
Abstract
Purpose:
Fertility preservation (FP) is becoming increasingly common among child, adolescent, and young-adult (CAYA) patients with cancer. However, Japan has long lacked definite estimates of utilization rates for FP services among CAYA patients with cancer, and little is known about disease/FP outcomes among users. Therefore, the Japan Society for Fertility Preservation (JSFP) launched the Japan Oncofertility Registry (JOFR) in 2018 and started the online registration of information regarding primary disease, FP, and data on prognosis and pregnancy outcomes. This study reports the analytical results of FP data registered in the JOFR as of 2021.
Methods:
Data about patients' primary disease(s), treatment courses, cancer and pregnancy outcomes, and specific procedures were extracted from the JOFR and analyzed.
Results:
In 2021, 1244 patients received counseling or treatment related to FP (540 males, 704 females). While the numbers of males in each age group were approximately equal, most females were aged between 31 and 40 years. In total, 490 male and 540 female patients underwent FP procedures. Leukemia, testicular cancer, and malignant lymphoma accounted for the majority of male cases seeking treatment, whereas breast cancer was the primary disease in two-thirds of the females. Since 1999, 395 patients have accumulatively experienced subsequent pregnancy.
Conclusions:
As of January 2022, >7000 cases from >100 fertility facilities have been registered in the JOFR. In the future, maintaining JOFR to disseminate information on cancer prognoses, pregnancy rates, and other oncofertility outcomes is expected to drive further expansion of oncofertility services in Japan.
Introduction
In 2017
However, compared with other countries,3–6 there are no clear statistics on how many CAYA patients with cancer undergo FP procedures. 2 Similarly, the pregnancy outcomes and cancer prognosis of patients who undergo FP remain unknown.
In Japan, the National Cancer Registry was established in 2016, and the national data on survival, recurrence, and mortality have been made available for research purposes since 2019. Meanwhile, the Japan Society of Obstetrics and Gynecology (JSOG) has launched a registry for assisted reproductive technology (ART) since 1992, 7 which has allowed for many high-impact publications of international relevance.8–11 However, the Japanese ART registry is intended to include information on oocytes and embryos only, excluding ovarian tissue or sperm. Moreover, the registry is not designed to contain information on patient background diseases, such as cancer, or to include any identifiable parameters 8 ; therefore, data linkage with other registries, including the National Cancer Registry, is impossible.
In this regard, the Japan Society for Fertility Preservation (JSFP) has established the Japan Oncofertility Registry (JOFR), for patients who have undergone FP counseling or procedures, and initiated the online registration of data on primary disease and its status, FP procedures, and pregnancy outcomes in November 2018. JOFR data are recompiled and updated once a year at each FP facility to investigate long-term outcomes (e.g., cancer treatment outcomes, the presence or absence of children, and pregnancy and childbirth outcomes).
The Ministry of Health, Labor and Welfare of Japan (MHLW) launched a project for promoting research on FP in April 2021 (“the Project” hereafter). Through the Project, FP facilities can apply for public subsidies for CAYA patients who undergo FP procedures (Tables 1 and 2). The facilities must register the patients to an updated version of the JOFR (“New JOFR”) in which National Cancer Registry data and patient-reported outcomes (PROs) are integrated.
Public Subsidies in the Ministry of Health, Labor and Welfare of Japan Project for Promoting Research on Fertility Preservation: Maximum Subsidy Amount Per Fertility Preservation Procedure
1 USD = ∼135 JPY.
Upper age limit: 42 years. Up to two times for ①, ②, ④, and ⑤, and once each for ③ at the time of tissue cryopreservation and autotransplantation.
FP, fertility preservation.
Public Subsidies in the Ministry of Health, Labor and Welfare of Japan Project for Promoting Research on Fertility Preservation: Maximum Subsidy Amount for Assisted Reproductive Technology Using Cryopreserved Specimen
1 USD = ∼135 JPY.
Up to six times when a female patient is aged ≤39 years. Up to three times when a female patient is aged 40–42 years. No subsidy when a female patient is aged ≥43 years.
ART, assisted reproductive technology.
Since the JSFP also requests that facilities register patients who do not undergo FP procedures to the “Old JOFR,” we believe the Project is serving to expand and popularize both types of the JOFR. As the New JOFR was not fully active at the time of this study, we analyzed the data registered only in the Old JOFR to elucidate the details of FP care provided in Japan as of 2021. This study will improve our understanding of the current status of oncofertility care in Japan.
