fatigue, and distress.
Some YAs described a shift in what was meaningful to them and a desire to spend time on meaningful goals even if it meant approaching goals in a new way to accommodate symptoms. Some described value in focusing on the present moment and taking a day-by-day approach to achieving goals, while others endorsed activity pacing, self-compassion (e.g., giving themselves permission to take breaks), positive self-talk, meditation, and having a routine as valuable ways to manage symptoms in the service of working toward goals. In addition to providing a sense of accomplishment, working to accomplish goals distracted them from symptoms.
Providers recommended both medical and behavioral symptom management strategies. Medical management involved pharmacologic strategies (e.g., psychotropic medications, hormone replacement therapy, pain medications), counseling survivors early and often about possible side effects/symptoms, and referring to specialists to address specific symptoms (e.g., physical therapy for lymphedema, palliative care for pain management). Recommended behavioral symptom management strategies included normalizing and validating patients' symptom experiences, activity pacing, encouraging physical activity and a healthy diet, helping patients better utilize their support networks, providing strategies for communicating with providers, and encouraging relaxation.
Utility of the intervention and feedback on intervention structure/format
Survivors and providers were in support of developing a tailored behavioral program for YAs to address post-treatment symptoms. Both described value in a program that addressed symptoms without the need for additional medications. Survivors felt that a group-based program for YAs would provide the opportunity to meet other young survivors who understood their experiences and may be particularly beneficial for YAs who do not have a strong support network. The group format was also noted as providing the opportunity to normalize the shared experience of post-treatment symptoms and to model symptom management strategies. YAs recommended keeping the group size small to increase participants' comfort with contributing.
Due to the COVID-19 pandemic, YAs were asked for their opinions about a Zoom-based intervention. Although some preferred an in-person intervention, all were open to receiving a symptom management intervention over Zoom. They acknowledged that this delivery format may reduce participation barriers (e.g., travel time/distance, parking/transportation costs) and be particularly beneficial for YAs with high symptom burden.
Providers echoed survivors' comments regarding the utility of a group-based intervention for helping to normalize and reduce stigma around post-treatment symptoms and provide peer support. They felt that a group format would allow survivors to learn from one another in an environment with those who understood their experiences.
All participants were informed that the intervention may include a complementary mobile application and were provided with a brief description. YAs and providers had an overwhelmingly positive response regarding the inclusion of a mobile application to reinforce content delivered during intervention sessions and provide access to symptom management strategies “on the go.” Survivors acknowledged that it would be helpful to be able to ask questions of the study team and chat with other group members within the application.
Barriers to intervention participation
Multiple potential barriers to intervention participation were noted by participants. These barriers included the following: (1) competing health care-related demands for patients who were in the midst of treatment; (2) time/distance required to attend in-person sessions; (3) differences in group members' experiences that may impact their ability to relate to one another (e.g., differing cancer types, treatment histories, ages, or prognoses); (4) inconsistent or limited access to the internet or Smartphone/tablet needed to access videoconferencing sessions or the mobile application; (5) the mobile application not being compatible with Android or iPhone operating systems; and (6) other competing demands (work/school/childcare). Consideration of these barriers when developing the prototype intervention was necessary to ensure creation of an accessible intervention to address post-treatment symptoms.
Prototype intervention
Table 4 outlines how information obtained during Phase I intervention development interviews informed the prototype intervention. An eight-session, group-based, symptom management intervention was developed (Table 5). The intervention combined behavioral symptom coping skills (e.g., activity–rest cycling, relaxation training, assertive communication) and home-based physical activity (i.e., cardiovascular, strength and resistance training) with strategies from Acceptance and Commitment Therapy (ACT; e.g., cognitive defusion, working toward values), 68 strategies to foster self-compassion69,70 (e.g., loving kindness meditations), and Meaning-Centered Psychotherapy71,72 (MCP; e.g., building meaning, focusing on the legacy you live and give). Content area experts (e.g., ACT: J.P.V.; MCP: J.G.W.; physical activity: C.E. and K.M.) were consulted to ensure appropriate adaption of intervention skills to the patient population and the development of a physical activity protocol that considered survivors' post-treatment needs. The intervention was designed to occur over Zoom over 10 weeks (sessions 1–6: weekly; sessions 7–8: biweekly).
Feedback from Intervention Development Interviews and Ways Feedback Informed the Prototype Intervention
SMART, specific, measurable, achievable, relevant, time-oriented; YA, young adult.
Intervention Outline
The study team developed printed patient manuals outlining the behavioral symptom management skills and the home-based physical activity protocol, which included a week-by-week cardiovascular (i.e., walking program, walk-to-run program), resistance training, and flexibility program. In conjunction with Pattern Health, a mobile application was developed (Fig. 2) to promote skill use (e.g., session-specific exercises, push notifications with skill-use reminders), allow for accessing intervention content “on-the-go” (e.g., audio recordings of relaxation exercises), and allow for pairing with a wireless activity tracker to track daily activity. The application was designed to be relevant to YA survivors (e.g., ability to chat with group members, inclusion of Spotify playlists to use while exercising).