Materials and Methods
The data of all patients saved in the Old JOFR through 2021 (i.e., registered by the end of January 2022) were extracted and compiled for this investigation. The JOFR data currently constitute the only available data source on FP in Japan, which has been used in this study.
The database's dictionary is shown in Table 3. The extracted data were analyzed to determine the numbers and basic information of the enrolled patients and reproductive findings and outcomes during follow-up, such as residual reproductive function and pregnancy.
Data Dictionary for the Japan Oncofertility Registry
AMH, Anti-Müllerian Hormone; JSOG, Japan Society of Obstetrics and Gynecology.
To compare the JOFR registration status across 47 prefectures, the JOFR registered cases were subdivided according to the location of the primary disease treatment facility's prefecture. The JOFR registration rate ( = number of JOFR registration cases/100,000 population) was calculated for each prefecture.
Four primary disease categories are eligible for public funding under the Project:
Treatments classified as high, intermediate, or low risk in the infertility risk hierarchy specified in the JSCO's Clinical Practice Guidelines for Fertility Preservation for CAYA Cancer Patients. Cancers in which long-term treatment is expected to reduce ovarian reserve, such as breast cancers (hormone therapy). Noncancerous disorders treated by hematopoietic stem cell transplantation, such as aplastic anemia, inherited bone marrow failure syndromes (e.g., Fanconi's anemia), primary immunodeficiency syndrome, congenital metabolic disorders, thalassemia, sickle cell disease, chronic active Epstein-Barr virus infection. Noncancerous diseases treated by alkylating agents, such as systemic erythematosus, lupus nephritis, polymyositis/dermatomyositis, and Behcet's disease.
One new addition to the New JOFR is an electronic platform for PROs called “ePRO,” through which enrolled individuals can update their records using their smartphones. This setup allows both patients and health care providers to furnish and verify the JOFR data regarding patients' general health status and reproductive function, including pregnancy outcomes (Fig. 1). Patients who received counseling or FP procedures before April 2021 or those who did not undergo any FP procedure were registered in the Old JOFR. Both Old and New JOFR are integrated in the updated registry system, called the JOFR-II, which has been fully operational since August 2022.

Old and New JOFR system. JOFR, Japan Oncofertility Registry.
Our study was conducted in compliance with Ethical Guidelines for Medical and Health Research Involving Human Subjects (MHLW), laws protecting personal information, and related guidelines. Patient data were input by FP facilities approved by the JSOG or Japanese Urological Association. Each JOFR facility was approved by its institutional review board or the clinical research ethics committee of Tohoku University Hospital. Generally, patients need to provide written consent and assent to be enrolled in the JOFR. Some patients who received counseling or FP procedures but had since died or who could not be reached to obtain consent were included in the Old JOFR, under the condition that public notice of the opt-out option and other study details were listed on the websites of the JSFP and JOFR facilities.
Results
In total, data from 7721 patients enrolled in the JOFR database were analyzed (3291 males, 4195 females, and 235 unknown). Figure 2 shows the number of patients registered, between 2006 and 2021, by year of first visit to each JOFR facility. At present, the JOFR database has 138 contributing facilities.
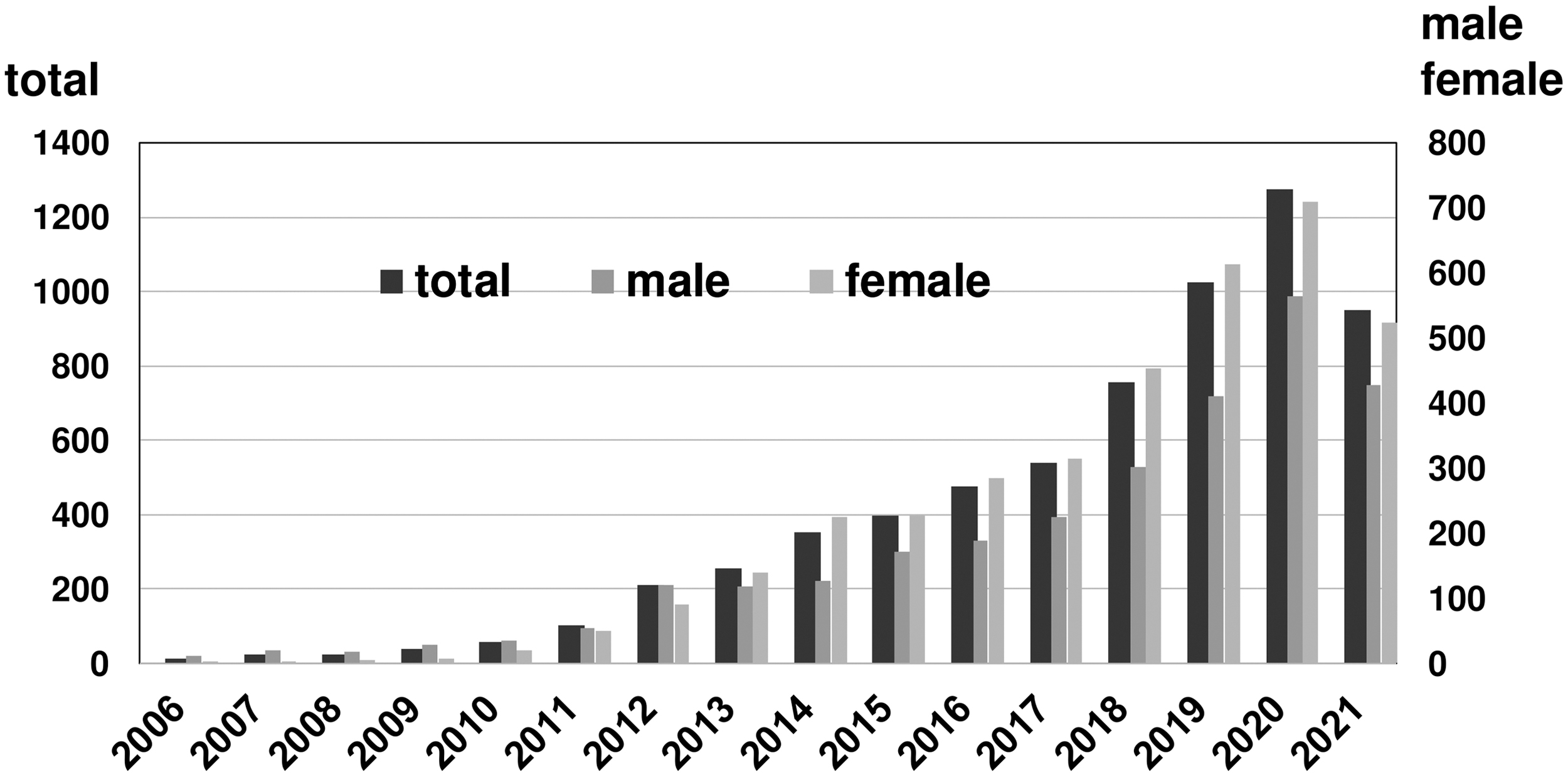
Patient enrollment in the JOFR by year.
In 2021, 1244 patients received counseling or FP procedures (540 males, 704 females). Table 4 shows the number of patients provided with each FP procedure. In total, 490 male (90.7%) and 540 female (76.7%) patients underwent an FP procedure in 2021. The age distribution of the survey conducted among participants who underwent FP procedures revealed that the number of males in each age group was comparable; meanwhile, the largest number of females occurred between the ages of 31 and 40 years (Supplementary Fig. S1).
Details of Patients Registered in the Japan Oncofertility Registry in 2021 (540 Males, 704 Females)
TESE, testicular sperm extraction.
Three categories of primary disease accounted for most male cases—leukemia, testicular cancer, and malignant lymphoma; however, breast cancer was the primary disease in two-thirds of female cases (Fig. 3). Among the total of 7721 JOFR registered patients, 395 experienced subsequent pregnancy (Table 5).

Details of Pregnancies Registered in the Japan Oncofertility Registry (n = 395)
JOFR, Japan Oncofertility Registry.
Patient data from the JOFR could be gathered from 46 of 47 prefectures. Among the 46 prefectures, 4 had a registration rate of >10, 9 prefectures between 5 and 10, 24 prefectures between 1 and 5, and 9 prefectures <1 per 100,000 population (Supplementary Fig. S2). The results showed that there were large differences in the number of people registered depending on the primary disease treatment facility's prefecture.
A statistical analysis was also performed to compare background data between the cases who underwent FP and those who did not in 2021. FP was chosen significantly more in male patients (p < 0.001) and new-onset primary disease (p < 0.001), irrespective of average age (p = 0.2708), number of experience of [partner's] of pregnancies (p = 0.7954), or presence of partner (p = 0.3631) (Table 6). No significant differences in FP rates were found in 2021 by the primary disease treatment facility's prefecture (Supplementary Fig. S3).
Statistical Analysis Comparing Background Data Between Cases With and Without Fertility Preservation in 2021
Blank data are excluded.