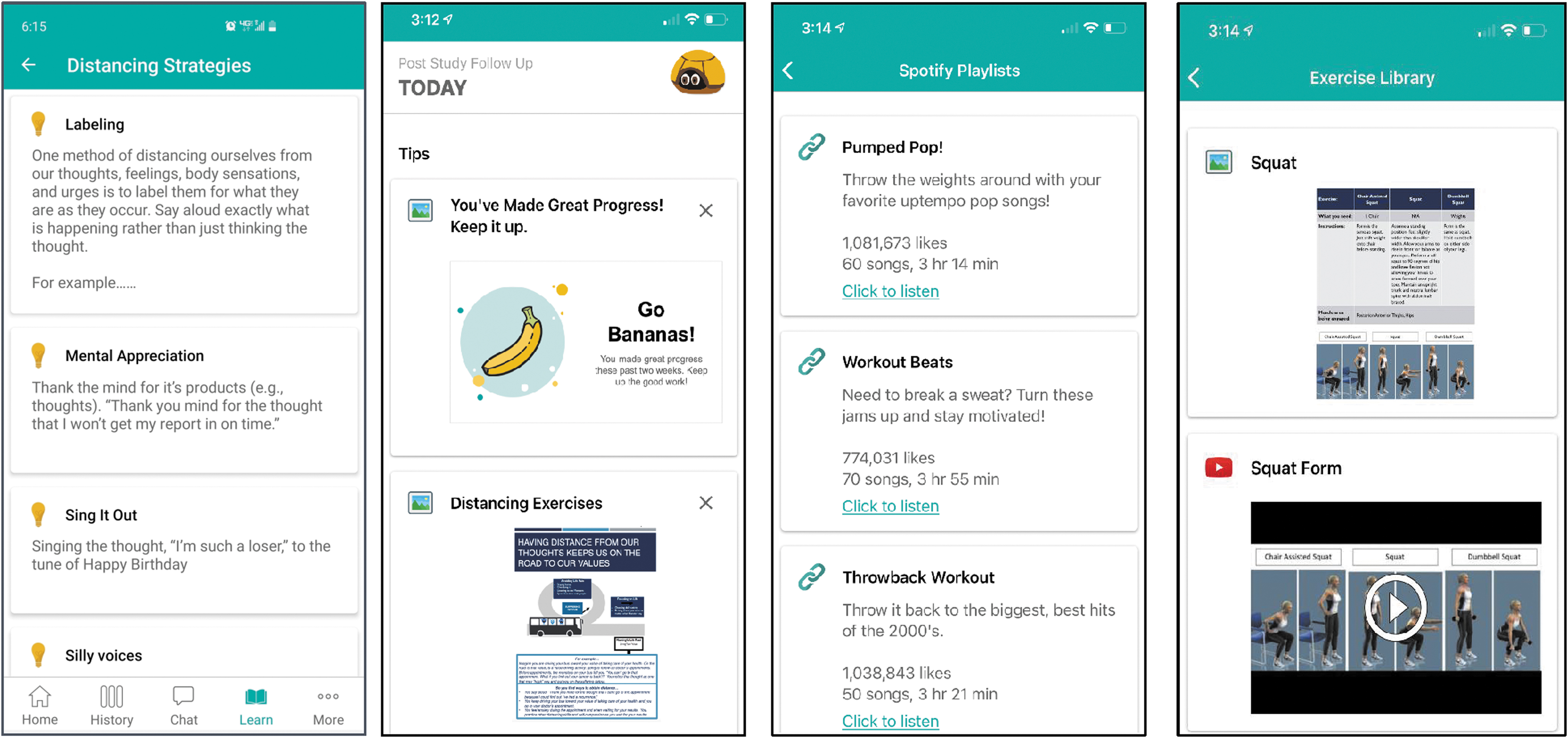
Intervention mobile application.
Informed by the Social Cognitive Theory,73,74 intervention sessions were designed to promote self-efficacy for symptom management by providing opportunities for modeling, role-plays, self-evaluation, self-monitoring, goal-setting, and receiving feedback from facilitators and group members. The proposed session format was as follows: (1) group socialization (15 minutes); (2) review of home practice and mobile application use (20 minutes); (3) provide education, skills training, and opportunities for skills practice (45 minutes); and (4) assign homework (10 minutes). This format allows for 15 minutes of casual interactions between group members to help them connect with one another. The remainder (75 minutes) of the interactive sessions include didactic, experiential, and group discussion of coping skills presented during the program.