The most common reason for not performing FP, which was presumed by health care providers in the FP facilities, was “Medically contraindicated,” such as poor performance status and no enough time for FP (14%), followed by “Unwilling to have children in the future” (12%), although the reason in 69% of the cases without FP was unknown (Supplementary Table S1).
Discussion
In 2017, the JSCO issued Clinical Practice Guidelines (GPGs) for FP in CAYA patients with cancer.1,12 In their CPGs published the same year, the JSOG assigned a Grade B-evidence rating to the recommendation, “Refer AYA cancer patients wishing to freeze oocytes or embryos to an assisted reproductive technology (ART) provider who can accommodate them.” “Building systems for referring patients to suitable ART hospitals/clinics” is a designated national obligation in the third Cancer Control Promotion Basic Plan, adopted by Cabinet decision in March 2018. Organizing guidelines for designated cancer care hospitals were revised in July 2018 based on this document.
Several foreign databases served as important models for the JOFR. The Project is preceded by FertiPROTEKT, an oncofertility network established in 2006. As of 2015, this network comprised of 101 member centers across three countries: Germany, Switzerland, and Australia. 13 In 2011, the network issued guidelines for the cryopreservation of ovarian tissue, in addition to oocytes 14 ; by 2015, member centers had frozen >500 unfertilized and fertilized eggs each, and performed >2500 ovarian cryopreservation procedures. Details regarding the procedures and outcomes of oncofertility patients in Australia are being recorded and analyzed in the Australasian Oncofertility Registry.13,15,16 Established in 2006, the Oncofertility Consortium runs a wide variety of interdisciplinary projects in the United States, ranging from basic research on oncofertility to clinical medicine and sociology. 17
In addition, the FUTuRE Fertility research team has established the first bilateral, multicenter Australian Oncofertility Registry, which is expected to improve FP in Australia and New Zealand by collecting prospective fertility follow-up data from all registered patients to determine postcancer treatment short- and long-term reproductive function based on cancer type, treatment type, and age at diagnosis.13,18 Furthermore, the number of FP cases is increasing in Europe 19 ; however, wide acceptance of FP remains a problem.
Approximately 20,000 adolescents and young adults aged 15–39 years are diagnosed with new cancer every year in Japan 20 ; however, our knowledge and framework for preserving fertility among this “AYA generation” remain weak and underdeveloped. Health care providers must develop and provide oncofertility services based on information related to patients' primary disease and FP, as well as treatment plans related to cancer and pregnancy outcomes; these critical challenges must be addressed as a matter of national policy.2,21–25
In this study, we sought to explore the details of FP care provided in Japan in 2021. Our study counted a cumulative total of 395 pregnancy cases in the JOFR. While embryo cryopreservation is usually provided to married patients, procedures for freezing eggs, sperm, and ovarian tissue are provided to unmarried people. Using the New JOFR cooperated with ePRO, further analysis is needed to determine how many patients have thus far attempted to conceive and used their frozen specimens for calculating the success rate of each FP procedure.
Related works include a nationwide survey of sperm cryopreservation providers, which included 820 patients with cancer who underwent the procedure between April 2015 and March 2016, 22 as well as a nationwide survey on FP procedures among female patients with cancer, Japan's first ever, which included 1085 cases of oocyte and embryo cryopreservation, and 122 cases of ovarian tissue cryopreservation between 2011 and 2015. 26 A 2016 research project by the MHLW reported that many FP facilities set upper age limits for FP services (e.g., 40–41 years for oocyte/ovary cryopreservation and 44–45 years for their use). It was also noted in Japan that FP procedures resulted in very few childbirths, and no records of live births resulting from cryopreserved ovarian tissue were found. 27 Compared with these previous reports, the size of our analysis population (490 males and 540 females in 2021) suggests increasing utility rates of oncofertility services for both sexes (Fig. 2).
Sperm cryopreservation is not expensive compared with oocyte/embryo/ovarian tissue cryopreservation, and ineffective enrollment incentives by public funding have been longstanding issues. Nonetheless, both female and male registrants have increased dramatically since our report on JOFR enrollment in 2019, 28 and we expect registrations to increase further following the implementation of the Project in April 2021.
In 2021, three categories of primary disease accounted for most male cases—leukemia, testicular cancer, and malignant lymphoma—while breast cancer was the primary disease in two-thirds of females. These findings are consistent with breast cancer's position as the most common cancer among Japanese females. 29 Among the >7000 cases accumulated since 2006, we noted 395 cases of subsequent pregnancy. Cases of livebirths after ovarian tissue cryopreservation and autotransplantation, which could not be confirmed in Japan previously, were also confirmed. 30
However, this information is based on the data currently present in the JOFR. Assuming that the number of CAYA cancer patients per population varies little by prefecture, the results of this study suggest that the chances of CAYA cancer patients receiving oncofertility care vary greatly by prefecture. In other words, JOFR registration rate may reflect the activity of regional oncofertility network in each prefecture.31,32
The results of our statistical analysis for background data between patients with and without FP showed that FP was significantly more preferred by male patients than by female patients, and in patients with a newly diagnosed primary disease than those with recurrent disease (Table 6). This may be because cryopreservation is easier to perform for sperm than for oocytes, embryos, and ovarian tissue, and because primary disease treatment is more likely to be prioritized in recurrent cases.
Since it would be psychologically burdensome to ask the patients themselves to answer why they did not choose FP, the answers were given by the health care providers who provided the counseling. Unfortunately, 69% of the respondents could not give a reason. However, similar to the results of the statistical analysis described above, our results suggest that the status of the patient's primary disease influences the choice of FP.
The Project receives public funding from national and prefectural sources sponsoring various types of FP procedures. One of its goals is to establish clinical evidence in support of these procedures. Hence, in addition to receiving authorization to participate in their prefectural oncofertility network, FP facilities are required to perform long-term follow-ups and update the JOFR database at least annually with information on patient cancer, pregnancy, and childbirth outcomes.
The Project also established a new online registry, that is, the New JOFR, which is an expansion of the Old JOFR, and developed an associated ePRO platform to allow enrolled patients to update the database directly with relevant information, such as their general health and pregnancy status, through a smartphone application—“FS (Fertility & Survivorship) Link.” The New JOFR will provide information not only about the treatment status of the primary disease but also the patient's contact details (home and email address), the status of sexual and reproductive health, childbearing plan (including adoption or foster care programs), and detailed information about pregnancy and delivery, constructed by both patient and health care provider (Supplementary Table S2).
In the future, we plan to augment the data stored in the JOFR by linking it with the National Cancer Registry data (Fig. 1). The New JOFR has improved the granularity of the input data, allowing sophisticated metrics to be evaluated; these include the percentages of cases who used frozen specimens (eggs, sperm, etc.) that resulted in pregnancy and/or childbirth (efficacy), and primary disease outcomes among users of different FP services (safety).
Over time, these data will provide insights that can be incorporated into periodic updates of FP guidelines. However, our patient reporting platform has still some challenging issues related to data security, including personally identifiable information (e.g., full name, home address), private, sensitive information (e.g., cancer status and treatments, sexual activity), and data accuracy (i.e., patient-reported input is considered the most accurate). The Project could also use technical support (such as a helpdesk) and provide alternative methods of data entry (helpdesk and paper forms, for instance). Options could also be given regarding data collection preferences, and to mitigate the psychological burden associated with questions (e.g., by including a “Don't Want to Answer” option).
Other issues include the small financial incentive available for sperm cryopreservation (Tables 1 and 2), and resistance from some patients to disclose their name or address. Gaining patients' understanding and cooperation by making sure that beneficial features of the smartphone app are part of their user experience (e.g., permitting patients to check and revise the information in the registry, reducing the administrative burden of applying for financial assistance, notifications related to updated procedures at FP/ART providers, and showing oncofertility-related information) will be essential to increasing user adoption.
In addition, many anticancer drugs not listed in the guidelines are currently prescribed in Japan, as in Europe and the United States, without sufficient evidence regarding the risk of amenorrhea. It may be possible, someday, to obtain more detailed evidence on the effects of anticancer drugs and regimens on reproductive function by tracking infertility outcomes in the JOFR. 33
Conclusion
Continuing to maintain the Old and New JOFR databases to disseminate information on prognoses, pregnancy rates, and other oncofertility outcomes in Japan will contribute to the further expansion of oncofertility services in the country.
Footnotes
Acknowledgments
We extend our deepest thanks to those involved in the JSFP Registration Committee Secretariat (Yoshiko Tsukiyama and Yuko Umezawa) and FP facilities who contribute to building the JOFR.
Authors' Contributions
Authors Disclosure Statement
No competing financial interests exist.
Funding Information
This study was sponsored by a 2020 grant-in-aid from the Comprehensive Research Project for Raising a Healthy Next Generation (Ministry of Health, Labour and Welfare): Integrated Research to Support and Spread the Preservation of Reproductive Function via Medical Adaptations (19DA0501).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.