Phase II: User testing sessions
User testers (N = 10) were supportive of the developed intervention. Based on feedback (Table 6), minor changes were made to the patient manuals and mobile application to improve the following: (1) relevance to the population; (2) intervention structure/format/layout/usability; (3) content and use of intervention skills; and (4) the program, more broadly. Feedback also informed how skills were described/introduced in the therapist manual.
Feedback from User Testers and Associated Adaptations to the Intervention and Mobile Application
AYA, adolescent and young adult.
User testers provided information about their thoughts on the utility and strengths of the proposed intervention and intervention materials. Specifically, they echoed comments provided by individuals during Phase I, highlighting the value of being able to connect with other YAs with whom they could relate to due to their shared cancer experience and developmental stage during the program. Participants also described value in integrating symptom coping skills into a group-based intervention as the group format would provide the opportunity to learn from one another about successful symptom management strategies. Individuals reviewing the printed intervention materials found the materials easy to follow, and they described specific components (e.g., call-out boxes) that helped to draw their attention to important concepts and aspects of the intervention.
Individuals reviewing the mobile application acknowledged the application's value in helping to keep intervention content at the front of their minds and as a convenient and readily accessible way to access coping skills “on-the-go.” Individuals reviewing both the printed materials and mobile application described utility in learning actionable symptom coping strategies that were then reinforced through exercises included in intervention materials.
Discussion
Post-treatment symptoms, although common, are often unaddressed for YA survivors. While prior literature suggests that YAs may feel overwhelmed by and ill-prepared to manage these long-term and late effects, 75 behavioral interventions have failed to target the unique symptom management needs of YAs. The goal of this study was to better understand the symptom experiences of YA survivors and to use this information to develop a behavioral symptom management intervention. Quantitative and qualitative data confirmed that pain, fatigue, and emotional distress were common and highly correlated post-treatment concerns for YAs. In addition, higher symptom burden was associated with lower self-efficacy for symptom management. YAs and providers acknowledged the need for and the benefit of a behavioral symptom management intervention specific to YAs to address pain, fatigue, and emotional distress.
Given the co-occurrence of pain, fatigue, and emotional distress, an eight-session, group-based intervention targeting these symptoms was developed to assist with reducing symptom severity and interference and enhancing self-efficacy for managing symptoms. By engaging both YA survivors and oncology providers in the intervention development, a program was created that resonated with the symptom experiences and needs of YA survivors and allowed for the incorporation of ways survivors might engage their providers to assist with symptom management (e.g., improving symptom communication). YA user testers reviewed the developed intervention, which allowed for further refinement of intervention content, format, and procedures to ensure applicability to YAs.
Despite its strengths (e.g., patient/provider-centered approach to intervention development/refinement), this study has limitations that might affect generalizability. (1) Five of the most common cancers among YAs were represented, which resulted in a heterogeneous sample (e.g., cancer type, treatments received). The developed intervention is broadly applicable to YAs but may not address post-treatment symptoms specific to a particular treatment/disease type. (2) The small sample size and lack of ethnic diversity may further limit generalizability. (3) Most provider participants were medical doctors; thus, the information obtained may not reflect the symptom management perspectives of other health professionals. (4) Finally, user testers participating in phase II reviewed either the printed intervention materials or the mobile application, but not both. This may have skewed feedback obtained from participants.
There are disparities in the care of YA cancer survivors when compared with childhood and older adult survivors and a need for research into the treatment of late effects of cancer, including persistent symptoms. 76 The present study further elucidates the post-treatment symptom concerns experienced by YAs and adds to the literature through the development of an intervention to address gaps in YAs' symptom management care. The developed intervention will be tested for feasibility and acceptability through a pilot randomized controlled trial.
Footnotes
Acknowledgments
We would like to thank our external advisory board members, Dr. Brandon Hayes Lattin, Dr. Ann Partridge, and Samantha Watson for their assistance with this project.
Authors' Contributions
The article has been approved by all the authors. Conceptualization: C.S.D., R.A.S., T.J.S., K.C.O., J.P.V., J.G.W., K.M., C.E., and F.J.K. Methodology: C.S.D., R.A.S., and K.C.O. Formal analysis: C.S.D. and J.M.S. Funding Acquisition: C.S.D. under the mentorship of K.C.O., R.A.S., F.J.K., and T.J.S. Investigation: C.S.D. and J.M.S. Supervision: R.A.S. and K.C.O. Writing—original draft: C.S.D. and J.M.S. Writing—reviewing and editing: R.A.S., T.J.S., K.C.O., J.P.V., J.G.W., F.J.K., J.M.S., and C.E.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Dr. Caroline S. Dorfman was supported by a career development award from the National Institutes of Health (K08CA245107).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.